Biochemical markers in the diagnosis of acute ischaemic stroke
Biochemical markers in the diagnosis of acute ischaemic stroke
Biochemical markers in the diagnosis of acute ischaemic stroke

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
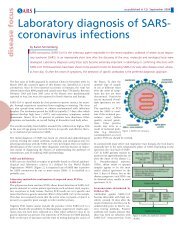
M arkers <strong>of</strong> Strokeas published <strong>in</strong> CLI November 2004analyte<strong>of</strong> <strong>the</strong> monthWith <strong>the</strong> development <strong>of</strong> effective <strong>the</strong>rapeutic <strong>in</strong>terventions for <strong>ischaemic</strong> <strong>stroke</strong>, <strong>the</strong> rapid<strong>diagnosis</strong> <strong>of</strong> cerebral ischaemia has become a priority <strong>in</strong> <strong>the</strong> management <strong>of</strong> <strong>the</strong> disease. In thisbrief review, we discuss <strong>the</strong> role <strong>of</strong> biochemical <strong>markers</strong> <strong>in</strong> <strong>the</strong> pathogenesis <strong>of</strong> <strong>stroke</strong>, as wellas recent data demonstrat<strong>in</strong>g that <strong>the</strong> measurement <strong>of</strong> biochemical <strong>markers</strong> <strong>in</strong> <strong>the</strong> blood is analternate approach to sensitive but costly neuroimag<strong>in</strong>g techniques for <strong>the</strong> early <strong>diagnosis</strong> <strong>of</strong><strong>ischaemic</strong> <strong>stroke</strong>.<strong>Biochemical</strong> <strong>markers</strong> <strong>in</strong> <strong>the</strong><strong>diagnosis</strong> <strong>of</strong> <strong>acute</strong> <strong>ischaemic</strong> <strong>stroke</strong>by James Floyd and Dr. Daniel LaskowitzTreatment for <strong>stroke</strong> is dependent on whe<strong>the</strong>r <strong>the</strong><strong>stroke</strong> is <strong>ischaemic</strong> or haemorrhagic, and <strong>the</strong>refore<strong>diagnosis</strong> with<strong>in</strong> <strong>the</strong> first six hours after onset <strong>of</strong>symptoms is essential if patients with <strong>ischaemic</strong><strong>stroke</strong> are to benefit from t-PA <strong>the</strong>rapy. Standardneuroimag<strong>in</strong>g techniques, such as computedtomography (CT) and magnetic resonance imag<strong>in</strong>g(MRI), and models based on cl<strong>in</strong>ical data have allbeen evaluated <strong>in</strong> <strong>the</strong> <strong>diagnosis</strong> <strong>of</strong> <strong>stroke</strong>. However,<strong>the</strong>y are <strong>in</strong>sufficiently accurate to serve as reliablediagnostic tests. Although newer, more sensitiveimag<strong>in</strong>g modalities are be<strong>in</strong>g developed and validated,<strong>the</strong>y are time-consum<strong>in</strong>g and are typicallyavailable only <strong>in</strong> academic centres and <strong>in</strong>stitutionswith <strong>stroke</strong> units. Measurement <strong>of</strong> biochemical<strong>markers</strong> <strong>in</strong> <strong>the</strong> blood is an alternative approach.Mechanisms <strong>of</strong> <strong>in</strong>jury from cerebral ischaemiaAcute cerebral ischaemia is caused by <strong>the</strong> occlusion<strong>of</strong> a cerebral blood vessel, result<strong>in</strong>g <strong>in</strong> decreasedblood flow to <strong>the</strong> bra<strong>in</strong>. As blood flow falls belowthreshold levels, normal neuronal function beg<strong>in</strong>sto fail and a host <strong>of</strong> molecular and cellular changesleads to cerebral <strong>in</strong>farction.One <strong>of</strong> <strong>the</strong> first events to occur is energy failurefrom reduced ATP syn<strong>the</strong>sis. The subsequentimpairment <strong>of</strong> ion homeostasis and <strong>the</strong> presence <strong>of</strong>excess extracellular glutamate result <strong>in</strong> neuronaldepolarisation, trigger<strong>in</strong>g an <strong>in</strong>flux <strong>of</strong> calciumthrough voltage-gated channels. Intracellular calciumoverload promotes numerous enzyme-dependentprocesses that lead to or exacerbate neuronal celldeath, <strong>in</strong>clud<strong>in</strong>g <strong>the</strong> production <strong>of</strong> reactive