Mutation screening for JAK2V617F: When to order the test and how ...
Mutation screening for JAK2V617F: When to order the test and how ...
Mutation screening for JAK2V617F: When to order the test and how ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Leukemia Research 30 (2006) 739–744Brief communication<strong>Mutation</strong> <strong>screening</strong> <strong>for</strong> JAK2 V617F : <strong>When</strong> <strong>to</strong> <strong>order</strong> <strong>the</strong> <strong>test</strong><strong>and</strong> <strong>how</strong> <strong>to</strong> interpret <strong>the</strong> resultsAyalew Tefferi ∗ , Animesh PardananiDivision of Hema<strong>to</strong>logy, Mayo Clinic, Rochester, 200 First Street SW, Rochester, MN 55905, USAReceived 31 December 2005; received in revised <strong>for</strong>m 5 January 2006; accepted 6 January 2006Available online 7 February 2006AbstractWith <strong>the</strong> application of adequately sensitive <strong>test</strong>s, it is now becoming evident that more than 90% of patients with conventionally-definedpolycy<strong>the</strong>mia vera (PV) carry <strong>the</strong> somatic JAK2 V617F mutation in <strong>the</strong>ir granulocytes. However, <strong>the</strong> specific mutation is also found in o<strong>the</strong>r classic<strong>and</strong> atypical myeloproliferative dis<strong>order</strong>s (MPD), albeit at a lesser frequency. In contrast, JAK2 V617F has not been reported in patients wi<strong>the</strong>i<strong>the</strong>r reactive myeloproliferation or lymphoid dis<strong>order</strong>s. There<strong>for</strong>e, mutation <strong>screening</strong> <strong>for</strong> JAK2 V617F can be considered as a myeloid-specificclonality assay <strong>and</strong> it is diagnostically most useful in <strong>the</strong> evaluation of “polycy<strong>the</strong>mia”.© 2006 Elsevier Ltd. All rights reserved.Keywords: JAK2 mutation; Polycy<strong>the</strong>mia; Thrombocy<strong>to</strong>sis; DiagnosisBetween March <strong>and</strong> June 2005, five studies describeda novel JAK2 somatic point mutation (a G-C <strong>to</strong> T-Atransversion, at nucleotide 1849 of exon 14, resulting in<strong>the</strong> substitution of valine <strong>to</strong> phenylalanine at codon 617;JAK2 V617F ) in classic, BCR/ABL-negative myeloproliferativedis<strong>order</strong>s (MPD) [1–5]. Subsequently, <strong>the</strong> same mutationwas demonstrated in o<strong>the</strong>r myeloid dis<strong>order</strong>s includingacute myeloid leukemia, <strong>the</strong> myelodysplastic syndrome,chronic myelomonocytic leukemia, juvenile myelomonocyticleukemia, chronic neutrophilic leukemia, hypereosinophilicsyndrome, systemic mas<strong>to</strong>cy<strong>to</strong>sis (SM), <strong>and</strong> o<strong>the</strong>ratypical MPD (Table 1). In contrast, JAK2 V617F has notyet been reported in patients with secondary polycy<strong>the</strong>mia,[1,6,7] acute [8–11] or chronic lymphoid dis<strong>order</strong>s, [11–14]non-hema<strong>to</strong>logic cancer, [10], or molecularly-defined MPD(e.g. chronic myeloid leukemia, [9] PDGFR-rearrangedeosinophilic dis<strong>order</strong>s, [6] KIT D816V -positive SM) [6]. Fur<strong>the</strong>rmore,among several hema<strong>to</strong>logic <strong>and</strong> solid tumorcell lines, JAK2 V617F was detected in only human erythroleukemia(HEL) cells [13,14].