Primary Benign Cystic Retroperitoneal Teratoma in an ...
Primary Benign Cystic Retroperitoneal Teratoma in an ...
Primary Benign Cystic Retroperitoneal Teratoma in an ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
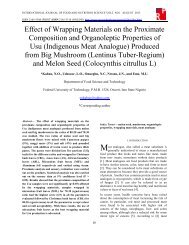
BIOCHEMICAL AND BIOPHYSICAL JOURNAL OF NEUTRON THERAPY & CANCER TREATMENTSVOL1.NO.1 JUNE 2013 http://www.researchpub.org/journal/bbjntct/bbjntct.htmlVOL.1<strong>Primary</strong> <strong>Benign</strong> <strong>Cystic</strong> <strong>Retroperitoneal</strong> <strong>Teratoma</strong><strong>in</strong> <strong>an</strong> Asymptomatic AdultRahul Gupta, MBBS, Yella Reddy, MS, Rohit Gupta, MBBS, James S. Welsh, MD,Alice Mad<strong>an</strong>i, B.A., Naray<strong>an</strong> S. Hosm<strong>an</strong>e, Ph.DAbstract— <strong>Primary</strong> retroperitoneal teratoma is a rare entity <strong>in</strong>adults with a dist<strong>in</strong>ctive imag<strong>in</strong>g appear<strong>an</strong>ce. We describe <strong>an</strong>unusual case of a 19-year old male patient referred to our hospitaldue to a large mass <strong>in</strong> his abdomen. Radiological work-uprevealed a large retroperitoneal mass with no other masses orabnormalities. Exploratory laparotomy with tumor resection wasperformed. Histopathological diagnosis confirmed a benign cysticteratoma. The patient is do<strong>in</strong>g well on follow up 5 years laterepigastric <strong>an</strong>d left hypochondrium mov<strong>in</strong>g with respiration <strong>an</strong>ddull to percussion. A cl<strong>in</strong>ical diagnosis of pseudop<strong>an</strong>creaticcyst was made <strong>an</strong>d patient was sent for various <strong>in</strong>vestigations.Rout<strong>in</strong>e blood tests <strong>an</strong>d ur<strong>in</strong>alysis were all with<strong>in</strong> normal limits.However, ultrasound demonstrated a large, complex, denselymixed echogenic mass, suggestive of a fatty nature to the masswith sheet like calcifications (Image 1) <strong>an</strong>d no ascites.Contrast computed tomography (CT) of the abdomen revealedIndex Terms— Laparotomy, Retroperitoneum, <strong>Teratoma</strong>I. INTRODUCTION<strong>Teratoma</strong>s are uncommon neoplasms that conta<strong>in</strong> derivativesof all three germ layers (ectoderm, mesoderm <strong>an</strong>d endoderm).Historically, teratomas were attributed to demons, sexualmisconduct <strong>an</strong>d abnormal fertilization. As with teratogenic, thename derives from the Greek word teras, me<strong>an</strong><strong>in</strong>g ‘monster’.<strong>Teratoma</strong>s belong to a class of tumors known asnon-sem<strong>in</strong>omatous germ cell tumor <strong>an</strong>d are typically located <strong>in</strong>gonadal region. However, extragonadal sites such as thesacrococcygeal region, mediast<strong>in</strong>um, neck, di<strong>an</strong>cephalon <strong>an</strong>dretroperitoneum have also been reported. <strong>Retroperitoneal</strong>teratomas often occur <strong>in</strong> <strong>in</strong>f<strong>an</strong>cy <strong>an</strong>d childhood but are rare <strong>in</strong>adults. In this article, we describe <strong>an</strong> unusual case of aretroperitoneal teratoma <strong>in</strong> a 19-year old asymptomatic malepatient who subsequently, underwent successful surgicalresection.II. CASE REPORTA 19-year old male presented with