Pressure Ulcer Prevention and Management - Sydney South West ...
Pressure Ulcer Prevention and Management - Sydney South West ...
Pressure Ulcer Prevention and Management - Sydney South West ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Policy Directive<strong>Pressure</strong> <strong>Ulcer</strong> <strong>Prevention</strong> <strong>and</strong> <strong>Management</strong>Document No:Functional Sub-Group:Summary:Approved by:SSW_PD2008_008Corporate GovernanceClinical GovernanceGuidelines for the prevention <strong>and</strong> management ofpressure ulcers in conjunction with the Warterlow RiskAssessment <strong>and</strong> <strong>Management</strong> Tool.Ms Kerry Russell, Area DON&MS(Endorsed by: Area Clinical Quality Council & NursingExecutive Committee)Publication (Issue) Date: March 2007Next Review Date: April 2010Replaces Existing Policy:Previous Review Dates:N/AN/ANote:<strong>Sydney</strong> <strong>South</strong> <strong>West</strong> Area Health Service (SSWAHS) was established on 1 January 2005 withthe amalgamation of the former Central <strong>Sydney</strong> Area Health Service (CSAHS) <strong>and</strong> the former<strong>South</strong> <strong>West</strong>ern <strong>Sydney</strong> Area Health Service (SWSAHS).In the interim period between 1 January 2005 <strong>and</strong> the release of single Area-wide SSWAHSpolicies (dated after 1 January 2005), the former CSAHS <strong>and</strong> SWSAHS policies wereapplicable as follows:-• SSWAHS Eastern Zone : CSAHS• SSWAHS <strong>West</strong>ern Zone: SWSAHSCompliance with this policy directive is m<strong>and</strong>atory Page 1 of 20
<strong>Sydney</strong> <strong>South</strong> <strong>West</strong> Area Health ServicePolicy No: SSW_PD2008_008Date Issued: January 2008PRESSURE ULCER PREVENTION AND MANAGEMENTCONTENTS1. Introduction1.1 Risks – Clinical1.2 Aims / Expected Outcomes2. Policy Statement3. Principles / Guidelines3.1 Background3.2 Guidelines3.2.1 Risk Assessment <strong>and</strong> documentation for all Patients WITHOUT a<strong>Pressure</strong> <strong>Ulcer</strong>3.2.2 Risk Assessment <strong>and</strong> Documentation for all Patients WITH a <strong>Pressure</strong><strong>Ulcer</strong>3.2.3 <strong>Pressure</strong> <strong>Ulcer</strong> <strong>Prevention</strong> Strategies3.2.4 Maintenance of Skin Integrity3.2.5 Repositioning Intervals according to pressure devices classification3.2.6 Training <strong>and</strong> Education4. Performance Measures4.1 Monitoring <strong>and</strong> Ongoing Reporting of <strong>Pressure</strong> <strong>Ulcer</strong>s4.2 Monitoring <strong>and</strong> Evaluation5. Definitions6. ReferencesAppendix 1:Appendix 2:Appendix 3:Appendix 4:Appendix 5:Appendix 6:Appendix 7:Waterlow <strong>Pressure</strong> <strong>Ulcer</strong> Risk AssessmentWaterlow <strong>Pressure</strong> <strong>Ulcer</strong> <strong>Management</strong>Summary of <strong>Prevention</strong> Strategies<strong>Pressure</strong> <strong>Ulcer</strong> GradesIntervention GuidelinesDevicesClassification of DevicesCompliance with this policy directive is m<strong>and</strong>atory Page 2 of 20
<strong>Sydney</strong> <strong>South</strong> <strong>West</strong> Area Health ServicePolicy No: SSW_PD2008_008Date Issued: January 2008• Interventions are to be documented <strong>and</strong> based on the SSWAHS<strong>Pressure</strong> <strong>Ulcer</strong> <strong>Prevention</strong> <strong>and</strong> <strong>Management</strong> Policy InterventionGuidelines (Appendix 3 & 4).• Pain management must include adequate analgesia as appropriate.• Strategies implemented to promote pressure ulcer healing <strong>and</strong>prevent further breakdown must be documented in the patient /client’s health care record.• Current risk assessment, existing pressure ulcers of all grades <strong>and</strong>presence of pressure relieving devices are to be documented in thepatient / client’s health care record on transfer or discharge.