∗ Corresponding author: Tel.: +1 507 284 3159; fax: +1 507 266 4972.E-mail address: tefferi.ayalew@mayo.edu (A. Tefferi).The pathogenetic relevance of JAK2 V617F is currentlyunder intense investigation [15]. The specific mutation occurswithin <strong>the</strong> enzymatically inactive JH2 pseudo-kinase domainthat regulates <strong>the</strong> active JH1 kinase domain [16]. Such indirectJAK2 activation leads <strong>to</strong> constitutive JAK-STAT hyperactivationwith resultant induction of erythropoietin hypersensitivity<strong>and</strong> cell trans<strong>for</strong>mation in murine cell lines <strong>and</strong>in vivo erythrocy<strong>to</strong>sis in mice [1]. These labora<strong>to</strong>ry observationsare consistent with <strong>the</strong> clinical demonstration of significantlyhigher hemoglobin levels in JAK2 V617F -positiveversus JAK2 V617F -negative ET [17–19] <strong>and</strong> in polycy<strong>the</strong>miavera (PV) patients with homozygous versus heterozygousmutant allele [20]. Similarly, mutation burden has beens<strong>how</strong>n <strong>to</strong> be significantly higher in PV compared <strong>to</strong> o<strong>the</strong>rMPD [21]. Most recently, activation of <strong>the</strong> enzyme as wellas downstream signaling involving JAK2 V617F was s<strong>how</strong>n <strong>to</strong>require <strong>the</strong> presence of an associated Type 1 cy<strong>to</strong>kine recep<strong>to</strong>r,which might explain <strong>the</strong> myeloid dis<strong>order</strong>-specificity aswell as phenotypic diversity that is associated with <strong>the</strong> specificmutation [22].A quick glance at Table 1 discloses a marked variationin mutational frequency, among different studies, in <strong>the</strong> contex<strong>to</strong>f similarly defined clinicopathologic entities. Based on0145-2126/$ – see front matter © 2006 Elsevier Ltd. All rights reserved.doi:10.1016/j.leukres.2006.01.004
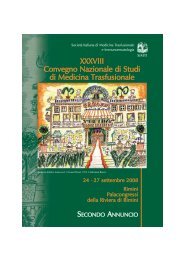
740 A. Tefferi, A. Pardanani / Leukemia Research 30 (2006) 739–744Table 1Summary of published literature on JAK2 V617F mutational frequencies in myeloproliferative dis<strong>order</strong>s. Homozygous mutational frequencies are indicated inparen<strong>the</strong>sisReference Polycy<strong>the</strong>mia vera Essential thrombocy<strong>the</strong>mia MMM O<strong>the</strong>r myeloid dis<strong>order</strong>sAssay type usedCell type usedLevine et al. [3]PCR sequencing 74% (25%) 32% (3%) 35% (9%) –Neutrophils n = 164 n = 115 n =46Kralovics et al. [4]PCR sequencing 65% (27%) 23% (3%) 57% (22%) CML 0%Neutrophils n = 128 n =93 n =23 (n =9)Baxter et al. [2]AS-PCR 97% (26%) 57% (0%) 50% (19%) –Neutrophils n =73 n =51 n =16All were AMMJones et al. [6]AS-PCR 81% (33%) 41% (7%) 43% (29%) CML 0%PB cells n =72 n =59 n =35 (n = 18)CMML/UMPD 20% (n = 152)HES/CEL 2% (n = 134)SM 0% (n = 28)CNL 33% (n =6)AML 0% (n = 17)James et al. [1]PCR sequencing 89% (30%) 43% 43% –Neutrophils n =45 n =21 n =7Tefferi et al. [7]PCR sequencing 95% (26%) 55% (0%) 30% (0%) –Neutrophils n =38 n =22 n =10All were AMMJelinek et al. [9]Pyrosequencing 86% 30% 95% CML 0%PB cells n =29 n =10 n =19 (n = 99)Post-MPD AML 55% (n = 22)AML M0-M5 0% (n = 20)AMLM60%(n =8)AML M7 18% (n = 11)MDS 1% (n = 68)CMML 13% (n = 52)Atypical MPD 19% (n = 16)Goerttler et al. [30]cDNA PCR sequencing 100% (27%) 33% (5%) 57% (21%) –Neutrophils n =22 n =42 n =14Passamonti et al. [21]Real-time AS-PCR 92% 53% 72% –Neutrophils n =25 n =19 n =46AMM 57%PPMM 100%James et al. [24]Real-time PCR 95% – – –Neutrophils n =80Campbell et al. [18]AS-PCR – 53% – –PB cells n = 776Wolanskyj et al. [17]PCR sequencing – 49% (0%) – –PB-MNC or BM cells n = 150An<strong>to</strong>nioli et al. [19]AS-PCR – 57% (6%) – –Neutrophils n = 130
