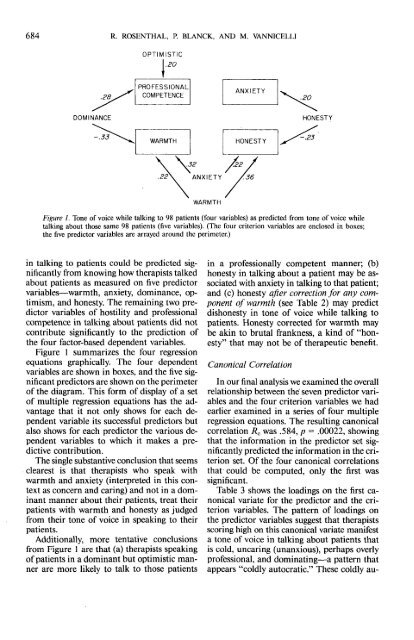
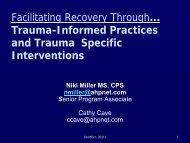
684 R. ROSENTHAL, P. BLANCK, AND M. VANNICELLIOPTIMISTIC.2032 /2222\ "ANXIETY /36WARMTHFigure 1. <strong>Tone</strong> <strong>of</strong> voice while talking <strong>to</strong> 98 patients (four variables) as predicted from <strong>to</strong>ne <strong>of</strong> voice whiletalking about those same 98 patients (five variables). (The four criterion variables are enclosed in boxes;the five predic<strong>to</strong>r variables are arrayed around the perimeter.)in talking <strong>to</strong> patients could be predicted significantlyfrom knowing how therapists talkedabout patients as measured on five predic<strong>to</strong>rvariables—warmth, anxiety, dominance, optimism,<strong>and</strong> honesty. The remaining two predic<strong>to</strong>rvariables <strong>of</strong> hostility <strong>and</strong> pr<strong>of</strong>essionalcompetence in talking about patients did notcontribute significantly <strong>to</strong> the prediction <strong>of</strong>the four fac<strong>to</strong>r-based dependent variables.Figure 1 summarizes the four regressionequations graphically. The four dependentvariables are shown in boxes, <strong>and</strong> the five significantpredic<strong>to</strong>rs are shown on the perimeter<strong>of</strong> the diagram. This form <strong>of</strong> display <strong>of</strong> a se<strong>to</strong>f multiple regression equations has the advantagethat it not only shows for each dependentvariable its successful predic<strong>to</strong>rs butalso shows for each predic<strong>to</strong>r the various dependentvariables <strong>to</strong> which it makes a predictivecontribution.The single substantive conclusion that seemsclearest is that therapists who speak withwarmth <strong>and</strong> anxiety (interpreted in this contextas concern <strong>and</strong> caring) <strong>and</strong> not in a dominantmanner about their patients, treat theirpatients with warmth <strong>and</strong> honesty as judgedfrom their <strong>to</strong>ne <strong>of</strong> voice in speaking <strong>to</strong> theirpatients.Additionally, more tentative conclusionsfrom Figure 1 are that (a) therapists speaking<strong>of</strong> patients in a dominant but optimistic mannerare more likely <strong>to</strong> talk <strong>to</strong> those patientsin a pr<strong>of</strong>essionally competent manner; (b)honesty in talking about a patient may be associatedwith anxiety in talking <strong>to</strong> that patient;<strong>and</strong> (c) honesty after correction for any componen<strong>to</strong>f warmth (see Table 2) may predictdishonesty in <strong>to</strong>ne <strong>of</strong> voice while talking <strong>to</strong>patients. Honesty corrected for warmth maybe akin <strong>to</strong> brutal frankness, a kind <strong>of</strong> "honesty"that may not be <strong>of</strong> therapeutic benefit.Canonical CorrelationIn our final analysis we examined the overallrelationship between the' seven predic<strong>to</strong>r variables<strong>and</strong> the four criterion variables we hadearlier examined in a series <strong>of</strong> four multipleregression equations. The resulting canonicalcorrelation R c was .584, p = .00022, showingthat the information in the predic<strong>to</strong>r set significantlypredicted the information in the criterionset. Of the four canonical correlationsthat could be computed, only the first wassignificant.Table 3 shows the loadings on the first canonicalvariate for the predic<strong>to</strong>r <strong>and</strong> the criterionvariables. The pattern <strong>of</strong> loadings onthe predic<strong>to</strong>r variables suggest that therapistsscoring high on this canonical variate manifesta <strong>to</strong>ne <strong>of</strong> voice in talking about patients thatis cold, uncaring (unanxious), perhaps overlypr<strong>of</strong>essional, <strong>and</strong> dominating—a pattern thatappears "coldly au<strong>to</strong>cratic." These coldly au-
SPEAKING TO AND ABOUT PATIENTS 685Table 3<strong>Predicting</strong> <strong>Therapists'</strong> <strong>Tone</strong> <strong>of</strong> <strong>Voice</strong> WhileTalking <strong>to</strong> 98 <strong>Patients</strong> From <strong>Therapists'</strong> <strong>Tone</strong> <strong>of</strong><strong>Voice</strong> While Talking <strong>About</strong> Those Same 98<strong>Patients</strong>: Canonical CorrelationPredic<strong>to</strong>r variableCriterion variableVariable Loading Variable LoadingPr<strong>of</strong>essionalism-Pr<strong>of</strong>essionalism-Competence .343 Competence .392Warmth -.427 Warmth -.719Absence <strong>of</strong>hostility .081 Anxiety -.082Anxiety -.490 Honesty -.516Dominance .490Optimism -.044Honesty -.131<strong>to</strong>cratic speakers about patients when speaking<strong>to</strong> patients are characterized as being