upper abdom<strong>in</strong>al distensionfor 3 months. He had no weight loss, bowel or ur<strong>in</strong>arycompla<strong>in</strong>ts. On exam<strong>in</strong>ation, a large mass was palpable <strong>in</strong> theSubmitted on 06/05/2013. Revised on 07/24/2013.Rahul Gupta is with Northern Ill<strong>in</strong>ois University, DeKalb, IL 60115U.S.A. (email: grahul.md@gmail.com)Yella Reddy is with Vyedhi Institute of Medical Sciences <strong>an</strong>d ResearchCentre, B<strong>an</strong>galore, 560 066 India (email: <strong>in</strong>fo@vims.ac.<strong>in</strong>)Rohit Gupta is with St. Georges University, Grenada, West Indies (email:dr.guptarohit@gmail.com)James S. Welsh is with Northern Ill<strong>in</strong>ois University <strong>an</strong>d Fermi NationalAccelerator Laboratory, Batavia, IL 60510 U.S.A. (email:sherm<strong>an</strong>welsh@gmail.com)Alice Mad<strong>an</strong>i is with Tr<strong>in</strong>ity School of Medic<strong>in</strong>e, St. V<strong>in</strong>cent <strong>an</strong>d theGrenad<strong>in</strong>es (email: alicemad<strong>an</strong>i@gmail.com)Naray<strong>an</strong> S. Hosm<strong>an</strong>e is with Northern Ill<strong>in</strong>ois University, DeKalb, IL 60115U.S.A. (email: hosm<strong>an</strong>e@niu.edu)5Image 1. Ultrasound of abdomen show<strong>in</strong>g retroperitoneal space occupy<strong>in</strong>glesiona large retroperitoneal mass <strong>an</strong>terior to the head of p<strong>an</strong>creas,<strong>in</strong>itially suspicious for a retroperitoneal sarcoma. However, thepresence of fat <strong>an</strong>d bone <strong>in</strong>side the mass was highly <strong>in</strong>dicativeof a benign cystic teratoma. CT-guided f<strong>in</strong>e needle aspirationcytology (FNAC) of the mass was consistent with the diagnosisof teratoma. Chest X-ray prior to surgery, revealed no lungmetastases or lymphadenopathy.Exploratory laparotomy revealed a large cystic retroperitonealmass (Image 2) situated <strong>an</strong>terior to the p<strong>an</strong>creas <strong>an</strong>d posterior tothe stomach. The tumor extended from the left hemidiaphragmdown to the umbilicus beyond the midl<strong>in</strong>e. Macroscopically,the encapsulated mass measured 14.86 cms x 11.03 cms (Image3). Microscopically, it appeared to be a cystic tumor withextensive necrosis <strong>an</strong>d amorphous debris. There were fewmature squamous cells along with few <strong>an</strong>ucleate squamouscells. Background showed <strong>an</strong> <strong>in</strong>filtrate of polymorphs,lymphocytes <strong>an</strong>d plasma cells. With<strong>in</strong> the mass itself, sk<strong>in</strong>
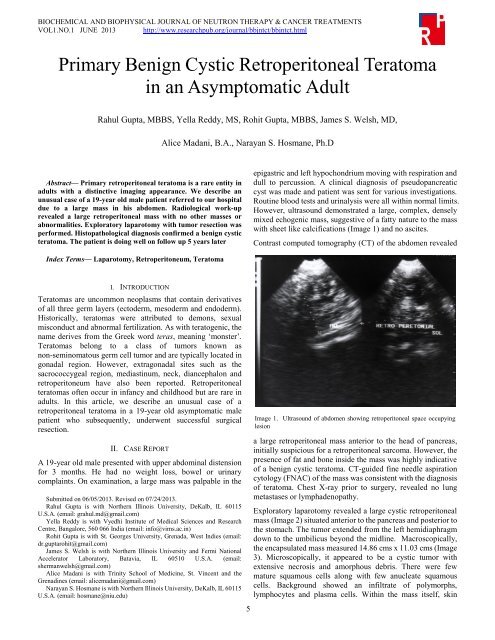
BIOCHEMICAL AND BIOPHYSICAL JOURNAL OF NEUTRON THERAPY & CANCER TREATMENTSVOL1.NO.1 JUNE 2013 http://www.researchpub.org/journal/bbjntct/bbjntct.htmlVOL.1Image 2. Exploratory laparotomy reveal<strong>in</strong>g the large cystic massadnexa, bone, fat <strong>an</strong>d nerve were seen, consistent with atril<strong>in</strong>eage teratoma. Histopathology confirmed the diagnosis ofa primary cystic teratoma, benign <strong>in</strong> nature, with no malign<strong>an</strong>tcells present. Postoperative course has been uneventful.III. DISCUSSIONImage 3. Contract CT of the abdomen shows a large retroperitoneal mass<strong>an</strong>terior to the head of p<strong>an</strong>creasOverall, primary retroperitoneal teratomas constitute about1-11% [1-3] of all primary retroperitoneal tumors.Approximately half of all teratomas found <strong>in</strong> children arediscovered <strong>in</strong> first decade of life with 43-45% of retroperitonealteratomas diagnosed with<strong>in</strong> the first year of life. Less th<strong>an</strong>10-20% of retroperitoneal teratomas present <strong>in</strong> patients after 30years of age [4].