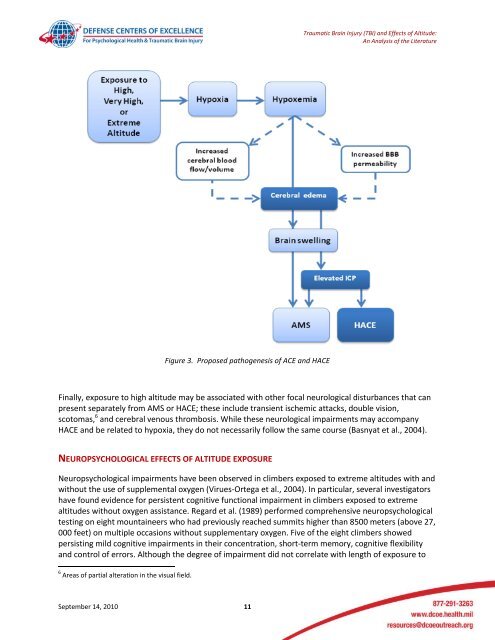
<strong>Traumatic</strong> <strong>Brain</strong> <strong>Injury</strong> (TBI) <strong>and</strong> <strong>Effects</strong> <strong>of</strong> <strong>Altitude</strong>:An Analysis <strong>of</strong> the Literaturewith AMS affecting more than four out <strong>of</strong> five individuals who fly directly to above 3800 meters (about12, 500 feet) (Basnyat & Murdoch, 2003).Individuals who develop symptoms <strong>of</strong> AMS should not ascend further, <strong>and</strong> should descend if theirsymptoms worsen or fail to improve. Immediate descent is critical if cerebral or pulmonary symptomsappear. Supplemental oxygen may help to relieve AMS symptoms.High-altitude cerebral edema (HACE) is relatively unusual, with prevalence estimated at between 0.5%<strong>and</strong> 4.0% <strong>of</strong> individuals who climb to altitudes above 2500 meters (8000 feet). However, because theprecise pathophysiology <strong>of</strong> neither syndrome is fully understood <strong>and</strong> because the incidence <strong>of</strong> HACE isdramatically less than that <strong>of</strong> AMS, it is not clear that the two syndromes reflect identical processes orvulnerabilities. Signs <strong>and</strong> symptoms <strong>of</strong> HACE may include dizziness, intense weakness, tingling, ataxia,altered consciousness, papilloedema (optic disc swelling), retinal hemorrhages <strong>and</strong> focal neurologicaldeficits. These symptoms can develop very quickly <strong>and</strong> are potentially fatal. As symptoms develop, thetime to loss <strong>of</strong> consciousness may be as little as 1-10 minutes (Clarke, 2006). Treatment requiresimmediate descent <strong>and</strong> oxygen supplementation. If HACE is not promptly managed <strong>and</strong> relieved, it canlead to brain herniation, coma, <strong>and</strong> death. Because HACE is usually preceded by AMS symptoms, it is<strong>of</strong>ten regarded as the “end stage” <strong>of</strong> AMS.The precise pathophysiological bases <strong>of</strong> AMS <strong>and</strong> HACE are not known, <strong>and</strong> are difficult to ascertainpartly due to individual differences. When these syndromes occur, they appear to follow from a series<strong>of</strong> systemic <strong>and</strong> cerebral changes that may involve increased cerebral blood flow (due to hypoxia)<strong>and</strong>/or vasogenic edema, both <strong>of</strong> which can cause to brain swelling <strong>and</strong> raised ICP (see Figure 3, below).Vasogenic edema has been observed in cases <strong>of</strong> moderate to severe AMS <strong>and</strong> HACE, perhaps due todisruption <strong>of</strong> BBB permeability. These <strong>and</strong> related hypotheses are the focus <strong>of</strong> continuing research,analysis, <strong>and</strong> review (Basnyat & Murdoch, 2003; Hackett, 1999a, 1999b; Hackett & Roach, 2001; Roach& Hackett, 2001; West, 2004; Wilson et al., 2009).Treatment with dexamethasone (anti-inflammatory steroid) is sometimes recommended to treat HACE(Schoene, 2005). However, recent clinical research suggests that steroids have no clear beneficial effecton TBI <strong>and</strong> may even have deleterious effects; therefore, steroids are NOT recommended for reducingICP in individuals who have sustained traumatic brain injury (TBI) (Bullock & Povlishock, 