• Implement appropriate prevention strategies as per Waterlow<strong>Pressure</strong> <strong>Ulcer</strong> <strong>Management</strong> Flowchart (Appendix 2)• All existing pressure ulcer must be reviewed <strong>and</strong> documented on thepatient/client’s discharge summary3.2.3 <strong>Pressure</strong> <strong>Ulcer</strong> <strong>Prevention</strong> Strategies<strong>Pressure</strong> injury prevention strategies, directed at reducing or modifyingpressure ulcer risk factors, should be incorporated into the patient / client’smanagement plan. All patients identified ‘at risk’ should have a plan of carethat incorporates measures such as pressure support systems, positioning,skin care <strong>and</strong> nutritional interventions. These strategies include:(i)(ii)(iii)(iv)maintenance of skin integrity;minimisation of pressure, shear <strong>and</strong> friction;implementing pressure relieving positions <strong>and</strong> a pertinent turningschedule, including repositioning intervals; <strong>and</strong>provision of an appropriate support surface.3.2.4 Maintenance of Skin IntegrityMaintaining the integrity of the patient / clients skin is the key to anyprevention program. As skin has a normal pH of 4-6.8, the skin’s acidity,normal flora <strong>and</strong> the natural anti-bacterial substances found in sebum delaymicro-organism growth. Maintaining a stable skin pH discourages thecolonisation of bacteria <strong>and</strong> reduces the risk of opportunistic infection.Patients at risk should have a skin inspection daily, or more often ifwarranted, paying particular attention to skin over bony prominences <strong>and</strong>weight bearing areas. A systematic inspection is integral to the earlyidentification of skin damage <strong>and</strong> provides a baseline for care planning <strong>and</strong>evaluating interventions. Actions to maintain skin integrity include:(i)Routinely Assess Skin:• Conduct a skin assessment on admission <strong>and</strong> at regularintervals, especially skin over bony prominences which is notdesigned to support sustained external pressure eg. Sacrum,heels <strong>and</strong> greater trochanters.Compliance with this policy directive is m<strong>and</strong>atory Page 6 of 20
<strong>Sydney</strong> <strong>South</strong> <strong>West</strong> Area Health ServicePolicy No: SSW_PD2008_008Date Issued: January 2008• Assess patients carefully for compromised peripheral circulation<strong>and</strong> diabetes.• Use vigilance to assess patients with casts, traction <strong>and</strong> supportstockings.• Document pre-existing ulcers in the patient / client health carerecord in terms of location, severity, size, description of ulcer<strong>and</strong> surrounding skin.(ii)Prevent Exposure to Excessive Moisture or Dryness:• Implement continence training with toileting / bowelmanagement regimes where applicable.• Minimise skin exposure to urine or faeces, excessive sweatingor wound drainage as these can increase the pH of the skincausing chemical damage, maceration <strong>and</strong> denuding of the skin.• Consider medical assessment (eg. medication review) for highrisk patients to manage reversible cases of incontinence.(iii) Promote Optimal Skin Hygiene:• Cleanse the skin gently to improve overall hygiene <strong>and</strong> stimulatecirculation.• Treat dry skin with appropriate moisturising creams.• Avoid vigorous rubbing or massaging over bony prominences.(iv) Promote Optimal Nutrition:• Encourage a balanced diet to provide adequate protein <strong>and</strong>caloric requirements.• Assess nutrition <strong>and</strong> hydration <strong>and</strong> other indicies of nutritionalstate, eg. body weight loss, muscle wasting or any signs ofvitamin or mineral deficiencies.• Consult a dietician when nutritional deficits compromise tissueintegrity.(v)Minimisation of <strong>Pressure</strong> Shear <strong>and</strong> Friction. Damage to the skin iscaused by pressure, shearing forces or friction, or a combination ofthese:• Patients / clients who are immobile, inactive <strong>and</strong> elderly are atgreatest risk.• Skin assessment is critical in providing an indication of the skin’stolerance to pressure shear <strong>and</strong> friction.• Correct positioning, transferring <strong>and</strong> h<strong>and</strong>ling techniques shouldbe employed(vi) Protect Against the Forces of Shear <strong>and</strong> Friction:• Use aids that eliminate dragging <strong>and</strong> friction eg. Hoists, slidesheets, slide boards <strong>and</strong> slings.• Take care when transferring patients / clients between bed <strong>and</strong>chair• Avoid the overuse of plastic sheets / kyliesCompliance with this policy directive is m<strong>and</strong>atory Page 7 of 20