<strong>Teratoma</strong>s arise from germ cells that fail to mature normally <strong>in</strong>the gonadal locations. These totipotent cells c<strong>an</strong> differentiate<strong>in</strong>to tissue components represent<strong>in</strong>g derivatives of mesoderm,ectoderm <strong>an</strong>d endoderm. The distribution of teratomas listed <strong>in</strong>6order of decreas<strong>in</strong>g frequency is: ovaries, testes, <strong>an</strong>teriormediast<strong>in</strong>um, retroperitoneal space, pre sacral <strong>an</strong>d coccygealareas, p<strong>in</strong>eal <strong>an</strong>d other <strong>in</strong>tracr<strong>an</strong>ial sites, neck <strong>an</strong>d abdom<strong>in</strong>alviscera other th<strong>an</strong> gonads. The developmental migratoryproperties of germ cells would expla<strong>in</strong> teratomas <strong>in</strong> theseextragonadal sites, which generally occur along midl<strong>in</strong>estructures [1, 5].<strong>Retroperitoneal</strong> teratomas are usually asymptomatic exceptwhen compression of the surround<strong>in</strong>g structures occurs.Patients with compressive symptoms may present with backpa<strong>in</strong>, genitour<strong>in</strong>ary symptoms, gastro<strong>in</strong>test<strong>in</strong>al symptoms(abdom<strong>in</strong>al distension, pa<strong>in</strong>, nausea <strong>an</strong>d vomit<strong>in</strong>g), as well aslower extremity or genital edema secondary to lymphaticobstruction [1, 6].The differential diagnosis of retroperitoneal teratomas <strong>in</strong>cludeovari<strong>an</strong> tumors, renal cysts, adrenal tumors, retroperitonealfibromas, retroperitoneal sarcomas (usually liposarcomas),hem<strong>an</strong>giomas, x<strong>an</strong>thogr<strong>an</strong>ulomas, enlarged lymph nodes <strong>an</strong>dperirenal abscesses [7, 8]. Testicular ultrasound is necessary torule out testicular germ cell tumor <strong>in</strong> male patients. This is <strong>an</strong>ecessary step s<strong>in</strong>ce 50% of men with retroperitoneal tumorsalso have testicular carc<strong>in</strong>oma <strong>in</strong> situ, a precursor for testiculargerm cell tumors [9].Between 1932 <strong>an</strong>d 1987, 32 adult cases were reported out ofwhich 15 occurred <strong>in</strong> female patients <strong>an</strong>d 17 occurred <strong>in</strong> males.<strong>Retroperitoneal</strong> teratomas <strong>in</strong> these patients were most oftenlocated near the upper pole of the kidney, mostly on the left side[5, 6]. -Malign<strong>an</strong>t degeneration was higher <strong>in</strong> adults th<strong>an</strong> <strong>in</strong> children,with <strong>in</strong>cidences of 25.8% <strong>an</strong>d 6.8%, respectively. Malign<strong>an</strong>tteratomas may cause rise <strong>in</strong> serum alpha-fetoprote<strong>in</strong> (AFP) [6].Calcifications c<strong>an</strong> be