Physician's Statement - Tata AIA Life Insurance
Physician's Statement - Tata AIA Life Insurance
Physician's Statement - Tata AIA Life Insurance

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
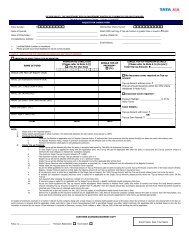
Policy No.:Claim No.:<strong>Tata</strong> <strong>AIA</strong> <strong>Life</strong> <strong>Insurance</strong> Company Limited(hereinafter called “<strong>Tata</strong> <strong>AIA</strong>”, whichever is applicable)TOTAL & PERMANENT DISABILITY CLAIM FORM (ATTENDING PHYSICIAN’S MEDICAL REPORT)To be completed in BLOCK letters by a duly qualified & registered medical practitioner at the claimant’s expense.Please answer all questions, use “not applicable” (N/A) as appropriate instead of leaving it blank. Counter-sign whereamendments/alterations are made in the form.Insured’s name Identity Card No. Age SexOccupation & duties of Insured declared to you(A) HISTORY & DIAGNOSISThe date when symptoms firstappeared or accident happened____ DD ____ MM _____YYYYSymptoms and complaintspresented by the InsuredThe date of first consultation____ DD ____ MM _____YYYYClinical and physicalfindings during firstconsultationThe date when the diagnosis wasgiven____ DD ____ MM _____YYYYThe diagnosis of thecondition and itscomplicationsThe date when the Insured firstabsent from work due to thecondition____ DD ____ MM _____YYYYHas patient ever hadsame or similar condition?If so, please state whenand give details.Details of consultations and treatment rendered by youDate/Period Details of Treatment Tests/Investigation/Surgical Procedures ResultName and address of other doctors/hospitals attended for treatment of this or similar conditionDate/Period Condition Physician/Hospital attended Address(B) CURRENT HEALTH OF THE INSUREDProgress of recoveryRecovered Improving Static RetrogressedRemarks :Current state of mobility.Give name of hospital and theperiod of hospitalconfinement, if anyRegistered and Corporate Office : <strong>Tata</strong> <strong>AIA</strong> <strong>Life</strong> <strong>Insurance</strong> Company Ltd. (IRDA Regn. No. 110),14th Floor, Tower A,Peninsula Business Park, Senapati Bapat Marg, Lower Parel, Mumbai 400013. CIN: U66010MH2000PLC128403.CLP/P4.9/4.T39 (I)Version 1Ambulatory Home confined Bed confined Hospital confinedRemarks :
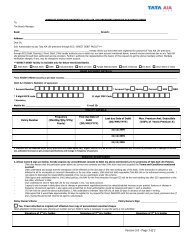
Please describe the currentphysical impairmentWith the current health condition ofthe Insured in mind, what wouldyou rate the present workingcapacity of the insured?Please describe the current mentalimpairment of the Insured (if normal,please go to Part D)With the current mental status of theInsured as described above, whatwould you rate the present ability forinterpersonal relations andcommunication of the insured?No limitation of functional capacity, capable of heavy work without restrictionsCapable of medium manual activitySlight limitation of functional capacity, capable of light workModerate limitation of functional capacity, capable of clerical / administrative activitySevere limitation of functional capacity, incapable of minimum activityRemarks :Able to engage in all interpersonal relations and communication (without limitations)Able to engage in most interpersonal relations and communication (slight limitations)Able to engage in only limited interpersonal relations and communication (moderate limitations)Unable to engage in interpersonal relations and communication (marked limitations)Has significant loss of psychological, physiological, personal and social adjustment (severe limitations)Remarks :(C) PROGNOSIS & REHABILITATIONIs the insured now totally disabled? In terms of his/her own job Yes No In terms of any other job Yes NoWhat duties of the Insured’s job ishe/she incapable of performing?Do you expect a fundamental ormarked change of this presentcondition in the future?YesNoIf yes, how long do you expect theInsured will take to perform duties?In terms of own jobWithin 1 Mth 1-3 Mths 3-6 Mths6-12 Mths > 12Mths NeverRemarks :In terms of any other jobWithin 1 Mth 1-3 Mths 3-6 Mths6-12 Mths >12Mths NeverRemarks :If no, please explainPlease state any furthertreatment/rehabilitation plan(D) MISCELLANEOUSIf there is any further information which in your opinion will assist us in assessing this claim, please furnish such information.Can our Medical Director and/or claim assessor release the information provided by youin this report to the patient when we are requested to explain our claim decision?I hereby declare that I have personally examined and treated the insured in connection to the above disability and that the facts asgiven above are true and complete to the best of my knowledge and belief.YesNoName of Physician _____________________________ Signature ______________________________________QualificationsRegistration No. &Place__________________________________________________________ Chop ______________________________________Address _____________________________ Telephone ________________________________________________________________________________________________Registered and Corporate Office : <strong>Tata</strong> <strong>AIA</strong> <strong>Life</strong> <strong>Insurance</strong> Company Ltd. (IRDA Regn. No. 110),14th Floor, Tower A,Peninsula Business Park, Senapati Bapat Marg, Lower Parel, Mumbai 400013. CIN: U66010MH2000PLC128403.Version 1