A. Tefferi, A. Pardanani / Leukemia Research 30 (2006) 739–744 741Table 1 (Continued )Reference Polycy<strong>the</strong>mia vera Essential thrombocy<strong>the</strong>mia MMM O<strong>the</strong>r myeloid dis<strong>order</strong>sAssay type usedCell type usedZhao et al. [5]PCR sequencing 83% (NA) – – –PB-MNC n =24Tefferi et al. [31]PCR sequencing – – 51% (6%) –PB-MNC n = 157AMM-45% (3%)PTMM-40% (11%)PPMM-91% (18%)Campbell et al. [32]AS-PCR or sequencing – – 55% –PB or BM cells n = 152All were AMMTefferi et al. [20]PCR sequencing 92% (21%) – – –Neutrophils n =63Steensma et al. [28] – – – MDS 5% (n = 101)PCR sequencing CMML 3% (n = 119)PB <strong>and</strong> BM cells HES 0% (n = 11)SM 25% (n =8)CNL 17% (n =6)Levine et al. [11]PCR sequencing – – – De novo AML 0.5% (n = 219)PB <strong>and</strong> BM cells Post-MPD AML 100% (n =3)MDS4%(n = 48)CMML/atypical MPD 8% (n = 116)Johan et al. [33]AS-PCR – – 38% CMML 2%PB cells n =21 (n = 47)All were AMMOhyashiki et al. [27]PCR sequencing – – – MDS-MF 33% (n =6)BM or PB cellsLee et al. [10]PCR-based SSCP 65% (35%) – – AML 2% (n = 113)BM cells n =17Scott et al. [14] AML6%(n = 90)AS-PCR MDS 0.5% (n = 20)BM cells CMML 0% (n =5)CML 1%* (n = 91)Tono et al. [34]PCR sequencing – – – JMML 20% (n =5)BM cells* The single CML patient had actually BCR/ABL-negative ET prior <strong>to</strong> <strong>the</strong> development of CML. The mutational frequencies in different studies are notcomparable because of <strong>the</strong> use of assays with variable sensitivity. AS-PCR, allele-specific PCR; CMML, chronic myelomonocytic leukemia; JMML, juvenilemyelomonocytic leukemia; CML, chronic myeloid leukemia; MDS, myelodysplastic syndrome; HES, hypereosinophilic syndrome; CEL, chronic eosinophilicleukemia; SM, systemic mas<strong>to</strong>cy<strong>to</strong>sis; CNL, chronic neutrophilic leukemia; UMPD, unclassified myeloproliferative dis<strong>order</strong>; AML, acute myeloid leukemia;BM, bone marrow; PB, peripheral blood; MNC, mononuclear cells; MMM, myelofibrosis with myeloid metaplasia; AMM, agnogenic myeloid metaplasia;PTMM, post thrombocy<strong>the</strong>mic myeloid metaplasia; PPMM, post polycy<strong>the</strong>mic myeloid metaplasia; PCR, polymerase chain reaction.our own experience that revealed, on careful re-review, anincorrect diagnosis <strong>for</strong> four reportedly JAK2 V617F -negativePV cases, [23] we trust that diagnostic imprecision is inpart <strong>to</strong> blame <strong>for</strong> <strong>the</strong> observed inconsistency in diseasespecificincidence figures reported in <strong>the</strong> literature. Such acontention is supported by a recent study that demonstrateddiscordant JAK2 V617F prevalence figures in WHO- versusPVSG-defined PV within <strong>the</strong> same study population [24].Differences in methodological assay sensitivity constituteano<strong>the</strong>r potential cause of discrepancy in reported mutational