oxygenspecies. Free radicals are generated <strong>in</strong> <strong>the</strong> oxygendeprivedenvironment, damag<strong>in</strong>g prote<strong>in</strong>s, DNA,and lipids. Conversion from aerobic respiration toanaerobic glycolysis results <strong>in</strong> lactic acidosis, whichfur<strong>the</strong>r contributes to tissue damage by promot<strong>in</strong>g<strong>in</strong>tracellular oedema and impair<strong>in</strong>g mitochondrialrespiration [1].After <strong>the</strong>se early mechanisms <strong>of</strong> <strong>in</strong>jury have been<strong>in</strong>itiated, apoptosis and <strong>in</strong>flammation mediate fur<strong>the</strong>rtissue <strong>in</strong>jury after ischaemia. Apoptosis, or programmedcell death, occurs primarily with<strong>in</strong> <strong>the</strong><strong>ischaemic</strong> penumbra but also with<strong>in</strong> <strong>the</strong> <strong>ischaemic</strong>core. Although apoptosis occurs for many days aftercerebral ischaemia, upregulation <strong>of</strong> caspases, <strong>the</strong>enzymatic mediators <strong>of</strong> this process, is evidentwith<strong>in</strong> hours <strong>of</strong> <strong>the</strong> <strong>in</strong>itial <strong>in</strong>sult. The <strong>in</strong>flammatoryresponse is characterised by <strong>the</strong> migration <strong>of</strong>leukoctyes - first neutrophils and <strong>the</strong>n macrophages- <strong>in</strong>to <strong>the</strong> bra<strong>in</strong>, where <strong>the</strong>y exert <strong>the</strong>ir damag<strong>in</strong>geffects by releas<strong>in</strong>g toxic substances, modulat<strong>in</strong>g <strong>the</strong>vasoreactivity <strong>of</strong> cerebral vessels, and through <strong>the</strong>irphagocytic activity. This is preceded by <strong>the</strong> production<strong>of</strong> many different cytok<strong>in</strong>es by glial cells, leukocytes,and endo<strong>the</strong>lial cells. Cytok<strong>in</strong>es attract leukocytesand stimulate <strong>the</strong> production <strong>of</strong> adhesionmolecules on leukocytes and endo<strong>the</strong>lial cells, facilitat<strong>in</strong>gmigration across <strong>the</strong> blood-bra<strong>in</strong> barrier [2].<strong>Biochemical</strong> <strong>markers</strong> <strong>in</strong> cerebral ischaemiaMany biochemical <strong>markers</strong> that correlate with cerebralischaemia have been identified [Table 1].Although much <strong>of</strong> <strong>the</strong> data on <strong>the</strong>se <strong>markers</strong> derivefrom animal models, this article will discuss onlyhuman studies, and primarily those that <strong>in</strong>volveblood measurements.Neuron-specific enolase (NSE) is an enzyme found<strong>in</strong> <strong>the</strong> cytoplasm <strong>of</strong> neurons and neuroendocr<strong>in</strong>ecells that has been studied extensively as a marker <strong>of</strong>neuronal <strong>in</strong>jury. Levels <strong>of</strong> this enzyme are elevated<strong>in</strong> <strong>the</strong> blood and CSF <strong>of</strong> patients present<strong>in</strong>g with<strong>ischaemic</strong> <strong>stroke</strong>, and <strong>the</strong>y correlate with <strong>in</strong>farctsize. Glial acidic fibrillary prote<strong>in</strong> (GFAP) andS100β are two <strong>markers</strong> <strong>of</strong> glial activation that havebeen evaluated <strong>in</strong> <strong>the</strong> sett<strong>in</strong>g <strong>of</strong> cerebral ischaemia.Serum levels <strong>of</strong> both prote<strong>in</strong>s are elevated as early aswith<strong>in</strong> 8 hours after symptom onset, correlat<strong>in</strong>gwith <strong>in</strong>farct size and functional outcome, as well aswith each o<strong>the</strong>r.The pr<strong>of</strong>ile <strong>of</strong> various <strong>in</strong>flammatory mediators <strong>in</strong><strong>the</strong> blood dur<strong>in</strong>g cerebral ischaemia has been studiedextensively <strong>in</strong> <strong>the</strong> cl<strong>in</strong>ical sett<strong>in</strong>g [2, 3]. Inhumans, blood levels <strong>of</strong> <strong>the</strong> cytok<strong>in</strong>es <strong>in</strong>terleuk<strong>in</strong>-1receptor antagonist (IL-1ra), <strong>in</strong>terleuk<strong>in</strong>-6 (IL-6),and tumour necrosis factor-α (TNF-α) become elevatedafter <strong>ischaemic</strong> <strong>stroke</strong>, and for IL-6 <strong>the</strong>sechanges occur with<strong>in</strong> a few hours <strong>of</strong> symptomonset. Monocyte chemoattractant prote<strong>in</strong>-1 (MCP-1), a chemok<strong>in</strong>e that attracts mononuclear leukoctyes,is elevated <strong>in</strong> <strong>the</strong> CSF <strong>of</strong> <strong>stroke</strong> patients present<strong>in</strong>gwith<strong>in</strong> 24 hours <strong>of</strong> symptom onset, but not<strong>in</strong> <strong>the</strong> blood. In a study <strong>of</strong> circulat<strong>in</strong>g levels <strong>of</strong> solubleselect<strong>in</strong>- and immunoglobul<strong>in</strong>-type adhesionmolecules <strong>in</strong> patients with <strong>ischaemic</strong> <strong>stroke</strong>, vascularcell adhesion molecule-1 (VCAM-1) was foundto be elevated with<strong>in</strong> 4 hours <strong>of</strong> symptom onset andendo<strong>the</strong>lial leukocyte adhesion molecule-1 (ELAM-1) with<strong>in</strong> 8 hours. Elevated levels <strong>of</strong> <strong>the</strong> <strong>acute</strong> phasereactant C-reactive prote<strong>in</strong> (CRP) have been shown<strong>in</strong> multiple prospective cohort studies to correlatewith an <strong>in</strong>creased <strong>in</strong>cidence <strong>of</strong> <strong>stroke</strong>. However, thisbiochemical marker has not yet been evaluated <strong>in</strong>an <strong>acute</strong> sett<strong>in</strong>g.Different components <strong>of</strong> <strong>the</strong> coagulation systemhave also been evaluated <strong>in</strong> <strong>ischaemic</strong> <strong>stroke</strong>patients. Levels <strong>of</strong> D-dimer, a marker <strong>of</strong> plasm<strong>in</strong>activity and fibr<strong>in</strong>olysis, are elevated with<strong>in</strong> hours<strong>of</strong> onset <strong>of</strong> cerebral ischaemia and rema<strong>in</strong> so formonths, reflect<strong>in</strong>g both <strong>acute</strong> and chronic coagulationabnormalities. The coagulation factorvonWillebrand factor (vWF) has been evaluated <strong>in</strong>patients four weeks after <strong>the</strong> occurrence <strong>of</strong> transient<strong>ischaemic</strong> attack (TIA) or <strong>ischaemic</strong> <strong>stroke</strong> and as apredictive marker <strong>in</strong> a prospective cohort study.Levels <strong>of</strong> vWF are elevated after cerebral ischaemia,Table 1. Some biochemical <strong>markers</strong> associated with cerebralischaemia.
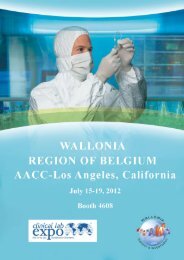
M arkers <strong>of</strong> Strokeas published <strong>in</strong> CLI November 2004imag<strong>in</strong>g modalities may be unavailable, such a test could contribute to a physician'sconfidence <strong>in</strong> adm<strong>in</strong>ister<strong>in</strong>g thrombolytic <strong>the</strong>rapy or assist <strong>in</strong> <strong>the</strong> decisionto transport patients with suspected cerebral ischaemia to a hospital with a<strong>stroke</strong> unit for fur<strong>the</strong>r evaluation. Without such a test, <strong>the</strong> <strong>diagnosis</strong> <strong>of</strong> <strong>stroke</strong>rema<strong>in</strong>s one that is made solely on cl<strong>in</strong>ical grounds <strong>in</strong> most hospitals.Table 2. <strong>Biochemical</strong> <strong>markers</strong> significantly correlated with <strong>the</strong> presence <strong>of</strong> <strong>ischaemic</strong> <strong>stroke</strong> <strong>in</strong>patients present<strong>in</strong>g with<strong>in</strong> six hours, and from 6 to 24 hours after onset <strong>of</strong> symptoms [4].The study <strong>of</strong> biochemical <strong>markers</strong> <strong>in</strong>volved <strong>in</strong> <strong>the</strong> <strong>ischaemic</strong> cascade has providedimportant <strong>in</strong>formation regard<strong>in</strong>g <strong>the</strong> pathogenesis <strong>of</strong> <strong>stroke</strong> and