cold,dishonest, <strong>and</strong> again, perhaps overly pr<strong>of</strong>essionalor "coldly pr<strong>of</strong>essional." In short, therapistswho speak <strong>of</strong> patients in a coldly au<strong>to</strong>craticway tend <strong>to</strong> speak <strong>to</strong> those patients ina coldly pr<strong>of</strong>essional way.The canonical correlation <strong>of</strong> .584 is the correlationbetween the canonical variates not theoriginal variables considered as sets. If wewant the correlation between the two sets <strong>of</strong>variables, we compute an index called^redundancy (Stewart & Love, 1968; Tucker& Chase, 1980). For the present data that correlationwas .388 considering all four canonicalvariates <strong>and</strong> .284 considering only the first canonicalvariate.The magnitudes <strong>of</strong> relationship found inthe present clinical context are quite comparable<strong>to</strong> those found in other clinical contextssuch as psychotherapy outcome research(Smith & Glass, 1977; Smith, Glass, & Miller,1980) <strong>and</strong> in other areas assessing the effects<strong>of</strong> nonverbal processes <strong>of</strong> social influence suchas the effects <strong>of</strong> interpersonal expectations(Rosenthal, 1966; Rosenthal & Jacobson,1968; Rosenthal & Rubin, 1978).ConclusionThe present study shows that therapists' <strong>to</strong>ne<strong>of</strong> voice in talking about patients can be used<strong>to</strong> make significantly accurate predictionsabout therapists' <strong>to</strong>ne <strong>of</strong> voice in talking <strong>to</strong>patients. Our research shows, furthermore,that these predictions are characterized by discriminantvalidity as well as predictive validity.The predictions about therapists' <strong>to</strong>ne <strong>of</strong> voiceare not only significant statistically but alsopractically meaningful in magnitude. Correlationsbased on the median simple, the medianmultiple, <strong>and</strong> the cumulative canonicalcorrelations were .24, .38, <strong>and</strong> .39, respectively.These correlations are associated with improvementsin prediction from 38% <strong>to</strong> 62%,from 31% <strong>to</strong> 69%, <strong>and</strong> from 30.5% <strong>to</strong> 69.5%,respectively (Rosenthal & Rubin, 1982). Inshort, these correlations, which are about ashigh as are usually obtained in clinical research<strong>of</strong> this type (Cohen, 1977, page 81), might wellbe <strong>of</strong> practical utility if their magnitude holdsup on replication.We are intrigued by the possibility that suchbrief clips <strong>of</strong> content-filtered speech might beuseful not only for further research on psychotherapeuticprocess but also, in the future,for the selection <strong>and</strong> supervision <strong>of</strong> therapistsas well.ReferencesAmerican Psychiatric Association. (1980). Diagnostic <strong>and</strong>statistical manual <strong>of</strong> mental disorders (3rd ed.). Washing<strong>to</strong>n,DC: Author.Blanck, P. D., & Rosenthal, R. (in press). The mediation<strong>of</strong> interpersonal expectancy effects: The counselor's <strong>to</strong>ne<strong>of</strong> voice. Journal <strong>of</strong> Educational Psychology.Blanck, P. D., Rosenthal, R., & Vannicelli, M. (1983).The fac<strong>to</strong>r structure <strong>of</strong> the therapist's <strong>to</strong>ne <strong>of</strong> voice. Unpublishedmanuscript, Harvard University, Cambridge,MA.Blanck, P. D., Rosenthal, R., Vanicelli, M., & Lee, T. D.(1983). Therapist's <strong>to</strong>ne <strong>of</strong> voice as predic<strong>to</strong>r <strong>of</strong> psychotherapeuticprocess: The first few seconds. Unpublishedmanuscript, Harvard University, Cambridge, MA.Caporael, L. R., Lukaszewski, M. P., & Culbertson, G.H. (1983). Secondary baby talk: Judgments by institutionalizedelderly <strong>and</strong> their caregivers. Journal <strong>of</strong> Personality<strong>and</strong> Social Psychology, 44, 746-754.Cohen, J. (1977). Statistical power analysis for the behavioralsciences (rev. ed.). NY: Academic Press.Davitz, J. R. (1964). The communication <strong>of</strong> emotionalmeaning. NY: McGraw-Hill.DePaulo, B. M., & Rosenthal, R. (1979). Ambivalence,discrepancy, <strong>and</strong> deception in nonverbal communication.In R. Rosenthal (Ed.), Skill in nonverbal communication:Individual differences (pp. 204-248).Cambridge, MA: Oelgeschlager, Gunn & Hain.DiMatteo, M. R. (1979). Nonverbal skill <strong>and</strong> the physicianpatientrelationship. In R. Rosenthal (Ed.), Skill in nonverbalcommunication: Individual differences (pp. 104-134). Cambridge, MA: Oelgeschlager, Gunn & Hain.Duncan, S., Jr., Rice, L. N., & Butler, J. M. (1968). <strong>Therapists'</strong>paralanguage in peak <strong>and</strong> poor psychotherapyhours. Journal <strong>of</strong> Abnormal Psychology, 73, 566-570.