<strong>Sydney</strong> <strong>South</strong> <strong>West</strong> Area Health ServicePolicy No: SSW_PD2008_008Date Issued: January 2008• Avoid shearing forces by using profiling beds <strong>and</strong> / or notelevating the head of the bed more than 30 degrees (asappropriate to the patient / clients clinical condition)(vii) Reduce Heel <strong>Pressure</strong>:• Protect heels against pressure injury, particularly those patient /clients confined to bed or with immobilised lower extremities.• Prevent constriction of the foot by tight or heavy bed linen withaid of a bed cradle.(viii) Promote Activity <strong>and</strong> Mobility:• Maximise activity <strong>and</strong> mobility status consistent with patient /clients medical condition <strong>and</strong> ability eg. Encourage earlymobilisation following surgery or stroke.• Use assist devices with active rehabilitation <strong>and</strong> earlyambulation to relieve pressure from stressed or damaged tissue<strong>and</strong> improve circulation eg. Trapeze, rollator, cane or walker.(ix) <strong>Pressure</strong> Relieving Positions:• Specific attention should be paid to patients / clients in bedassessed to be ‘at risk’ for pressure ulcer development.• A care plan for systematically turning <strong>and</strong> repositioning thepatient should be developed that includes the use of positioningaids <strong>and</strong> pressure devices to relieve pressure from bonyprominences.• Repositioning schedules should consider the patients medicalcondition <strong>and</strong> comfort level.• Positioning frequency is based on skin inspection <strong>and</strong> should beincreased if skin discolouration is evident.(x)<strong>Pressure</strong> Repositioning Intervals:• When patients are unable to move themselves <strong>and</strong> relieve thepressure, clinical staff must intervene <strong>and</strong> reposition the patientregularly, being careful to eliminate any shearing forces to otherareas of skin eg. dragging heels along the sheet. Appropriatelifting aids <strong>and</strong> manual h<strong>and</strong>ling equipment must be used at alltimes.• The frequency of repositioning is dependent on the individualpatient / clients skin’s tolerance to pressure. The repositioningschedule should consider the patient/client’s medical condition,comfort, overall plan of care as well as the support surface used.Repositioning decreases the time a patient / client spends in oneposition <strong>and</strong> pressure relieving devices reduce pressureintensity• Reposition the patient more frequently if sitting up <strong>and</strong> / or use amore efficient support system if the patient / clients skin colourchanges. Conduct a skin inspection of all pressure points todetermine the effectiveness of the repositioning scheduleCompliance with this policy directive is m<strong>and</strong>atory Page 8 of 20
<strong>Sydney</strong> <strong>South</strong> <strong>West</strong> Area Health ServicePolicy No: SSW_PD2008_008Date Issued: January 20083.2.5 Repositioning Intervals According to <strong>Pressure</strong> Devices Classification (forpressure relief)Product descriptionFoam replacementmattressesContoured surfaces ordifferent density foamsVery high risk( 20+ )Patient risk categoryHigh risk( 15+ )At risk( 10 )1 hour 2 hours 3 hoursStatic air-filledmattresses 2 hours 3 hours 4 hoursAlternating pressureoverlays2 Cell CycleAlternating pressuremattresses2 Cell CycleAlternating pressuremattress3 cell cycle4 hours 5 hours 6 hours6 hours 8 hours 8 hours8 hours 8 hours 8 hours3.2.6 Training <strong>and</strong> EducationTraining <strong>and</strong> education programs for the prevention of pressure ulcers shouldbe structured, organised <strong>and</strong> comprehensive. They should be directed at alllevels of health professionals, patients / clients, families <strong>and</strong> carers involvedin patient / client management. The basic education should include thefollowing content:• Patient / Client assessment;• Aetiology <strong>and</strong> risk factors;• Risk assessment tools <strong>and</strong> their application;• Uniform staging classification;• Skin assessment <strong>and</strong> skin care;• Selection