has identifiedpotential targets for <strong>the</strong>rapeutic <strong>in</strong>tervention. However, <strong>the</strong>se surrogate<strong>markers</strong> for cerebral ischaemia are useful as a diagnostic modality only ifpatients with <strong>ischaemic</strong> <strong>stroke</strong> can be identified with high sensitivity and specificity.A recent report <strong>of</strong> a diagnostic panel <strong>of</strong> biochemical <strong>markers</strong> [5] suggeststhat this novel approach may serve as a useful diagnostic test for <strong>ischaemic</strong><strong>stroke</strong> dur<strong>in</strong>g <strong>the</strong> <strong>acute</strong> period.and higher levels at basel<strong>in</strong>e are associated with an <strong>in</strong>creased <strong>in</strong>cidence <strong>of</strong> <strong>stroke</strong>.Various growth factors have been implicated <strong>in</strong> facilitat<strong>in</strong>g recovery after <strong>stroke</strong>,some by stimulat<strong>in</strong>g angiogenesis <strong>in</strong> regions <strong>of</strong> <strong>in</strong>farction. In post-mortemanalyses <strong>of</strong> bra<strong>in</strong> specimens, <strong>in</strong>creased expression <strong>of</strong> transform<strong>in</strong>g growth factor-β(TGF- β) and platelet-derived growth factor (PDGF) were found <strong>in</strong><strong>in</strong>farcted areas and border zones. The measurement <strong>of</strong> vascular endo<strong>the</strong>lialgrowth factor (VEGF) <strong>in</strong> <strong>the</strong> blood <strong>of</strong> <strong>ischaemic</strong> <strong>stroke</strong> patients revealed elevatedlevels on <strong>the</strong> day <strong>of</strong> admission, persist<strong>in</strong>g for two weeks. Conversely, apoptosisleads to cont<strong>in</strong>ued necrosis after cerebral ischaemia, particularly <strong>in</strong> <strong>the</strong><strong>ischaemic</strong> penumbra. Immunochemical sta<strong>in</strong><strong>in</strong>g <strong>of</strong> bra<strong>in</strong> specimens frompatients with symptomatic cerebral ischaemia demonstrated upregulation <strong>of</strong>caspase-3 <strong>in</strong> selectively vulnerable areas <strong>of</strong> <strong>the</strong> bra<strong>in</strong>.The <strong>acute</strong> time-w<strong>in</strong>dowAlthough <strong>the</strong> number <strong>of</strong> studies <strong>of</strong> biochemical <strong>markers</strong> <strong>in</strong> <strong>ischaemic</strong> <strong>stroke</strong>patients has <strong>in</strong>creased dramatically over <strong>the</strong> past few years, very few have <strong>in</strong>cludedmeasurements made dur<strong>in</strong>g <strong>the</strong> first few hours after symptom onset - a criticalperiod for <strong>the</strong>rapeutic decision-mak<strong>in</strong>g. Recently, plasma levels <strong>of</strong> 26 differentbiochemical <strong>markers</strong> have been evaluated <strong>in</strong> patients present<strong>in</strong>g <strong>acute</strong>ly withcerebral ischaemia, and compared with healthy controls [4]. These <strong>markers</strong> -many <strong>of</strong> which were exam<strong>in</strong>ed <strong>in</strong> relation to <strong>ischaemic</strong> <strong>stroke</strong> for <strong>the</strong> first time -<strong>in</strong>cluded <strong>in</strong>flammatory mediators, growth factors, and <strong>markers</strong> <strong>of</strong> glial activation,cellular <strong>in</strong>jury, myel<strong>in</strong> breakdown, thrombosis, and apoptosis. The cl<strong>in</strong>icaloutcome <strong>of</strong> <strong>ischaemic</strong> <strong>stroke</strong> was def<strong>in</strong>ed as a neurological deficit last<strong>in</strong>g longerthan 24 hours result<strong>in</strong>g from cerebral ischaemia, confirmed ei<strong>the</strong>r radiographicallyor through <strong>the</strong> exclusion <strong>of</strong> o<strong>the</strong>r aetiologies.Significant correlations between many <strong>of</strong> <strong>the</strong> biochemical <strong>markers</strong> and <strong>the</strong> presence<strong>of</strong> <strong>ischaemic</strong> <strong>stroke</strong> were demonstrated <strong>in</strong> patients