demonstrated <strong>in</strong> 61.5% of teratoma caseson a pla<strong>in</strong> <strong>an</strong>teroposterior <strong>an</strong>d lateral abdom<strong>in</strong>al films <strong>an</strong>d areuseful for the pre-operative diagnosis [1]. Such calcificationsmay be with<strong>in</strong> the tumor or on the rim of the cyst wall. Eventhough 74% of benign teratomas conta<strong>in</strong> calcification, they alsooccur <strong>in</strong> 12.5% of malign<strong>an</strong>t teratomas [10].Several imag<strong>in</strong>g modalities elucidate different characteristicsof a teratoma. For example, ultrasound c<strong>an</strong> identify the cystic,solid or complex components of the tumor [11]. The cysticportion may be further differentiated <strong>in</strong>to sebum, non-fat fluid<strong>an</strong>d structures resembl<strong>in</strong>g fetal parts. However, ultrasound hasits limitations as Davidson et al found that ultrasound poorlyidentified fat <strong>an</strong>d calcifications, which are suggestive ofteratoma.CT has several adv<strong>an</strong>tages over ultrasound. First, it gives morespecific <strong>in</strong>formation on the fat, prote<strong>in</strong>aceous fluid <strong>an</strong>dcalcification components of the teratoma through Hounsfieldunits, which allows qu<strong>an</strong>titative comparison of subst<strong>an</strong>ces ofdifferent radiodensities. The presence of fatty portions of thetumor <strong>in</strong> the horizontal <strong>in</strong>terface with dependent fluid, whichprobably represents sebum, is virtually pathognomonic of ateratoma [11, 12]. However, a fat fluid level has also beendescribed <strong>in</strong> case of a well differentiated liposarcoma of theretroperitoneum [13]. Second, CT appears superior to
BIOCHEMICAL AND BIOPHYSICAL JOURNAL OF NEUTRON THERAPY & CANCER TREATMENTSVOL1.NO.1 JUNE 2013 http://www.researchpub.org/journal/bbjntct/bbjntct.htmlVOL.1ultrasound at def<strong>in</strong><strong>in</strong>g extent <strong>in</strong> to surround<strong>in</strong>g org<strong>an</strong>s <strong>an</strong>d forevaluat<strong>in</strong>g the cyst wall [11].Magnetic reson<strong>an</strong>ce imag<strong>in</strong>g (MRI) <strong>an</strong>d <strong>an</strong>giography offerother benefits. MRI is superior to both ultrasound <strong>an</strong>d CT <strong>in</strong>def<strong>in</strong><strong>in</strong>g the <strong>an</strong>atomical relationship of the teratoma withadjacent org<strong>an</strong>s <strong>an</strong>d local tumor spread [14, 15]. MRI c<strong>an</strong> alsodist<strong>in</strong>guish fluid, fat, calcium <strong>an</strong>d soft tissue elements, as wellas predict resectability <strong>an</strong>d evaluate recurrence [16].Angiography is beneficial for detect<strong>in</strong>g the presence ofhypervascularity, arterial encasement <strong>an</strong>d org<strong>an</strong> <strong>in</strong>vasion,features often suggest<strong>in</strong>g malign<strong>an</strong>cy [17].In our case, the <strong>in</strong>itial differential diagnosis <strong>in</strong>cludedretroperitoneal sarcoma. Even with modern preoperativeimag<strong>in</strong>g studies, retroperitoneal sarcomas c<strong>an</strong> be confused withretroperitoneal teratomas [18]. Pre- or post-operative radiationtherapy c<strong>an</strong> be challeng<strong>in</strong>g <strong>in</strong> retroperitoneal sarcomas becauseof radiosensitive adjacent normal structures <strong>an</strong>d the need forrelatively high doses, especially <strong>in</strong> unresectable cases or whenpositive marg<strong>in</strong>s are left beh<strong>in</strong>d. In such situations, fast neutrontherapy [19] or more recently, <strong>in</strong>tensity-modulatedradiotherapy, <strong>in</strong>traoperative electron beam radiotherapy orproton therapy has been considered [20]. While retroperitonealsarcomas are often treated with a comb<strong>in</strong>ation of preoperativeradiation therapy <strong>an</strong>d surgery [21, 22], retroperitonealteratomas, if benign, usually do not warr<strong>an</strong>t radiotherapy.IV. CONCLUSIONIn summary, teratomas c<strong>an</strong> macroscopically be divided <strong>in</strong>to 2categories: cystic or solid. <strong>Cystic</strong> teratomas are mostly benign,conta<strong>in</strong><strong>in</strong>g sebaceous materials <strong>an</strong>d mature tissue types. On theother h<strong>an</strong>d, solid teratomas are often malign<strong>an</strong>t <strong>an</strong>d composedof immature embryonic tissues <strong>in</strong> addition to adipose,cartilag<strong>in</strong>ous, fibrous <strong>an</strong>d bony components. The prognosis isexcellent for benign retroperitoneal teratoma if completeresection c<strong>an</strong> be accomplished.ACKNOWLEDGMENTDr. Rahul Gupta would like to th<strong>an</strong>k Rik<strong>in</strong> Shah, MD student,for giv<strong>in</strong>g his valuable time <strong>in</strong> help<strong>in</strong>g proofread <strong>an</strong>d evaluatethis article. We gratefully acknowledge KishwaukeeCommunity Hospital Foundation for the support of this work.[5] Engel RM, Elk<strong>in</strong>s RC, Fletcher BD. <strong>Retroperitoneal</strong> teratoma. Review ofthe literature <strong>an</strong>d presentation of <strong>an</strong> unusual case. C<strong>an</strong>cer 1968; 22:1068-1073.[6] Lambri<strong>an</strong>ides AL, Walker MM, Ros<strong>in</strong> RD. <strong>Primary</strong> retroperitonealteratoma <strong>in</strong> adults. Urology 1987; 29: 310-312.[7] P<strong>an</strong>toja E, Llobet R, Gonzalez-Flores B. <strong>Retroperitoneal</strong> teratoma: ahistorical review. J Urol 1976; 115: 520-523.[8] P<strong>an</strong>dya JS, Pai MV, Munchhala S. <strong>Retroperitoneal</strong> teratoma present<strong>in</strong>g asacute abdomen <strong>in</strong> <strong>an</strong> elderly person. Ind Jou Gastroentero 2000; 19;89-90.[9] T. Gillig<strong>an</strong>, P.K<strong>an</strong>toff. Extragonadal germ cell tumors <strong>in</strong>volv<strong>in</strong>g themediast<strong>in</strong>um <strong>an</strong>d retroperitoneum. UpToDate Patient Preview, W.K. Oh,Ed., UpToDate, Waltham, Mass, USA, 2009.[10] Bruneton JN, Diard F, Drouillard JP, et al. <strong>Primary</strong> retroperitonealteratoma <strong>in</strong> adults: Presentation of two cases <strong>an</strong>d review of the literature.Radiology 1980; 134; 613-616.[11] Davidson AJ, Hartm<strong>an</strong> DS, Goldm<strong>an</strong> SM, Mature teratoma of theretroperitoneum: radiologic, pathologic, <strong>an</strong>d cl<strong>in</strong>ical correlation.Radiology 1989; 172: 421-425.[12] Billmire DF, Grosfeld JL. <strong>Teratoma</strong>s <strong>in</strong> childhood: <strong>an</strong>alysis of 142 cases.J Pediatric Surg 1986; 21: 548-551.