of appropriate pressure redistributing equipment;• Implementation of an individualised management program whichincludes discharge planning needs; <strong>and</strong>• Positioning / h<strong>and</strong>ling techniquesIn addition education should also focus on:• Principles of wound healing <strong>and</strong> product selection;• Relevant policies <strong>and</strong> procedures;• Documentation of relevant data;• Clinical audit processes of preventative <strong>and</strong> therapeutic interventions;• Clinical governance which includes commitment to <strong>and</strong> availability ofeducation <strong>and</strong> training;• Where to get further advice eg. Resource persons in organisation;<strong>and</strong>Compliance with this policy directive is m<strong>and</strong>atory Page 9 of 20
<strong>Sydney</strong> <strong>South</strong> <strong>West</strong> Area Health ServicePolicy No: SSW_PD2008_008Date Issued: January 20084. Performance Measures• Roles <strong>and</strong> responsibilities of the multidisciplinary team.4.1 Monitoring <strong>and</strong> Ongoing Reporting of <strong>Pressure</strong> <strong>Ulcer</strong>sIf a patient / client is identified as having a pressure ulcer the following mustoccur:(i)(ii)(iii)(iv)(v)A notification in the patient / client healthcare record via the pink notificationsticker must occur after the incident is notified in IIMS;Each month on a nominated day a prevalence audit is to be conducted bythe Nursing Unit Manager (NUM) or delegate. The results of this audit areto be sent to the Quality Unit <strong>and</strong> copies of the audit are to be kept by theNUM as evidence;The Quality Unit will then generate a monthly report for distribution to eachNursing Unit Manager, Department Head & Clinical Manager in order toupdate <strong>and</strong> monitor the pressure ulcer status of each patient / client with adocumented pressure ulcer;The Quality Unit will generate a trended monthly report from the aggregateddata; <strong>and</strong>Bi-Annually Clinical Nurse Consultants will conduct a prevalence audit of allpatients in the facility.Incidence <strong>and</strong> prevalence of pressure ulcers by site, grade <strong>and</strong> intervention mustbe reported <strong>and</strong> discussed at the appropriate local clinical meetingMonthly aggregated reports are to be directed to the Facility Director of Nursingor Community Health Director of Nursing.An aggregated quarterly report from each Facility <strong>and</strong> Community Health QualityUnit indicating incidence <strong>and</strong> prevalence of pressure ulcers by site, grade <strong>and</strong>intervention must be tabled at the SSWAHS Nursing Clinical Practice CommitteemeetingAny incidence of grades 1 - 4 pressure ulcer must undergo a SeverityAssessment Code score in IIMS.Aggregated monthly incidence <strong>and</strong> prevalence rates on grade <strong>and</strong> site of allpressure ulcers are to be presented to relevant teams <strong>and</strong> committees.Identification of any contributing factors <strong>and</strong> recommendations on strategies toreduce the incidence are to be recorded <strong>and</strong> implemented with minimal delay.Review of the effectiveness of the strategies <strong>and</strong> actual outcomes is to beassessed <strong>and</strong> recorded by teams <strong>and</strong> relevant committees.4.2 Monitoring <strong>and</strong> EvaluationNursing managers are responsible for maintaining high st<strong>and</strong>ards of care <strong>and</strong>ensuring the resources, educational programs <strong>and</strong> audit systems are in place tosupport an effective pressure ulcer prevention <strong>and</strong> management program.Regular evaluation is part of an ongoing process of monitoring <strong>and</strong> assessing.The monthly clinical audit forms an integral part of the organisations qualityCompliance with this policy directive is m<strong>and</strong>atory Page 10 of 20
