

TEMPORALIS MUSCLE FLAP - Vula - University of Cape Town
TEMPORALIS MUSCLE FLAP - Vula - University of Cape Town
TEMPORALIS MUSCLE FLAP - Vula - University of Cape Town

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
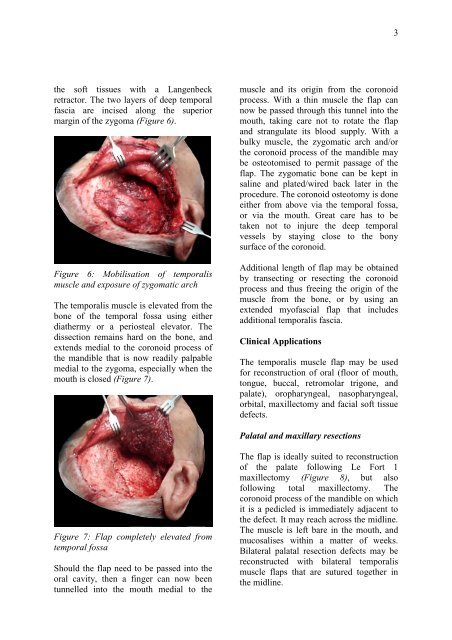
3the s<strong>of</strong>t tissues with a Langenbeckretractor. The two layers <strong>of</strong> deep temporalfascia are incised along the superiormargin <strong>of</strong> the zygoma (Figure 6).Figure 6: Mobilisation <strong>of</strong> temporalismuscle and exposure <strong>of</strong> zygomatic archThe temporalis muscle is elevated from thebone <strong>of</strong> the temporal fossa using eitherdiathermy or a periosteal elevator. Thedissection remains hard on the bone, andextends medial to the coronoid process <strong>of</strong>the mandible that is now readily palpablemedial to the zygoma, especially when themouth is closed (Figure 7).muscle and its origin from the coronoidprocess. With a thin muscle the flap cannow be passed through this tunnel into themouth, taking care not to rotate the flapand strangulate its blood supply. With abulky muscle, the zygomatic arch and/orthe coronoid process <strong>of</strong> the mandible maybe osteotomised to permit passage <strong>of</strong> theflap. The zygomatic bone can be kept insaline and plated/wired back later in theprocedure. The coronoid osteotomy is doneeither from above via the temporal fossa,or via the mouth. Great care has to betaken not to injure the deep temporalvessels by staying close to the bonysurface <strong>of</strong> the coronoid.Additional length <strong>of</strong> flap may be obtainedby transecting or resecting the coronoidprocess and thus freeing the origin <strong>of</strong> themuscle from the bone, or by using anextended my<strong>of</strong>ascial flap that includesadditional temporalis fascia.Clinical ApplicationsThe temporalis muscle flap may be usedfor reconstruction <strong>of</strong> oral (floor <strong>of</strong> mouth,tongue, buccal, retromolar trigone, andpalate), oropharyngeal, nasopharyngeal,orbital, maxillectomy and facial s<strong>of</strong>t tissuedefects.Palatal and maxillary resectionsFigure 7: Flap completely elevated fromtemporal fossaShould the flap need to be passed into theoral cavity, then a finger can now beentunnelled into the mouth medial to theThe flap is ideally suited to reconstruction<strong>of</strong> the palate following Le Fort 1maxillectomy (Figure 8), but als<strong>of</strong>ollowing total maxillectomy. Thecoronoid process <strong>of</strong> the mandible on whichit is a pedicled is immediately adjacent tothe defect. It may reach across the midline.The muscle is left bare in the mouth, andmucosalises within a matter <strong>of</strong> weeks.Bilateral palatal resection defects may bereconstructed with bilateral temporalismuscle flaps that are sutured together inthe midline.













