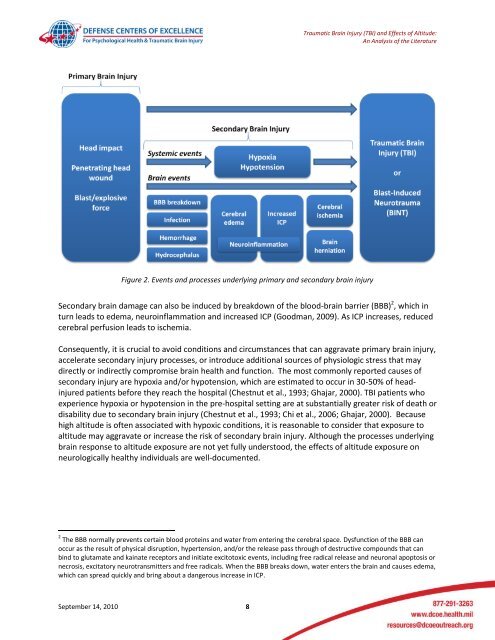
<strong>Traumatic</strong> <strong>Brain</strong> <strong>Injury</strong> (TBI) <strong>and</strong> <strong>Effects</strong> <strong>of</strong> <strong>Altitude</strong>:An Analysis <strong>of</strong> the LiteratureFigure 2. Events <strong>and</strong> processes underlying primary <strong>and</strong> secondary brain injurySecondary brain damage can also be induced by breakdown <strong>of</strong> the blood-brain barrier (BBB) 2 , which inturn leads to edema, neuroinflammation <strong>and</strong> increased ICP (Goodman, 2009). As ICP increases, reducedcerebral perfusion leads to ischemia.Consequently, it is crucial to avoid conditions <strong>and</strong> circumstances that can aggravate primary brain injury,accelerate secondary injury processes, or introduce additional sources <strong>of</strong> physiologic stress that maydirectly or indirectly compromise brain health <strong>and</strong> function. The most commonly reported causes <strong>of</strong>secondary injury are hypoxia <strong>and</strong>/or hypotension, which are estimated to occur in 30-50% <strong>of</strong> headinjuredpatients before they reach the hospital (Chestnut et al., 1993; Ghajar, 2000). TBI patients whoexperience hypoxia or hypotension in the pre-hospital setting are at substantially greater risk <strong>of</strong> death ordisability due to secondary brain injury (Chestnut et al., 1993; Chi et al., 2006; Ghajar, 2000). Becausehigh altitude is <strong>of</strong>ten associated with hypoxic conditions, it is reasonable to consider that exposure toaltitude may aggravate or increase the risk <strong>of</strong> secondary brain injury. Although the processes underlyingbrain response to altitude exposure are not yet fully understood, the effects <strong>of</strong> altitude exposure onneurologically healthy individuals are well-documented.2 The BBB normally prevents certain blood proteins <strong>and</strong> water from entering the cerebral space. Dysfunction <strong>of</strong> the BBB canoccur as the result <strong>of</strong> physical disruption, hypertension, <strong>and</strong>/or the release pass through <strong>of</strong> destructive compounds that canbind to glutamate <strong>and</strong> kainate receptors <strong>and</strong> initiate excitotoxic events, including free radical release <strong>and</strong> neuronal apoptosis ornecrosis, excitatory neurotransmitters <strong>and</strong> free radicals. When the BBB breaks down, water enters the brain <strong>and</strong> causes edema,which can spread quickly <strong>and</strong> bring about a dangerous increase in ICP.September 14, 2010 8
<strong>Traumatic</strong> <strong>Brain</strong> <strong>Injury</strong> (TBI) <strong>and</strong> <strong>Effects</strong> <strong>of</strong> <strong>Altitude</strong>:An Analysis <strong>of</strong> the LiteratureClinical Parameters <strong>of</strong> TBI at <strong>Altitude</strong>Neurons respond to oxygen deprivation in the order <strong>of</strong> milliseconds. Because the brain is the mostoxygen-dependent organ in the body, it is the first organ to be affected by reduced oxygen delivery athigh altitude. The concentration <strong>of</strong> oxygen in air is constant at 20.9% up to about 12, 000 meters, but asone ascends in altitude, barometric pressure decreases <strong>and</strong> causes a reduction in the partial pressure 3 <strong>of</strong>oxygen. This is referred to as hypobaric hypoxia. At 5500 meters (about 18,000 feet) above sea level, thepartial pressure <strong>of</strong> oxygen is reduced to about half its value at sea level; at 8800 meters (about 29,000feet) it is reduced to a third <strong>of</strong> its sea level value.When the body is subjected to hypobaric hypoxia, less oxygen can move from the airspace <strong>of</strong> the lungsinto the blood. Low arterial PO 2 causes vasodilation in the brain (Borgstrom et al., 1975), which alterscerebral blood flow. The precise underlying mechanisms <strong>and</strong> processes 4 <strong>of</strong> altitude-related changes inthe brain are not yet fully understood, but the results are similar to the events that trigger secondaryinjury cascades following TBI. These include cerebral edema, increased ICP, compromised perfusion,ischemic injury, <strong>and</strong> apoptosis 5 . Therefore, individuals who sustain TBI at high altitude, or who must betransported at high altitude, are placed at additional risk for secondary hypoxic tissue injury. Thispresents a unique challenge for those who provide acute medical care <strong>and</strong> transport.High-altitude illness refers to a spectrum <strong>of</strong> syndromes that can develop in otherwise healthy individualsshortly after ascent to high (1500-3500 meters), very high (3500-5500 meters) or extreme (above 5500meters) altitudes. Neurological effects vary widely among individuals. Symptoms such as headache <strong>and</strong>altered night vision can develop in some individuals at as little as 1500 meters (approximately 5000feet), which is the altitude equivalent inside a pressurized commercial aircraft. In general, though,neurological effects are more likely to occur at altitudes above 2500 meters (approximately 8000 feet).Prevention <strong>of</strong> altitude illness depends on slow ascent, prompt recognition <strong>of</strong> signs <strong>and</strong> symptoms,supplementary oxygen <strong>and</strong> descent to lower altitude to avoid worsening effects.Three altitude-related syndromes have been identified: acute mountain sickness; high altitude cerebraledema; <strong>and</strong> high altitude pulmonary cerebral edema. Acute mountain sickness (AMS) involves a variety<strong>of</strong> non-specific symptoms such as headache, fatigue, dizziness, nausea, vomiting, <strong>and</strong>/or sleepdisturbance. Typically, one or more <strong>of</strong> these symptoms develop 6-12 hours after arrival at altitude; theyare easily confused with effects <strong>of</strong> exhaustion, migraine, dehydration or hypothermia. Some individualsexperience discomfort <strong>and</strong>/or AMS at as low as 2400 meters (8000 feet) (Muhm et al., 2007). Withoutthe benefit <strong>of</strong> supplemental oxygen, AMS affects about half (53%) <strong>of</strong> those who trek (walk) to heights <strong>of</strong>4000 - 5000 meters (13, 000-16, 000 feet; Hackett et al., 1976; Verdy & Judge, 2006). Rapid ascentdramatically increases the risk <strong>of</strong> developing altitude-related high-altitude illness (Hackett et al., 1976),3 In a gas mixture (in this case, air), partial pressure <strong>of</strong> oxygen refers to the pressure it would have if it occupied the samevolume, alone, at the same temperature.4 A detailed analysis <strong>of</strong> the cellular basis <strong>and</strong> pathophysiological mechanisms underlying these <strong>and</strong> related effects is beyond thescope <strong>of</strong> this report; these have been discussed at length by other authors (Bailey et al., 2009; Basnyat & Murdoch, 2003;Finn<strong>of</strong>f, 2008; Goodman et al., 2009; Kushi et al., 2003; Schmidt et al., 2005; Wilson et al., 2009).5 Apoptosis is a type <strong>of</strong> programmed cell death involving a series <strong>of</strong> biochemical events which lead to the death <strong>of</strong> cells. Theprocesses associated with apoptosis do not damage the organism. By contrast, necrosis is a form <strong>of</strong> traumatic cell death thatresults from acute cellular injury.September 14, 2010 9



![Body Composition and Military [PDF] - Human Performance ...](https://img.yumpu.com/43269347/1/190x245/body-composition-and-military-pdf-human-performance-.jpg?quality=85)
![Tips for Grocery Shopping [PDF]](https://img.yumpu.com/37447379/1/190x245/tips-for-grocery-shopping-pdf.jpg?quality=85)



![Synthetic Drugs [PDF] - Human Performance Resource Center](https://img.yumpu.com/37447322/1/190x245/synthetic-drugs-pdf-human-performance-resource-center.jpg?quality=85)