<strong>Sydney</strong> <strong>South</strong> <strong>West</strong> Area Health ServicePolicy No: SSW_PD2008_008Date Issued: January 2008improvement plan. The principles <strong>and</strong> process ensure that agreedoutcome measures are achieved. <strong>Pressure</strong> ulcer monitoring must include:• Monthly incidence reports both at clinical <strong>and</strong> organisational level• Monthly clinical pressure ulcer prevalence audits5. DefinitionsBlanching Hyperaemia - reddened areas turn white following application of fingerpressure; this indicates that the microcirculation is intact.Epithelialisation - regeneration of the epidermis across the wound surface.Erythema - redness of the skin surface caused by vasodilation.Eschar - brown or black necrotic tissue.Exudate - any fluid that has exuded out of a tissue or its capillaries because of aninjury or inflammation <strong>and</strong> is high in protein <strong>and</strong> white cells.Friction - a force created by two surfaces in contact moving across each other.Granulation - healing tissue composed of newly formed capillaries <strong>and</strong> fibroblasts.Incidence - the frequency of occurrence of any event or condition over a period oftime <strong>and</strong> in relation to the population in which it occurs, as an incidence of a disease.Ischaemia - deficiency of blood, due to obstruction or constriction of a blood vessel.Necrosis - death of tissue.Non-blanching Hyperaemia - persistent redness when finger pressure is applied toan area of reactive hyperaemia indicating disruption to the microcirculation.<strong>Pressure</strong> - a perpendicular load or force.<strong>Pressure</strong> Reducing Support Surfaces - support surfaces that maintain tissueinterface.<strong>Pressure</strong> Support Surfaces - support surfaces that maintain tissue interface pressure<strong>Pressure</strong> <strong>Ulcer</strong> - an area of localised tissue damage caused by unrelieved pressure,friction or shear. <strong>Pressure</strong> ulcers occur most commonly on the sacrum <strong>and</strong> heel butcan develop anywhere on the body including the coccyx, occiput, clavicle, ear <strong>and</strong>nose. Other terms for a pressure ulcer are pressure sore, bedsore <strong>and</strong> decubitus ulcer.Prevalence - the number of existing cases of a particular disease or condition in agiven population at a designated time.Reactive Hyperaemia - a normal compensatory mechanism following an episode ofreduced skin perfusion to the tissues as a result of pressure. Relief of pressure resultsin reddening of skin caused by blood returning back into ischaemic tissues.Compliance with this policy directive is m<strong>and</strong>atory Page 11 of 20
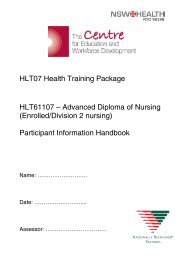
Appendix 1Waterlow <strong>Pressure</strong> <strong>Ulcer</strong> Risk Assessment ToolCircle scores in the table below <strong>and</strong> calculate the total to obtain risk score. (Several scores per category can beused).Has the patient previously had a pressure ulcer? Yes □ No □Has this pressure ulcer been entered into IIMS? Yes □ No □Sex/Age Build/Weight for Height (BMI) Special RisksMaleFemale14-4950-6465-7475-8081+12123450Average (20-24.9)Height (m) 2Above average (25-29.9)1Obese >302Below average 4hrs ## - scores can be discounted 48hrspost op provided pt is recoveringnormallyCytotoxinsSteroidsAnti-inflammatory(max score 4)Malnutrition Screening Tool (MST) – circle <strong>and</strong> add for a totalB. How much weight has the ptlost?Go to question BGo to question CScore 2 <strong>and</strong> go to C0.5-5kg5-10kg10-15kg>15kgUnsure12342MedicationsC. Has the pt been eating poorlybecause of a decreased appetite?NoYesTotal MalnutritionScoreIf the patient’s malnutrition screening score is 2 or more pleaserefer pt to a dietician.Total WaterlowScoreDate Referred:Signature:(total all scores +MST score)Waterlow <strong>Pressure</strong> <strong>Ulcer</strong> Risk 10+ At risk 15+ High Risk 20+ Very High Risk© J Waterlow 1985 Revised 20050184
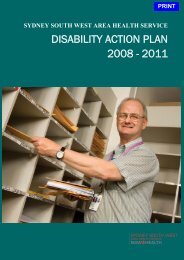