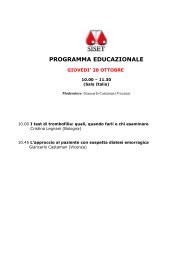
742 A. Tefferi, A. Pardanani / Leukemia Research 30 (2006) 739–744Table 2Test indications <strong>and</strong> result interpretation of mutation <strong>screening</strong> <strong>for</strong> JAK2 V617FJAK2 V617F <strong>test</strong> indications Positive result Negative result“Increased” hemoglobin/hema<strong>to</strong>crit Consistent with PV PV diagnosis unlikely but not impossibleSplanchnic or cerebral vein thrombosis Consistent with PV/MPD PV diagnosis unlikelyThrombocy<strong>to</strong>sis Consistent with MPD Diagnostically unhelpfulUnexplained cy<strong>to</strong>penia or cy<strong>to</strong>sis Consistent with MPD Diagnostically unhelpfulfrequencies. For example, use of a more sensitive assay in onestudy led <strong>to</strong> an increase in mutational frequency <strong>for</strong> PV from73% <strong>to</strong> 97% [2]. Assay sensitivity might also be affected byboth tissue type (neutrophils versus o<strong>the</strong>r cells) <strong>and</strong> nucleicacid source (genomic DNA versus RNA) of <strong>the</strong> <strong>test</strong> sample.Never<strong>the</strong>less, <strong>the</strong> practical impact of such fac<strong>to</strong>rs is currentlyuncertain <strong>and</strong> systematic studies are needed <strong>for</strong> fur<strong>the</strong>rclarification [24]. In <strong>the</strong> meantime, we strongly recommendavoidance of undue reliance on a single <strong>test</strong> report <strong>and</strong> encouragerepeat <strong>test</strong>ing in <strong>the</strong> presence of ei<strong>the</strong>r marginally positiveor clinically incompatible <strong>test</strong> results.Some generalizations <strong>and</strong> practical recommendations canbe made based on in<strong>for</strong>mation from Table 1 <strong>and</strong> <strong>the</strong> abovediscussion (Table 2). First, ei<strong>the</strong>r peripheral blood or bonemarrow mutation <strong>screening</strong> <strong>for</strong> JAK2 V617F appears <strong>to</strong> becurrently most useful <strong>for</strong> <strong>the</strong> evaluation of “polycy<strong>the</strong>mia”.However, <strong>the</strong> particular <strong>test</strong> is intended <strong>to</strong> complement ra<strong>the</strong>rthan substitute <strong>for</strong> clinical diagnosis that is based on his<strong>to</strong>ry,physical examination, <strong>and</strong> pertinent labora<strong>to</strong>ry <strong>test</strong>s includingserum erythropoietin level <strong>and</strong> bone marrow examination[25]. Accordingly, if clinical suspicion <strong>for</strong> PV is low, a negativeperipheral blood <strong>test</strong> result argues against <strong>the</strong> specificdiagnosis <strong>and</strong> should allow deferral of fur<strong>the</strong>r investigationwith ei<strong>the</strong>r bone marrow biopsy or red cell mass measurement.A bone marrow biopsy is, <strong>how</strong>ever, indicated in <strong>the</strong>presence of a high clinical suspicion <strong>for</strong> PV, regardless ofmutational status [20,21,24]. Fur<strong>the</strong>rmore, in <strong>the</strong> context ofsuspected PV, in<strong>for</strong>mation regarding JAK2 V617F mutationalstatus should help clarify <strong>the</strong> situation