2007). Otherpharmacotherapeutic options for the prevention <strong>and</strong> treatment <strong>of</strong> altitude-related illnesses in otherwisehealthy individuals are reviewed elsewhere (Wilson et al., 2009; Wright et al., 2008).A third altitude-related illness is known as high-altitude pulmonary edema (HAPE), which usuallypresents in the first 24-48 hours after arrival at altitudes higher than 2500 meters (approximately 8000feet). HAPE may or may not follow AMS, but <strong>of</strong>ten co-occurs with signs <strong>of</strong> HACE. HAPE is a cardiopulmonarysyndrome that usually appears first as dyspnea (shortness <strong>of</strong> breath) <strong>and</strong> reduced tolerance forexercise. This can lead to dry cough (which can later become productive), tachypnea (rapid breathing),tachycardia (rapid heart rate) <strong>and</strong> fever. Cold is a risk factor for HAPE. HAPE is more common in menthan in women, <strong>and</strong> in individuals with pre-existing cardiopulmonary circulation abnormalities. Again,descent <strong>and</strong> supplemental oxygen are the recommended treatments.September 14, 2010 10
<strong>Traumatic</strong> <strong>Brain</strong> <strong>Injury</strong> (TBI) <strong>and</strong> <strong>Effects</strong> <strong>of</strong> <strong>Altitude</strong>:An Analysis <strong>of</strong> the LiteratureFigure 3. Proposed pathogenesis <strong>of</strong> ACE <strong>and</strong> HACEFinally, exposure to high altitude may be associated with other focal neurological disturbances that canpresent separately from AMS or HACE; these include transient ischemic attacks, double vision,scotomas, 6 <strong>and</strong> cerebral venous thrombosis. While these neurological impairments may accompanyHACE <strong>and</strong> be related to hypoxia, they do not necessarily follow the same course (Basnyat et al., 2004).NEUROPSYCHOLOGICAL EFFECTS OF ALTITUDE EXPOSURENeuropsychological impairments have been observed in climbers exposed to extreme altitudes with <strong>and</strong>without the use <strong>of</strong> supplemental oxygen (Virues-Ortega et al., 2004). In particular, several investigatorshave found evidence for persistent cognitive functional impairment in climbers exposed to extremealtitudes without oxygen assistance. Regard et al. (1989) performed comprehensive neuropsychologicaltesting on eight mountaineers who had previously reached summits higher than 8500 meters (above 27,000 feet) on multiple occasions without supplementary oxygen. Five <strong>of</strong> the eight climbers showedpersisting mild cognitive impairments in their concentration, short-term memory, cognitive flexibility<strong>and</strong> control <strong>of</strong> errors. Although the degree <strong>of</strong> impairment did not correlate with length <strong>of</strong> exposure to6 Areas <strong>of</strong> partial alteration in the visual field.September 14, 2010 11



![Body Composition and Military [PDF] - Human Performance ...](https://img.yumpu.com/43269347/1/190x245/body-composition-and-military-pdf-human-performance-.jpg?quality=85)
![Tips for Grocery Shopping [PDF]](https://img.yumpu.com/37447379/1/190x245/tips-for-grocery-shopping-pdf.jpg?quality=85)



![Synthetic Drugs [PDF] - Human Performance Resource Center](https://img.yumpu.com/37447322/1/190x245/synthetic-drugs-pdf-human-performance-resource-center.jpg?quality=85)