Appendix 2Waterlow <strong>Pressure</strong> <strong>Ulcer</strong> <strong>Management</strong> FlowchartNOT AT RISK < 10AT RISK 10+HIGH RISK 15+VERY HIGH RISK 20+PRESSUREULCERNo managementunless change inconditionWaterlow assessmentto be completed everyweek or morefrequently if change inconditionDocument in thepatient/client healthcare record <strong>and</strong> on thecare planIdentify level of riskManage as perprevention strategiesChoose a pressuresupport system accordingto the level of risk(Appendix 4)Dietician referral to assessthe patient/clients nutritionalstatus & dietaryrequirementsWaterlow assessment to becompleted every week ormore frequently if change inconditionEnter into IIMS. Whenappropriate contact woundcare specialistDocument in thepatient/client health carerecord <strong>and</strong> on the woundmanagement chartChoose a pressuresupport system accordingto the level of risk(Appendix 4)Dietician referral to assessthe patient/clients nutritionalstatus & dietaryrequirements & hydration<strong>Pressure</strong> ulcer woundmanagement as pertreatment protocolsContact wound carespecialist for advice &assistance re pressureulcerReview ulcer at eachdressing change. Documentin health care record woundmanagement chartDocument in thepatient/client health carerecord <strong>and</strong> on the careplanAny patient/client with agrade 3-4 pressure ulcer isto remain at High Risk fortheir entire admissionService required Date contacted SignatureEntered into IIMS YES NOEquipment Hire required YES NOCompany contacted YES NOWound Care Specialist YES NODietician YES NOInterventional strategies implemented:PLEASE NOTE: Any patient that has suffered a Stage 3 or 4 pressure ulcer in the past is ‘At Risk’ of developinganother <strong>and</strong> is to be treated as HIGH RISK throughout their entire admission
Appendix 3Summary of <strong>Prevention</strong> Strategies• Assess all patients/clients using the Waterlow <strong>Pressure</strong> <strong>Ulcer</strong> Risk Assessment Tool• Assess the patient/clients nutrition, function, continence <strong>and</strong> general medical condition• Involve all relevant members of the multi-disciplinary team• Initiate the following interventions <strong>and</strong> evaluate the outcomesMaintain skinintegrityEliminatepressure, shear& frictionInitiatepositioning, turnschedule &support surfaceDocument &communicateConduct a dailysystematic skininspection of ‘at risk’patients for signs ofimpaired skin integrityEliminate orminimise allpotentially irritatingskin substancesStabilise skin &body temperaturePromotecontinenceassessment/training & self careindependenceAvoid direct contactbetween bonyprominences with pillowsor foam wedgesKeep the head of thebed at the lowest levelfor the patients/clientsconditionRelieve heel pressure inbed-boundpatients/clients or withimmobilised lower limbsEmploy proper lifting& manual h<strong>and</strong>lingtechniquesMaximisepatient/clientsactivity &mobilisationconsistent withmedical condition &abilityRepositionpatient/clientsaccording to theirrisk status <strong>and</strong> asfrequently as skin’stolerance dictatesAllocate an appropriatesupport surface foridentified level of risk. Usein conjunction with anindividualised turningregimenInvolve relevant membersof the multi-disciplinaryteam• physiotherapist• occupationaltherapist• dietician• medical staff• nursing staffDocument clearly all riskassessments,interventions &outcomesRegularly assessresponses tointerventionsAvoid prolongeduninterrupted sitting in achair or wheelchair(> two hours)Avoid positioningpatients on thetrochanter
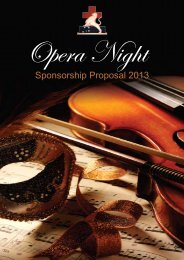
Appendix 4<strong>Pressure</strong> <strong>Ulcer</strong> GradesGrade Definition Explanatory NotesOneObservable pressure-relatedalteration(s) of intact skin mayinclude changes in one or moreof the following: skin temperature(warmth or coolness) tissueconsistency (firm or boggy feel)<strong>and</strong>/or sensation(pain/itching)The ulcer appears as a defined area of persistentredness in lightly pigmented skin, whereas in darker skintones, the ulcer may appear with persistent red, blue <strong>and</strong>purple hues.TwoThreePartial thickness skin lossinvolving epidermis <strong>and</strong>/or dermisFull thickness skin loss involvingdamage or necrosis tosubcutaneous tissue <strong>and</strong>extending down to, but notthrough, the underlying fasciaThe pressure ulcer is superficial <strong>and</strong> presents clinically asan abrasion, blister or shallow crater.Can present as necrotic tissue or eschar.The ulcer presents clinically as a deep crater with orwithout undermining of the adjacent tissue.FourFull thickness skin loss withextensive destruction, tissuenecrosis or damage to muscle,bone, or supporting structures(forexample, tendon or jointcapsule).Undermining <strong>and</strong> sinus tracts may also be associatedwith Grade 4 pressure ulcers.
