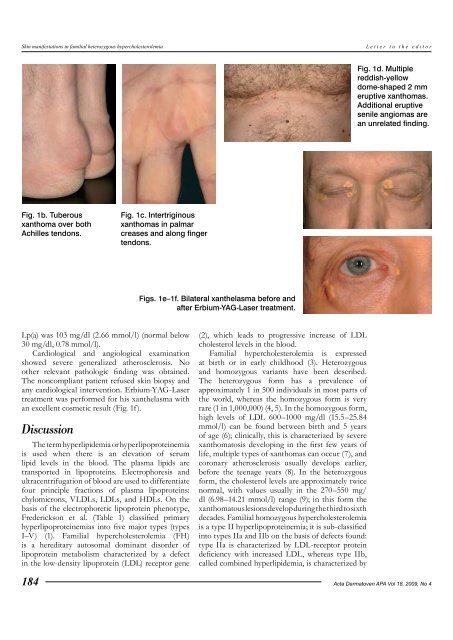
<strong>Sk<strong>in</strong></strong> <strong>manifestations</strong> <strong>in</strong> <strong>familial</strong> <strong>heterozygous</strong> <strong>hypercholesterolemia</strong>Letter to the editorFig. 1d. Multiplereddish-yellowdome-shaped 2 mmeruptive xanthomas.Additional eruptivesenile angiomas arean unrelated f<strong>in</strong>d<strong>in</strong>g.Fig. 1b. Tuberousxanthoma over bothAchilles tendons.Fig. 1c. Intertrig<strong>in</strong>ousxanthomas <strong>in</strong> palmarcreases and along f<strong>in</strong>gertendons.Figs. 1e–1f. Bilateral xanthelasma before andafter Erbium-YAG-Laser treatment.Lp(a) was 103 mg/dl (2.66 mmol/l) (normal below30 mg/dl, 0.78 mmol/l).Cardiological and angiological exam<strong>in</strong>ationshowed severe generalized atherosclerosis. Noother relevant pathologic f<strong>in</strong>d<strong>in</strong>g was obta<strong>in</strong>ed.The noncompliant patient refused sk<strong>in</strong> biopsy andany cardiological <strong>in</strong>tervention. Erbium-YAG-Lasertreatment was performed for his xanthelasma withan excellent cosmetic result (Fig. 1f).DiscussionThe term hyperlipidemia or hyperlipoprote<strong>in</strong>emiais used when there is an elevation of serumlipid levels <strong>in</strong> the blood. The plasma lipids aretransported <strong>in</strong> lipoprote<strong>in</strong>s. Electrophoresis andultracentrifugation of blood are used to differentiatefour pr<strong>in</strong>ciple fractions of plasma lipoprote<strong>in</strong>s:chylomicrons, VLDLs, LDLs, and HDLs. On thebasis of the electrophoretic lipoprote<strong>in</strong> phenotype,Frederickson et al. (Table 1) classified primaryhyperlipoprote<strong>in</strong>emias <strong>in</strong>to five major types (typesI–V) (1). Familial <strong>hypercholesterolemia</strong> (FH)is a hereditary autosomal dom<strong>in</strong>ant disorder oflipoprote<strong>in</strong> metabolism characterized by a defect<strong>in</strong> the low-density lipoprote<strong>in</strong> (LDL) receptor gene184(2), which leads to progressive <strong>in</strong>crease of LDLcholesterol levels <strong>in</strong> the blood.Familial <strong>hypercholesterolemia</strong> is expressedat birth or <strong>in</strong> early childhood (3). Heterozygousand homozygous variants have been described.The <strong>heterozygous</strong> form has a prevalence ofapproximately 1 <strong>in</strong> 500 <strong>in</strong>dividuals <strong>in</strong> most parts ofthe world, whereas the homozygous form is veryrare (1 <strong>in</strong> 1,000,000) (4, 5). In the homozygous form,high levels of LDL 600–1000 mg/dl (15.5–25.84mmol/l) can be found between birth and 5 yearsof age (6); cl<strong>in</strong>ically, this is characterized by severexanthomatosis develop<strong>in</strong>g <strong>in</strong> the first few years oflife, multiple types of xanthomas can occur (7), andcoronary atherosclerosis usually develops earlier,before the teenage years (8). In the <strong>heterozygous</strong>form, the cholesterol levels are approximately twicenormal, with values usually <strong>in</strong> the 270–550 mg/dl (6.98–14.21 mmol/l) range (9); <strong>in</strong> this form thexanthomatous lesions develop dur<strong>in</strong>g the third to sixthdecades. Familial homozygous <strong>hypercholesterolemia</strong>is a type II hyperlipoprote<strong>in</strong>emia; it is sub-classified<strong>in</strong>to types IIa and IIb on the basis of defects found:type IIa is characterized by LDL-receptor prote<strong>in</strong>deficiency with <strong>in</strong>creased LDL, whereas type IIb,called comb<strong>in</strong>ed hyperlipidemia, is characterized byActa Dermatoven APA Vol 18, 2009, No 4
Letter to the editor<strong>Sk<strong>in</strong></strong> <strong>manifestations</strong> <strong>in</strong> <strong>familial</strong> <strong>heterozygous</strong> <strong>hypercholesterolemia</strong>Fig. 1g. Arcus senilis between 4 and 12 o’clock.decreased LDL-receptor and <strong>in</strong>creased ApoB withadditional tendency for elevated LDL and VLDLIn our patient, the lipid profile was suggestive of<strong>heterozygous</strong> type IIa hyperlipoprote<strong>in</strong>emia, withmarkedly elevated LDL cholesterol levels andnormal VLDL and triglyceride levels. Intertrig<strong>in</strong>ous,tend<strong>in</strong>ous, tuberous xanthomas and xanthelasmapalpebrarum