Central nervous system vasculitis
Central nervous system vasculitis
Central nervous system vasculitis

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
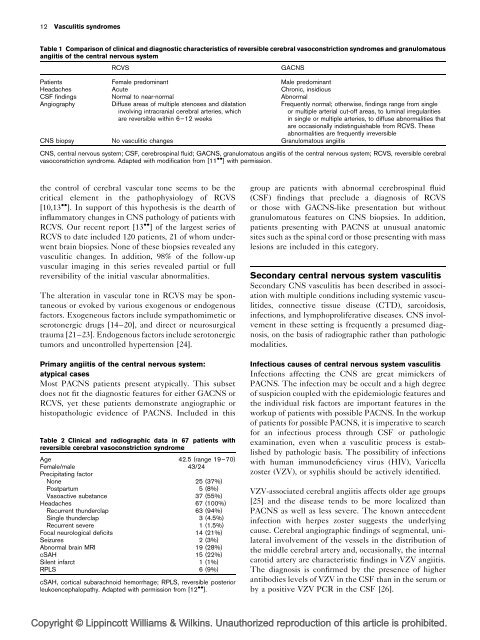
12 Vasculitis syndromesTable 1 Comparison of clinical and diagnostic characteristics of reversible cerebral vasoconstriction syndromes and granulomatousangiitis of the central <strong>nervous</strong> <strong>system</strong>RCVSGACNSPatients Female predominant Male predominantHeadaches Acute Chronic, insidiousCSF findings Normal to near-normal AbnormalAngiographyDiffuse areas of multiple stenoses and dilatationinvolving intracranial cerebral arteries, whichare reversible within 6–12 weeksCNS biopsy No vasculitic changes Granulomatous angiitisFrequently normal; otherwise, findings range from singleor multiple arterial cut-off areas, to luminal irregularitiesin single or multiple arteries, to diffuse abnormalities thatare occasionally indistinguishable from RCVS. Theseabnormalities are frequently irreversibleCNS, central <strong>nervous</strong> <strong>system</strong>; CSF, cerebrospinal fluid; GACNS, granulomatous angiitis of the central <strong>nervous</strong> <strong>system</strong>; RCVS, reversible cerebralvasoconstriction syndrome. Adapted with modification from [11 ] with permission.the control of cerebral vascular tone seems to be thecritical element in the pathophysiology of RCVS[10,13 ]. In support of this hypothesis is the dearth ofinflammatory changes in CNS pathology of patients withRCVS. Our recent report [13 ] of the largest series ofRCVS to date included 120 patients, 21 of whom underwentbrain biopsies. None of these biopsies revealed anyvasculitic changes. In addition, 98% of the follow-upvascular imaging in this series revealed partial or fullreversibility of the initial vascular abnormalities.The alteration in vascular tone in RCVS may be spontaneousor evoked by various exogenous or endogenousfactors. Exogeneous factors include sympathomimetic orserotonergic drugs [14–20], and direct or neurosurgicaltrauma [21–23]. Endogenous factors include serotonergictumors and uncontrolled hypertension [24].Primary angiitis of the central <strong>nervous</strong> <strong>system</strong>:atypical casesMost PACNS patients present atypically. This subsetdoes not fit the diagnostic features for either GACNS orRCVS, yet these patients demonstrate angiographic orhistopathologic evidence of PACNS. Included in thisTable 2 Clinical and radiographic data in 67 patients withreversible cerebral vasoconstriction syndromeAge 42.5 (range 19–70)Female/male 43/24Precipitating factorNone 25 (37%)Postpartum 5 (8%)Vasoactive substance 37 (55%)Headaches 67 (100%)Recurrent thunderclap 63 (94%)Single thunderclap 3 (4.5%)Recurrent severe 1 (1.5%)Focal neurological deficits 14 (21%)Seizures 2 (3%)Abnormal brain MRI 19 (28%)cSAH 15 (22%)Silent infarct 1 (1%)RPLS 6 (9%)cSAH, cortical subarachnoid hemorrhage; RPLS, reversible posteriorleukoencephalopathy. Adapted with permission from [12 ].group are patients with abnormal cerebrospinal fluid(CSF) findings that preclude a diagnosis of RCVSor those with GACNS-like presentation but withoutgranulomatous features on CNS biopsies. In addition,patients presenting with PACNS at unusual anatomicsites such as the spinal cord or those presenting with masslesions are included in this category.Secondary central <strong>nervous</strong> <strong>system</strong> <strong>vasculitis</strong>Secondary CNS <strong>vasculitis</strong> has been described in associationwith multiple conditions including <strong>system</strong>ic vasculitides,connective tissue disease (CTD), sarcoidosis,infections, and lymphoproliferative diseases. CNS involvementin these setting is frequently a presumed diagnosis,on the basis of radiographic rather than pathologicmodalities.Infectious causes of central <strong>nervous</strong> <strong>system</strong> <strong>vasculitis</strong>Infections affecting the CNS are great mimickers ofPACNS. The infection may be occult and a high degreeof suspicion coupled with the epidemiologic features andthe individual risk factors are important features in theworkup of patients with possible PACNS. In the workupof patients for possible PACNS, it is imperative to searchfor an infectious process through CSF or pathologicexamination, even when a vasculitic process is establishedby pathologic basis. The possibility of infectionswith human immunodeficiency virus (HIV), Varicellazoster (VZV), or syphilis should be actively identified.VZV-associated cerebral angiitis affects older age groups[25] and the disease tends to be more localized thanPACNS as well as less severe. The known antecedentinfection with herpes zoster suggests the underlyingcause. Cerebral angiographic findings of segmental, unilateralinvolvement of the vessels in the distribution ofthe middle cerebral artery and, occasionally, the internalcarotid artery are characteristic findings in VZV angiitis.The diagnosis is confirmed by the presence of higherantibodies levels of VZV in the CSF than in the serum orby a positive VZV PCR in the CSF [26].Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.