with blood drawn bothbefore 6 hours and between 6 and 24 hours after symptom onset [Table 2].Although many <strong>of</strong> <strong>the</strong> <strong>in</strong>dividual correlations were excellent - as with previousstudies exam<strong>in</strong><strong>in</strong>g biochemical <strong>markers</strong> - no s<strong>in</strong>gle marker possessed <strong>the</strong> requisitepredictive capacity for it to serve as a cl<strong>in</strong>ically useful diagnostic test.A panel approach for <strong>the</strong> <strong>diagnosis</strong> <strong>of</strong> <strong>ischaemic</strong> <strong>stroke</strong>To optimise diagnostic accuracy, <strong>the</strong> biochemical <strong>markers</strong> that best correlatedwith <strong>ischaemic</strong> <strong>stroke</strong> were entered <strong>in</strong>to a predictive multivariate model and athree-marker panel was developed that <strong>in</strong>cluded matrix metalloprote<strong>in</strong>ase-9(MMP-9), vascular cell adhesion molecule (VCAM), and vWF [4]. This panelwas able to dist<strong>in</strong>guish <strong>ischaemic</strong> <strong>stroke</strong> patients present<strong>in</strong>g with<strong>in</strong> 6 hours <strong>of</strong>symptom onset from controls with a sensitivity and specificity <strong>of</strong> over 90%[Figure 1]. Ano<strong>the</strong>r panel, which <strong>in</strong>cluded S100β ra<strong>the</strong>r than MMP-9, was ableto dist<strong>in</strong>guish <strong>stroke</strong> patients present<strong>in</strong>g between 6 and 24 hours after symptomonset from controls with a similar sensitivity and specificity. Abnormalities <strong>in</strong><strong>the</strong>se <strong>markers</strong> reflect glial activation and derangements <strong>in</strong> <strong>the</strong> coagulation systemand <strong>in</strong>flammatory processes - events that occur early <strong>in</strong> <strong>the</strong> <strong>ischaemic</strong> cascade.A po<strong>in</strong>t-<strong>of</strong>-care test that measures biochemical <strong>markers</strong> <strong>of</strong> cerebral ischaemiacould be cost- and time-sav<strong>in</strong>g <strong>in</strong> comparison with expensive neuroimag<strong>in</strong>gtechniques currently be<strong>in</strong>g <strong>in</strong>vestigated. In <strong>the</strong> community sett<strong>in</strong>g, where <strong>the</strong>seFigure 1. Received operat<strong>in</strong>g characteristics (ROC) curve demonstrat<strong>in</strong>g predictive capacity<strong>of</strong> biomarker panel: sensitivity vs 1-specificity [4].References1. Barber PA, Demchuk AM, Hirt L, et al. Biochemistry <strong>of</strong> ischemic <strong>stroke</strong>. Adv Neurol2003; 92: 151 - 164.2. Pantoni L, Sarti C and Inzitari D. Cytok<strong>in</strong>es and cell adhesion molecules <strong>in</strong> cerebralischaemia: experimental bases and <strong>the</strong>rapeutic perspectives. Arterioscler Throm VascBiol 1998; 18: 503 - 513.3. Price CJS, Warburton EA and Menon DK. Human cellular <strong>in</strong>flamation <strong>in</strong> <strong>the</strong> pathology<strong>of</strong> <strong>acute</strong> ischemia. J Neurol Neurosurg Psychiatry 2003; 74: 1476 - 1484.4. Lynch JR, Bless<strong>in</strong>g R, White WD, et al. Novel diagnostic test for <strong>acute</strong> <strong>stroke</strong>. Stroke2004; 35: 57 - 63.5. Reynolds MA, Kirchick HJ, Dahlen JR, Anderberg JM, McPherson PH, Nakamura KK,Laskowitz DT, Valkirs GE and Buechler KF. Early Bio<strong>markers</strong> <strong>of</strong> Stroke. Cl<strong>in</strong>icalChemistry 2003; 49: 1733 - 1739.For a full list <strong>of</strong> references contact <strong>the</strong> correspond<strong>in</strong>g author.The authorsJames S. Floyd, BSDuke University School <strong>of</strong> Medic<strong>in</strong>eDaniel T. Laskowitz, MD, MHSAssociate Pr<strong>of</strong>essorDepartments <strong>of</strong> Medic<strong>in</strong>e (Neurology) and Anes<strong>the</strong>siologyDuke University Medical CenterDurham, NC 27707U.S.A.Correspond<strong>in</strong>g authorDaniel T. Laskowitz. MD, MHSBox 2900, Duke University Medical CenterDurham, NC 27710, USA.Fax +1 919 684 6514Email: danl@neuro.duke.edu