Allergic coNtAct DermAtitis of the foot - The Dermatologist
Allergic coNtAct DermAtitis of the foot - The Dermatologist
Allergic coNtAct DermAtitis of the foot - The Dermatologist
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
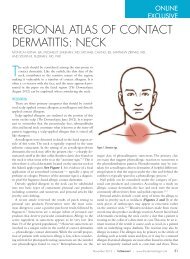
sic “shoe pattern dermatitis” on <strong>the</strong> <strong>foot</strong>is suggestive <strong>of</strong> allergic contact dermatitis(Figure 1). This pattern shows aneczematous process involving <strong>the</strong> dorsal<strong>foot</strong> and ankle with notable sparing <strong>of</strong><strong>the</strong> inter-digital spaces. <strong>The</strong>re is <strong>of</strong>tena relative symmetry, but one side maybe more heavily affected than <strong>the</strong> o<strong>the</strong>r.Spreading <strong>of</strong> <strong>the</strong> process up <strong>the</strong> anklesover time is also a clue to ACD. Thisis particularly true in <strong>the</strong> setting <strong>of</strong> achronic, stable, well-localized dermatitisthat <strong>the</strong>n shifts to become poorly localizedand spreading.Endogenous dermatitis is <strong>of</strong>ten <strong>the</strong>most difficult to separate from allergiccontact dermatitis. This category includesatopic <strong>foot</strong> dermatitis, nummular<strong>foot</strong> dermatitis, juvenile plantar dermatosisand <strong>the</strong> pompholyx-dyshidrosisspectrum. In many cases, <strong>the</strong> diagnosis<strong>of</strong> endogenous dermatitis is one <strong>of</strong> exclusion,made only after a negative patchtest has been performed to help rule outallergic contact dermatitis.Acral papulosquamous entities maybe easily diagnosed if typical stigmataare seen elsewhere on <strong>the</strong> patient. However,if involvement is limited to <strong>the</strong>feet, <strong>the</strong>re can be significant morphologicoverlap with chronic eczematousprocesses. Acral psoriasis, palmoplantarpustulosis and pityriasis rubra pilarisfall into this category. In a study in<strong>the</strong> International Journal <strong>of</strong> Dermatology,70 patients suspected <strong>of</strong> having allergiccontact dermatitis <strong>of</strong> <strong>the</strong> <strong>foot</strong> underwentpatch testing; 30 were given a finaldiagnosis <strong>of</strong> psoriasis. 20Infectious entities <strong>of</strong> <strong>the</strong> feet aretypically less likely to be misdiagnosedas contact dermatitis, with one majorexception. Dermatophyte infection caneasily be missed and should always beconsidered in <strong>the</strong> differential diagnosis<strong>of</strong> a patient with a possible contact dermatitis<strong>of</strong> <strong>the</strong> <strong>foot</strong>.Hybrid dermatitis is a clinically usefulterm that takes into account <strong>the</strong> factthat many patients have multifactorialdisease. It is <strong>of</strong>ten <strong>the</strong> case that a patientmay be atopic with a component <strong>of</strong> irritantdermatitis and superimposed allergiccontact dermatitis. Utilizing <strong>the</strong>term “hybrid dermatitis” brings int<strong>of</strong>ocus <strong>the</strong> need to address all underlyingfactors to ensure clinical success. Similarto <strong>the</strong> endogenous group, this diagnosisis typically only made after <strong>the</strong> completion<strong>of</strong> a full work-up, including comprehensivepatch testing.Practical Aspects <strong>of</strong> Patch TestingAs discussed above, <strong>the</strong> differential diagnosis<strong>of</strong> <strong>foot</strong> dermatitis can be a challenge.Patch testing is <strong>the</strong> gold standardfor making <strong>the</strong> diagnosis <strong>of</strong> allergic contactdermatitis. Most patch test expertsadvocate an approach that utilizes anexpanded series, including testing components<strong>of</strong> <strong>the</strong> patient’s own <strong>foot</strong>wearand socks. <strong>The</strong> most common allergenshave been listed in Table 1.While management <strong>of</strong> ACD <strong>of</strong> <strong>the</strong><strong>foot</strong> can be challenging, <strong>the</strong> majority<strong>of</strong> patients should be able to attainsustained improvement or resolution<strong>of</strong> <strong>the</strong>ir symptoms if proper patch testingis carried out and relevant allergensare avoided. 