with ei<strong>the</strong>r “equivocal”or “inconsistent” bone marrow his<strong>to</strong>logy.Peripheral blood mutation <strong>screening</strong> <strong>for</strong> JAK2 V617F is alsohelpful during <strong>the</strong> evaluation of an increased platelet countthat is clinically not consistent with reactive thrombocy<strong>to</strong>sis.However, unlike <strong>the</strong> a<strong>for</strong>ementioned situation with <strong>the</strong> workup of polycy<strong>the</strong>mia, <strong>the</strong> negative predictive value of <strong>the</strong> <strong>test</strong>is <strong>to</strong>o low <strong>to</strong> warrant deferral of bone marrow examination in<strong>the</strong> absence of JAK2 V617F [17,18]. Similarly, although a positive<strong>test</strong> result confirms clonality <strong>and</strong> makes <strong>the</strong> possibility ofFig. 1. A modern diagnostic algorithm <strong>for</strong> suspected polycy<strong>the</strong>mia vera (PV) that incorporates mutation <strong>screening</strong> <strong>for</strong> JAK2 V617F . * PV-characteristic featuresinclude splenomegaly, leukocy<strong>to</strong>sis, thrombocy<strong>to</strong>sis, aquagenic pruritus, splanchnic or cerebral vein thrombosis, erythromelalgia, <strong>and</strong> microcy<strong>to</strong>sis related <strong>to</strong>iron deficiency.
A. Tefferi, A. Pardanani / Leukemia Research 30 (2006) 739–744 743chronic myeloid leukemia unlikely, it cannot fur<strong>the</strong>r specify<strong>the</strong> underlying MPD [18]. There<strong>for</strong>e, a bone marrow examinationshould not be skipped over during <strong>the</strong> work up ofapparently clonal thrombocy<strong>to</strong>sis, regardless of JAK2 V617Fmutational status. Approximately 50% of patients with ETare expected <strong>to</strong> carry <strong>the</strong> JAK2 V617F mutation [17,18] <strong>and</strong>a positive mutation <strong>screening</strong> <strong>test</strong> confirms <strong>and</strong>/or clarifies<strong>the</strong> o<strong>the</strong>rwise largely subjective his<strong>to</strong>logical diagnosis of ET.Fur<strong>the</strong>rmore, although heterozygous JAK2 V617F is seen inboth ET <strong>and</strong> PV, homozygosity <strong>for</strong> <strong>the</strong> mutant allele favors<strong>the</strong> latter diagnosis [18].In general, our enthusiasm is lukewarm regarding <strong>the</strong> utilityof mutation <strong>screening</strong> <strong>for</strong> JAK2 V617F in MPD o<strong>the</strong>r thanPV or ET [6,26,27]. In this regard, it is apparent from <strong>the</strong>in<strong>for</strong>mation from Table 1 that <strong>the</strong> particular <strong>test</strong> cannot reliablydistinguish classic MPD from atypical MPD. However,mutational frequency in both MDS <strong>and</strong> de novo AML islow enough <strong>to</strong> consider limited utility in differentiating <strong>the</strong>sedis<strong>order</strong>s from MPD as a whole [9,11,28]. Also, in routineclinical practice, it is not infrequent <strong>to</strong> encounter casesof unexplained cy<strong>to</strong>penia, cy<strong>to</strong>sis, or deep vein thrombosisinvolving splanchnic or cerebral vessels. In such instances,mutation <strong>screening</strong> <strong>for</strong> JAK2 V617F is indicated <strong>and</strong> a