[13] Smirniotopoulos JG, Chiechi MV. <strong>Teratoma</strong>s, dermoids, <strong>an</strong>d epidermoidsof the head <strong>an</strong>d neck. Radiographics 1995; 15: 1437-1455.[14] Bell<strong>in</strong> MF, Duron JJ, Curet PH, Dion-Voir<strong>in</strong> E, Grellet J. <strong>Primary</strong>retroperitoneal teratoma <strong>in</strong> the adult: correlation of the MRI features withCT <strong>an</strong>d pathology. Magn Reson Imag<strong>in</strong>g 1991; 9: 263-266.[15] Choi BI, Chi JG, kim SH, Ch<strong>an</strong>g KH, H<strong>an</strong> MC. MR imag<strong>in</strong>g ofretroperitoneal teratoma: correlation with CT <strong>an</strong>d pathology. J ComputAssist Tomogr 1989; 13: 1083-1086.[16] Cohen MC, Weetm<strong>an</strong> RM, Provisor AJ. Efficacy of magnetic reson<strong>an</strong>ceimag<strong>in</strong>g <strong>in</strong> 139 children with tumors. Arch Surg 1986; 121: 522-529.[17] Renato F, Paolo V, Girolamo M, Vig<strong>an</strong>o L, Aless<strong>an</strong>dro P, Claudio V, et al.Malign<strong>an</strong>t retroperitoneal teratoma: case report <strong>an</strong>d literature review.Acta Urol Belg 1996; 64: 49-54.[18] Ki EY, Park ST, Park JS, Hur SY. A huge retroperitoneal liposarcoma:case report. Euro J Gynaecol Oncol 2012; 33(3): 318-320.[19] Schwartz DL, E<strong>in</strong>ck J, Bellon J, Laramore GE. Fast neutron radiotherapyfor soft tissue <strong>an</strong>d cartilag<strong>in</strong>ous sarcomas at high risk for local recurrence.Int J Radiat Oncol Biol Phys. 2001 Jun 1; 50(2):449-456.[20] Yoon SS, Chen YL, Kirsch DG, Maduekwe UN, Rosenberg AE, NielsenGP, Sah<strong>an</strong>i DV, Choy E, Harmon DC, DeL<strong>an</strong>ey TF. Proton-beam,<strong>in</strong>tensity-modulated, <strong>an</strong>d/or <strong>in</strong>traoperative electron radiation therapycomb<strong>in</strong>ed with aggressive <strong>an</strong>terior surgical resection forretroperitoneal sarcomas. Ann Surg Oncol. 2010; 17(6): 1515-1529.[21] Zlotecki RA, Katz TS, Morris CG, L<strong>in</strong>d DS, Hochwald SN. Adjuv<strong>an</strong>tradiation therapy for resectable retroperitoneal soft tissue sarcoma: theUniversity of Florida experience. Am J Cl<strong>in</strong> Oncol. 2005 Jun; 28(3):306-310.[22] Alford S, Choong P, Ch<strong>an</strong>der S, Henderson M, Powell G, Ng<strong>an</strong> S.Outcomes of preoperative radiotherapy <strong>an</strong>d resection of retroperitonealsarcoma. ANZ J Surg. 2013; 83(5): 334-336.REFERENCES[1] Gschwend J, Burke TW, Woodward JE, et al. <strong>Retroperitoneal</strong> teratomapresent<strong>in</strong>g as <strong>an</strong> abdom<strong>in</strong>al-pelvic mass. Obstet Gynecol 1987; 70:500-502.[2] L<strong>an</strong>e RH, Stephens DH, Reim<strong>an</strong> HM. <strong>Primary</strong> retroperitoneal neoplasms:CT f<strong>in</strong>d<strong>in</strong>gs <strong>in</strong> 90 cases with cl<strong>in</strong>ical <strong>an</strong>d pathologic correlation. AmerJour Roentgenology 1989; 152: 83-89.[3] W<strong>an</strong>g RM, Chen CA. <strong>Primary</strong> retroperitoneal teratoma. Acta ObstetGynecol Sc<strong>an</strong>d 2000; 79: 707-708.[4] P<strong>an</strong>ageas E. General diagnosis case of the day. <strong>Primary</strong> retroperitonealteratoma. AJR Am J Roentology 1991; 156; 1292-1294..7