are typical <strong>manifestations</strong>.Xanthoma (from Greek ξανθός ‘yellow’) is adeposition of yellowish material formed by lipids<strong>in</strong> foam cells (10) (macrophages with phagocytosedlipid material) and collagen. There are differentxanthomas based on their cl<strong>in</strong>ical and morphologicalaspects.Various experiments have been conducted todef<strong>in</strong>e the mechanism of lipid deposition <strong>in</strong> tendonxanthomas. LDL derived from plasma is trapped <strong>in</strong>the collagen and glycosam<strong>in</strong>oglycans of the tendonmatrix and can be oxidized at these sites. Thereaction of LDL with macrophages or other cells ofthe tendon can expla<strong>in</strong> the modification of LDL <strong>in</strong>tooxLDL, which is taken up ma<strong>in</strong>ly by macrophages,thereby promot<strong>in</strong>g the formation of foam cells (11,12), which extravasate through the vascular wallsand deposit <strong>in</strong> perivascular connective tissue.Tendon xanthomas are firm subcutaneousnodules, which may be hard due to fibrosis. Theyare usually sk<strong>in</strong> colored and do not appear yellowbecause the cholesterol ester is deposited deep with<strong>in</strong>the tendons. They are localized over the proximalf<strong>in</strong>ger jo<strong>in</strong>ts, the <strong>in</strong>sertions of the patellar tendons,and the Achilles tendons (13). This disfigur<strong>in</strong>gpathological state may <strong>in</strong>terfere with function andcause achillodynia and, rarely, spontaneous tendonrupture (14). Tendonitis, peritend<strong>in</strong>itis or bursitis,trauma, nodules from rheumatic arthritis, or gouttophi are other frequent conditions that may lead toAchilles tendon (AT) thicken<strong>in</strong>g, and <strong>in</strong> such casesdifferential diagnosis from ATX (Achille tendonFig. 2. The hypoechoic area between the arrowscorresponds to tuberous xanthoma.xanthoma) may be difficult. Detailed family andmedical history, serum lipid analysis, and ultrasoundof the affected tendon may help <strong>in</strong> the differentialdiagnosis (15, 16). Ultrasound is the most importantimag<strong>in</strong>g method used for evaluat<strong>in</strong>g ATX (16–18).The sonographic aspect, with 7.5 MHz l<strong>in</strong>ear arraytransducer, of our patient’s Achilles tendon wascharacterized by a focal hypoechoic lesion (Fig.2). The deposition of cholesterol <strong>in</strong> xanthomas issimilar to that <strong>in</strong> atherosclerotic lesions (19). Cl<strong>in</strong>icaland imag<strong>in</strong>g studies have suggested that a positivecorrelation exists between tendon xanthomaregression and improvement <strong>in</strong> atheroscleroticdisease (20), which is the ma<strong>in</strong> cause of death <strong>in</strong>dyslipidemic patients.Xanthelasma palpebrarum is the mostimportant cl<strong>in</strong>ical manifestation visible around theeyes. Accord<strong>in</strong>g to many epidemiologic studies,xanthelasma is thought to be a determ<strong>in</strong>ant of an<strong>in</strong>creased risk of atherosclerosis (21).Very rare are <strong>in</strong>tertrig<strong>in</strong>ous xanthomas, consist<strong>in</strong>gof a yellow dermal plaque with corrugated surfacelocalized <strong>in</strong> the f<strong>in</strong>ger webs, palmar creases, axillae,buttocks, and antecubital and popliteal fossae (22,23). Other type of xanthomas are the eruptive formlocalized <strong>in</strong> the gluteal region, trunk, and extensorsurface of the extremities; these lesions are small, lightyellow, and usually surrounded by an <strong>in</strong>flammatoryhalo. An important sign is the corneal arcus orarcus senilis, which appears as a s<strong>in</strong>gle grayish r<strong>in</strong>gparallel to the limbus and is separated from it by a1 mm lucid <strong>in</strong>terval of Vogt. It is typically localizedbetween 6 and 12 o’clock. It develops as a result oflipid deposition <strong>in</strong> the deep corneal stroma and thelimbal sclera, and its prevalence <strong>in</strong>creases with age.Various techniques and methods have been described<strong>in</strong> the literature to treat this condition, <strong>in</strong>clud<strong>in</strong>gapplication of trichloroacetic acid (TCA), electriccautery, surgical excision, carbon dioxide laserActa Dermatoven APA Vol 18, 2009, No 4 185