positive<strong>test</strong> is consistent with <strong>the</strong> presence of occult MPD includinginapparent PV whereas a negative <strong>test</strong> result does not ruleout <strong>the</strong> possibility. Finally, our overall discussion assumes<strong>the</strong> utilization of adequately sensitive (i.e. sensitivity of 5%or less) mutation <strong>screening</strong> assays as well as a Bayesianapproach <strong>to</strong> result interpretation. The latter becomes especiallyimportant when using super-sensitive assays that mightdetect small copies of JAK2 V617F in healthy individuals, a situationthat is analogous <strong>to</strong> BCR/ABL [29]. Finally, <strong>the</strong> overallobjectivity <strong>and</strong> accessibility of both JAK2 mutation <strong>screening</strong><strong>and</strong> erythropoietin determination from <strong>the</strong> peripheralblood allows <strong>for</strong> a practical modern approach in evaluatingpolycy<strong>the</strong>mia that does not require red cell mass measurement<strong>and</strong> limits <strong>the</strong> number of bone marrow examinations(Fig. 1).AcknowledgementsWe acknowledge Dr. Rebecca F. McClure’s help indata sharing <strong>and</strong> scientific discussion. There are no potentialauthor conflicts of interest that relate <strong>to</strong> <strong>the</strong> currentmanuscript.Contributions. Ayalew Tefferi came up with <strong>the</strong> concept,designed <strong>the</strong> study, <strong>and</strong> wrote <strong>the</strong> paper. Dr. Animesh Pardananihelped with <strong>the</strong> design of <strong>the</strong> study <strong>and</strong> approved <strong>the</strong>final draft of <strong>the</strong> paper.References[1] James C, Ugo V, Le Couedic JP, Staerk J, Delhommeau F, LacoutC, et al. A unique clonal JAK2 mutation leading <strong>to</strong> constitutivesignalling causes polycythaemia vera. Nature 2005;434:1144–8.[2] Baxter EJ, Scott LM, Campbell PJ, East C, Fourouclas N, Swan<strong>to</strong>nS, et al. Acquired mutation of <strong>the</strong> tyrosine kinase JAK2 in humanmyeloproliferative dis<strong>order</strong>s. Lancet 2005;365:1054–61.[3] Levine RL, Wadleigh M, Cools J, Ebert BL, Wernig G, HuntlyBJ, et al. Activating mutation in <strong>the</strong> tyrosine kinase JAK2 in polycy<strong>the</strong>miavera, essential thrombocy<strong>the</strong>mia, <strong>and</strong> myeloid metaplasiawith myelofibrosis. Cancer Cell 2005;7:387–97.[4] Kralovics R, Passamonti F, Buser AS, Teo SS, Tiedt R, PasswegJR, et al. A gain-of-function mutation of JAK2 in myeloproliferativedis<strong>order</strong>s. N Engl J Med 2005;352:1779–90.[5] Zhao R, Xing S, Li Z, Fu X, Li Q, Krantz SB, et al. Identificationof an acquired JAK2 mutation in polycy<strong>the</strong>mia vera. J Biol Chem2005;280:22788–92.[6] Jones AV, Kreil S, Zoi K, Waghorn K, Curtis C, Zhang L, et al.Widespread occurrence of <strong>the</strong> JAK2 V617F mutation in chronicmyeloproliferative dis<strong>order</strong>s. Blood 2005;106:2162–8.[7] Tefferi A, Sirhan S, Lasho TL, Schwager SM, Li CY, Dingli D,et al. Concomitant neutrophil JAK2 mutation <strong>screening</strong> <strong>and</strong> PRV-1 expression analysis in myeloproliferative dis<strong>order</strong>s <strong>and</strong> secondarypolycythaemia. Br J Haema<strong>to</strong>l 2005;131:166–71.