Appendix 5Intervention Guidelines<strong>Pressure</strong> <strong>Ulcer</strong> Grade 1ObjectiveRelieve pressurePrevent friction <strong>and</strong> sheeringProtect skin from moistureProtect fragile skin <strong>and</strong> bony prominencesRecommendationEstablish a repositioning regime. If indicated, usepressure relieving devices according to <strong>Pressure</strong>Score Risk Assessment <strong>and</strong> the <strong>Pressure</strong> <strong>Ulcer</strong><strong>Prevention</strong> Protocol Flow Chart.Do not drag patient. Use correct manual h<strong>and</strong>lingtechnique <strong>and</strong> appropriate equipmentUse continence management systems. Use barrierskin cream to prevent skin maceration. Gently cleansite, rinse <strong>and</strong> dry well daily. Keep site clean <strong>and</strong>dry.Dermal pad, heel protector, hydrocolloid<strong>Pressure</strong> <strong>Ulcer</strong> Grade 2 (Grade 1 plus the following)ObjectiveRecommendationPromote new tissue formationAttend dressing using appropriate materials Changedressing when strike through occurs or PRN.Change dressing daily if wound infected.Remove/control exudate<strong>Pressure</strong> <strong>Ulcer</strong> Grade 3 (Grade 2 plus the following)ObjectiveRecommendationPromote new tissue formationAttend dressing using appropriate materialsChange dressing when strike through occurs orPRN.Change dressing daily if wound infected.Remove/control exudate<strong>Pressure</strong> <strong>Ulcer</strong> Grade 4 (Grade 3 plus the following)ObjectiveRecommendationTreat infection <strong>and</strong> control any odourIn addition to surgical debridement systemicantibiotic cover is recommendedDebride necrotic areaSurgical debridement is required for all necroticwounds or as per Facility / Community HealthCentre Policy. The size of the wound willdetermine if debridement is attended in OT or inthe clinical area.
Appendix 6DevicesEquipment does not replace nursing care, but is an adjunct to pressure relief such as repositioning.Good pressure area prevention practices MUST continue whilst patient is sitting out of bed, with theassistance of static or alternating cushions.TYPE OF DEVICE DESCRIPTION EXAMPLE WATERLOWSCORESTATIC PRESSURERELIEVING/REDUCING DEVICE• Support Surfaces can containfoam, gel, air or water.• Reduce pressure byincreasing the supportingsurface area (by) conformingto the body.• Decrease friction <strong>and</strong>shearing.• Also includes seating devices.St<strong>and</strong>ard Hospital Mattress<strong>Pressure</strong> relieving mattress• Contoured foam• Different density foamMattress Overlay(Placed on top of hosp mattress)• Foam Fibre Filled• Air filled10 + Medium RiskDYNAMICPRESSURERELIEVING/REDUCING DEVICE• Non-powered overlay supportsurface• Dynamic air filled chambersthat allow air exchangebetween compartments whencompressedMattress Overlay• Air-filled chambers 15+ High RiskALTERNATINGPRESSURERELIEVING/REDUCING SYSTEM• Consists of rows of cells thatdeflate <strong>and</strong> inflate alternately.• Transfer pressure loading fromone body part to another.• Come as mattress overlay ormattress replacement• Also includes seating devices1. Mattress Overlay(Placed on top of hosp mattress)• 2 Cell Cycle15 + High Risk2. Mattress Replacement• 2 Cell Cycle20 + Very HighRiskExisting <strong>Pressure</strong><strong>Ulcer</strong>sSPECIALTY BEDSLow Air Loss: <strong>Pressure</strong> reduction forvery high Risk patients. Ideal forpatients who are unable to toleratemoving surface. For example: PlasticSurgeryMattress Replacement• Overall low air loss cells Burns Unit <strong>and</strong>Critical CareNote: The above is not an exhaustive list of products available. Manufacturer’s instructions need to befollowed.(a) N.B. Devices not recommended for the prevention of pressure ulcers:• Doughnut cushion- not recommended as it reduces tissue oxygenation <strong>and</strong> the centre of the ringcan create tissue congestion <strong>and</strong> pressures in the areas surrounding the donut.• Massage - Not necessary <strong>and</strong> no evidence that prevention of pressure ulcers occurs.• Sheep skin - Can relieve friction but does not relieve pressure.• Cream – No evidence to support it relieves pressure or friction.• Water filled gloves / casks – Not recommended