12 To maximize <strong>the</strong> yield <strong>of</strong>patch testing, it is important to recognizewhich patterns <strong>of</strong> <strong>foot</strong> dermatitisare most likely to show relevant positivereactions. For example, <strong>the</strong> previouslymentioned “classic shoe dermatitis pattern”with dorsal <strong>foot</strong> involvement is <strong>the</strong><strong>foot</strong> pattern most likely to show relevantpositive reactions on patch testing. 21Conversely, some patterns are importantto recognize because <strong>of</strong> <strong>the</strong>ir relativelylow yield on patch testing. One suchpattern is symmetric involvement <strong>of</strong>both <strong>the</strong> central palms and plantar feet.This pattern is more likely to be an endogenouseczema or psoriasis and has alower yield on patch testing for relevantpositive reactions.It is also important to know how tointerpret positive results. For example,nickel is a commonly tested and frequentlypositive allergen, but <strong>the</strong> relevance<strong>of</strong> nickel allergy is somewhatunclear when considering <strong>foot</strong> dermatitis.Dimethylglyoxime-positive metalsnaps, fasteners, buckles or islets may berelevant in a patient with <strong>foot</strong> dermatitisand a positive patch test to nickel.Some reports also suggest that systemicnickel exposure in an allergic patientcan present as a dyshidrotic hand and<strong>foot</strong> eczema. 22,23 Outside <strong>of</strong> <strong>the</strong>se twosettings, a positive nickel patch test mayonly represent past sensitization withoutcurrent relevance. Similarly, a positivereaction to fragrance, neomycin,bacitracin or corticosteroid may or mayTable 3. ExPanded Shoe Series 15Allergen FocusAdhesivesp-tert-butylphenol-formaldehyde resinColophonyEpoxy ResinBenzoyl PeroxideDyesParaphenylendiamineDisperse Blue 106 or 124Rubber ComponentsBlack Rubber MixCarba MixMercaptobenzothiazole or Mercapto MixThiourea MixThiuram MixDithiodimorpholineLea<strong>the</strong>r Tanning AgentsPotassium DichromateGlutaraldehydeFormaldehydenot currently be relevant. Evaluation<strong>of</strong> relevance for allergens that are notcore components <strong>of</strong> <strong>foot</strong>wear like <strong>the</strong>above allergens requires that <strong>the</strong> presence<strong>of</strong> retained allergens be excluded.For example, odor-eliminating powdersand sprays may be a source <strong>of</strong> fragranceretention in <strong>foot</strong>wear. Similarly, topicalmedicaments are frequently applied to<strong>the</strong> feet and it is possible for <strong>the</strong>se medicamentsto become embedded into <strong>the</strong>sock and <strong>foot</strong>wear. 24,25When determining what allergensto test, a standard series to screen forcommon shoe allergens and occult allergens,such as those described in <strong>the</strong>previous paragraph, is useful. However,it is also important to expand testingbeyond this standard series. It has beenshown that, in 12.7% <strong>of</strong> patients with<strong>foot</strong> dermatitis, <strong>the</strong> NACDG standardseries failed to identify any relevantallergens. 14 This number <strong>of</strong> non-reactorsis reduced when testing includessamples taken directly from <strong>the</strong> patient’ssocks and shoes. 12,14 Samplescan be taken from <strong>foot</strong>wear with an8-mm punch, <strong>the</strong>reby yielding piecesequal in size to a standard 8-mm Finnchamber. In addition, it is <strong>of</strong>ten helpfulto utilize an expanded shoe series.A good series will adequately screenfor sensitivity to adhesives, dyes, rubbercomponents and lea<strong>the</strong>r tanningagents, which may not be included onsome standard series. Table 3 high-November 2012 | <strong>The</strong> <strong>Dermatologist</strong> ® | www.<strong>the</strong>-dermatologist.com 23