[8] Sulong S, Case M, Min<strong>to</strong> L, Wilkins B, Hall A, Irving J. The V617Fmutation in Jak2 is not found in childhood acute lymphoblasticleukaemia. Br J Haema<strong>to</strong>l 2005;130:964–5.[9] Jelinek J, Oki Y, Gharibyan V, Bueso-Ramos C, Prchal JT, Vers<strong>to</strong>vsekS, et al. JAK2 mutation 1849G > T is rare in acute leukemiasbut can be found in CMML, Philadelphia chromosome-negativeCML, <strong>and</strong> megakaryocytic leukemia. Blood 2005;106:3370–3.[10] Lee JW, Kim YG, Soung YH, Han KJ, Kim SY, Rhim HS, et al.The JAK2 V617F mutation in de novo acute myelogenous leukemias.Oncogene 2005.[11] Levine RL, Loriaux M, Huntly BJ, Loh ML, Beran M, S<strong>to</strong>ffregenE, et al. The <strong>JAK2V617F</strong> activating mutation occurs in chronicmyelomonocytic leukemia <strong>and</strong> acute myeloid leukemia, but notin acute lymphoblastic leukemia or chronic lymphocytic leukemia.Blood 2005;106:3377–9.[12] Lee JW, Soung YH, Kim SY, Nam SW, Park WS, Lee JY, et al.JAK2 V617F mutation is uncommon in non-Hodgkin lymphomas.Leuk Lymphoma 2006;47:313–4.[13] Melzner I, Weniger MA, Menz CK, Moller P. Absence of <strong>the</strong> <strong>JAK2V617F</strong> activating mutation in classical Hodgkin lymphoma <strong>and</strong> primarymediastinal B-cell lymphoma. Leukemia 2005.[14] Scott LM, Campbell PJ, Baxter EJ, Todd T, Stephens P, EdkinsS, et al. The V617F JAK2 mutation is uncommon in cancers <strong>and</strong>in myeloid malignancies o<strong>the</strong>r than <strong>the</strong> classic myeloproliferativedis<strong>order</strong>s. Blood 2005;106:2920–1.[15] Tefferi A, Gillil<strong>and</strong> DG. JAK2 in myeloproliferative dis<strong>order</strong>s is notjust ano<strong>the</strong>r kinase. Cell Cycle 2005;4:1053–6.[16] Saharinen P, Vihinen M, Silvennoinen O. Au<strong>to</strong>inhibition of Jak2tyrosine kinase is dependent on specific regions in its pseudokinasedomain. Mol Biol Cell 2003;14:1448–59.[17] Wolanskyj AP, Lasho TL, Schwager SM, McClure RF, Wadleigh M,Lee SJ, et al. JAK2 mutation in essential thrombocythaemia: clinicalassociations <strong>and</strong> long-term prognostic relevance. Br J Haema<strong>to</strong>l2005;131:208–13.[18] Campbell PJ, Scott LM, Buck G, Wheatley K, East CL, Marsden JT,et al. Definition of subtypes of essential thrombocythaemia <strong>and</strong> relation<strong>to</strong> polycythaemia vera based on JAK2 V617F mutation status:a prospective study. Lancet 2005;366:1945–53.[19] An<strong>to</strong>nioli E, Guglielmelli P, Pancrazzi A, Bogani C, Verrucci M,Ponziani V, et al. Clinical implications of <strong>the</strong> JAK2 V617F mutationin essential thrombocy<strong>the</strong>mia. Leukemia 2005;19:1847–9.[20] Tefferi A, Lasho TL, Schwager SM, Str<strong>and</strong> JS, Elliott M,Mesa R, et al. The clinical phenotype of wild-type, heterozygous,<strong>and</strong> homozygous JAK2(V617F) in polycy<strong>the</strong>mia vera. Cancer2005.[21] Passamonti F, Rumi E, Pietra D, Della Porta MG, Boveri E, Pascut<strong>to</strong>C, et al. Relation between JAK2 (V617F) mutation status,