Appendix 7Classification of DevicesConstant low pressure devicesConstant low pressure devices’ characteristics/features include:• may be foam, gel pads, air overlays <strong>and</strong> mattresses (static air or low air loss devices)• constant low pressure applied to the skin can still cause tissue ischaemia <strong>and</strong> necrosishence the device must be complimented with a turning regime relating to thepatient/clients risk status eliminating pressure at frequent intervals to allow blood tocirculate to ischaemic tissues• tight/knotted wrinkle free bed linen produces a ‘hammocking’ effect, undermining thepressure reducing qualities of the support systemGel filled padsFoam devicesStatic/Dynamic air devicesLow air loss devices• used on operating theatre <strong>and</strong> x-ray tables• may be used to protect the sacral area of ‘low risk’patient/clients in wheel chairs• durable, heavy to h<strong>and</strong>le <strong>and</strong> lack air flow• need to observe <strong>and</strong> correct gel migration within thepad with position changes• available in a variety of sizes, density <strong>and</strong> thicknessfor use as mattress replacements or overlays on beds<strong>and</strong> trolleys, or as chair cushions• life expectancy of products is generally one to twoyears for an overlay <strong>and</strong> five years for a mattress• foam device covers should be a two-way stretch,waterproof <strong>and</strong> vapour permeable• are non-mechanical, non-powered support surfacesthat remain motionless, except in response to patientmovement eg. RoHo• they may have interconnected chambers that allow airexchange between compartments when compressed• devices should be regularly checked <strong>and</strong> adjusted tothe patients body weight to avoid over <strong>and</strong> underinflation that may increase the interface pressure• available as an overlay, a replacement mattress or aspecialty bed• provide a continuous flow of air from the entiresurface of the mattress, using a micro-porous material• powerful motor provides the air necessary to maintainair cell inflation, despite constant air loss• pressure within the air cells is maintained at thelowest possible level for adequate patient support <strong>and</strong>body alignment
Appendix 7Alternating pressure devicesAlternating pressure devices’ characteristics/features include:• dynamic <strong>and</strong> active pressure relief systems that require an electric power source• supplied as pressure cushions, overlays, single or multilayered mattress replacements• some devices automatically adjust to patient weight <strong>and</strong> position changeAlternating pressure devices• generate alternating high <strong>and</strong> low pressures betweenan individual’s body <strong>and</strong> the support surface• cyclically inflate <strong>and</strong> deflate groups of air filled cellsgenerally placed transversely across the mattresssurface• support the body via inflated cells, while deflated cellsreduce contact pressure; this allows oxygenation <strong>and</strong>nutrition to the tissues• significantly lower tissue interface pressure whencompared with a basic hospital mattress• require checking of mattress for puncture, tubingkinking <strong>and</strong> noise factor• the pressure relieving qualities of the device arereduced by plastic sheets, incontinence sheets <strong>and</strong>sheepskins between the patient <strong>and</strong> the surface• devices must have CPR <strong>and</strong> transport facility