744 A. Tefferi, A. Pardanani / Leukemia Research 30 (2006) 739–744granulocyte activation <strong>and</strong> constitutive mobilization of CD34-positivecells in<strong>to</strong> peripheral blood in myeloproliferative dis<strong>order</strong>s. Blood2005.[22] Lu X, Levine R, Tong W, Wernig G, Pikman Y, Zarnegar S, et al.Expression of a homodimeric type I cy<strong>to</strong>kine recep<strong>to</strong>r is required<strong>for</strong> <strong>JAK2V617F</strong>-mediated trans<strong>for</strong>mation. Proc Natl Acad Sci USA2005;102:18962–7.[23] McClure R, Mai M, Lasho T. Validation of two clinically usefulassays <strong>for</strong> evaluation of JAK2 V617F mutation in chronic myeloproliferativedis<strong>order</strong>s. Leukemia 2005.[24] James C, Delhommeau F, Marzac C, Teyss<strong>and</strong>ier I, Couedic JP,Giraudier S, et al. Detection of JAK2 V617F as a first intentiondiagnostic <strong>test</strong> <strong>for</strong> erythrocy<strong>to</strong>sis. Leukemia 2005.[25] Tefferi A, Spivak JL. Polycy<strong>the</strong>mia vera: scientific advances <strong>and</strong>current practice. Semin Hema<strong>to</strong>l 2005;42:206–20.[26] Vardiman JW, Brunning RD, Harris NL. WHO his<strong>to</strong>logical classificationof chronic myeloproliferative diseases. In: Jaffe ES, HarrisNL, Stein H, Vardiman JW, edi<strong>to</strong>rs. World Health Organization classificationof tumors: tumours of <strong>the</strong> haema<strong>to</strong>poietic <strong>and</strong> lymphoidtissues. Lyon, France: International Agency <strong>for</strong> Research on Cancer(IARC) Press; 2001. p. 17–44.[27] Ohyashiki K, Aota Y, Akahane D, Go<strong>to</strong>h A, Miyazawa K, KimuraY, et al. The JAK2 V617F tyrosine kinase mutation in myelodysplasticsyndromes (MDS) developing myelofibrosis indicates <strong>the</strong>myeloproliferative nature in a subset of MDS patients. Leukemia2005;19:2359–60.[28] Steensma DP, Dewald GW, Lasho TL, Powell HL, McClure RF,Levine RL, et al. The JAK2 V617F activating tyrosine kinase mutationis an infrequent event in both “atypical” myeloproliferativedis<strong>order</strong>s <strong>and</strong> myelodysplastic syndromes. Blood 2005;106:1207–9.[29] Bose S, Deininger M, Gora-Tybor J, Goldman JM, Melo JV.The presence of typical <strong>and</strong> atypical BCR-ABL fusion genes inleukocytes of normal individuals: biologic significance <strong>and</strong> implications<strong>for</strong> <strong>the</strong> assessment of minimal residual disease. Blood1998;92:3362–7.[30] Goerttler PS, Steimle C, Marz E, Johansson PL, Andreasson B,Griesshammer M, et al. The Jak2V617F mutation, PRV-1 overexpression,<strong>and</strong> EEC <strong>for</strong>mation define a similar cohort of MPD patients.Blood 2005;106:2862–4.[31] Tefferi A, Lasho TL, Schwager SM, Steensma DP, Mesa RA, Li CY,et al. The JAK2(V617F) tyrosine kinase mutation in myelofibrosiswith myeloid metaplasia: lineage specificity <strong>and</strong> clinical correlates.Br J Haema<strong>to</strong>l 2005;131:320–8.[32] Campbell PJ, Griesshammer M, Dohner K, Dohner H, Kusec R,Hasselbalch HC, et al. The V617F mutation in JAK2 is associatedwith poorer survival in idiopathic myelofibrosis. Blood 2005.[33] Johan MF, Goodeve AC, Bowen DT, Frew ME, Reilly JT.JAK2 V617F <strong>Mutation</strong> is uncommon in chronic myelomonocyticleukaemia. Br J Haema<strong>to</strong>l 2005;130:968.[34] Tono C, Xu G, Toki T, Takahashi Y, Sasaki S, Terui K, et al.JAK2 Val617Phe activating tyrosine kinase mutation in juvenilemyelomonocytic leukemia. Leukemia 2005;19:1843–4.