S884 Circulation November 2, <strong>2010</strong>adult patients with VF refractory to shocks and epinephrine.228 Neither lidocaine nor amiodarone has been shown toimprove survival to hospital discharge.PrecautionsLidocaine toxicity includes myocardial and circulatory depression,drowsiness, disorientation, muscle twitching, andseizures, especially in patients with poor cardiac output andhepatic or renal failure. 229,230MagnesiumMagnesium is indicated for the treatment of documentedhypomagnesemia or for torsades de pointes (polymorphic VTassociated with long QT interval). There is insufficientevidence to recommend for or against the routine administrationof magnesium during cardiac arrest. 231–233PrecautionsMagnesium produces vasodilation and may cause hypotensionif administered rapidly.ProcainamideProcainamide prolongs the refractory period of the atria andventricles and depresses conduction velocity.PrecautionsThere is limited clinical data on using procainamide in infantsand children. 234–236 Infuse procainamide very slowly (over 30to 60 minutes) while monitoring the ECG and blood pressure.Decrease the infusion rate if there is prolongation of the QTinterval, or heart block; stop the infusion if the QRS widensto 50% of baseline or hypotension develops. Do notadminister together with another drug causing QT prolongation,such as amiodarone, without expert consultation. Priorto using procainamide for a hemodynamically stable patient,expert consultation is strongly recommended.Sodium BicarbonateRoutine administration of sodium bicarbonate is not recommendedin cardiac arrest (Class III, LOE B). 212,237,238 Sodiumbicarbonate may be administered for treatment of sometoxidromes (see “Toxicological Emergencies,” below) orspecial resuscitation situations such as hyperkalemic cardiacarrest.PrecautionsDuring cardiac arrest or severe shock, arterial blood gasanalysis may not accurately reflect tissue and venous acidosis.239,240 Excessive sodium bicarbonate may impair tissueoxygen delivery; 241 cause hypokalemia, hypocalcemia, hypernatremia,and hyperosmolality; 242,243 decrease the VFthreshold; 244 and impair cardiac function.VasopressinThere is insufficient evidence to make a recommendation foror against the routine use of vasopressin during cardiac arrest.Pediatric 245–247 and adult 248,249 case series/reports suggestedthat vasopressin 245 or its long-acting analog, terlipressin,246,247 may be effective in refractory cardiac arrest whenstandard therapy fails. A large <strong>pediatric</strong> NRCPR case series,however, suggested that vasopressin is associated with lowerROSC, and a trend toward lower 24-hour and dischargesurvival. 250 A preponderance of controlled trials in adults donot demonstrate a benefit. 251–256Pulseless ArrestIn the text below, box numbers identify the correspondingstep in the algorithm (Figure 1).● (Step 1) As soon as the child is found to be unresponsivewith no breathing, call for help, send for a defibrillator(manual or AED), and start CPR (with supplementaryoxygen if available). Attach ECG monitor or AED pads assoon as available. Throughout resuscitation, emphasisshould be placed on provision of high-quality CPR (providingchest compressions of adequate rate and depth,allowing complete chest recoil after each compression,minimizing interruptions in compressions and avoidingexcessive ventilation).● While CPR is being given, determine the child’s cardiacrhythm from the ECG or, if you are using an AED, thedevice will tell you whether the rhythm is “shockable” (eg,VF or rapid VT) or “not shockable” (eg, asystole or PEA).It may be necessary to temporarily interrupt chest compressionsto determine the child’s rhythm. Asystole and bradycardiawith a wide QRS are most common in asphyxialarrest. 1 VF and PEA are less common 13 but VF is morelikely to be present in older children with sudden witnessedarrest.“Nonshockable Rhythm”: Asystole/PEA (Step 9)PEA is an organized electric activity—most commonly slow,wide QRS complexes—without palpable pulses. Less frequentlythere is a sudden impairment of cardiac output withan initially normal rhythm but without pulses and with poorperfusion. This subcategory, formerly known as electromechanicaldissociation (EMD), may be more reversible thanasystole. For asystole and PEA:● (Step 10) Continue CPR with as few interruptions in chestcompressions as possible. A second rescuer obtains vascularaccess and delivers epinephrine, 0.01 mg/kg (0.1 mL/kgof 1:10 000 solution) maximum of 1 mg (10 mL), whileCPR is continued. The same epinephrine dose is repeatedevery 3 to 5 minutes (Class I, LOE B). There is no survivalbenefit from high-dose epinephrine, and it may be harmful,particularly in asphyxia (Class III, LOE B). 257–261 Highdoseepinephrine may be considered in exceptional circumstances,such as -blocker overdose (Class IIb, LOE C).● Once an advanced airway is in place, 1 rescuer should givecontinuous chest compressions at a rate of at least 100 perminute without pause for ventilation. The second rescuerdelivers ventilations at a rate of 1 breath every 6 to 8seconds (about 8 to 10 breaths per minute). Rotate thecompressor role approximately every 2 minutes to preventcompressor fatigue and deterioration in quality and rate ofchest compressions. Check rhythm every 2 minutes withminimal interruptions in chest compressions. If the rhythmis “nonshockable” continue with cycles of CPR and epinephrineadministration until there is evidence of ROSC oryou decide to terminate the effort. If at any time the rhythmDownloaded from circ.ahajournals.org by on October 20, <strong>2010</strong>
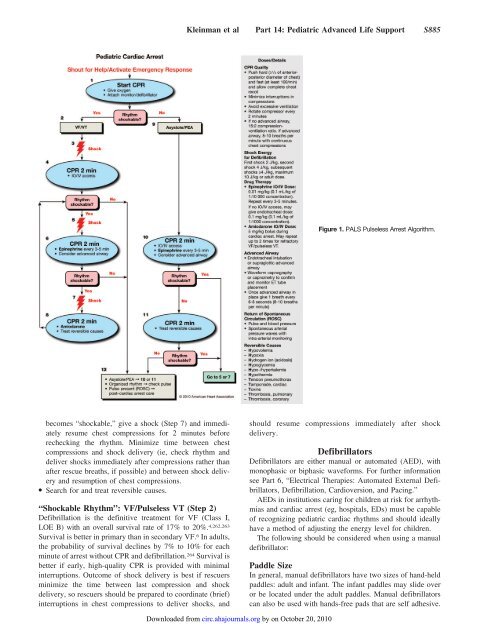
Kleinman et al Part 14: Pediatric Advanced Life Support S885Figure 1. P<strong>ALS</strong> Pulseless Arrest Algorithm.becomes “shockable,” give a shock (Step 7) and immediatelyresume chest compressions for 2 minutes beforerechecking the rhythm. Minimize time between chestcompressions and shock delivery (ie, check rhythm anddeliver shocks immediately after compressions rather thanafter rescue breaths, if possible) and between shock deliveryand resumption of chest compressions.● Search for and treat reversible causes.“Shockable Rhythm”: VF/Pulseless VT (Step 2)Defibrillation is the definitive treatment for VF (Class I,LOE B) with an overall survival rate of 17% to 20%. 4,262,263Survival is better in primary than in secondary VF. 6 In adults,the probability of survival declines by 7% to 10% for eachminute of arrest without CPR and defibrillation. 264 Survival isbetter if early, high-quality CPR is provided with minimalinterruptions. Outcome of shock delivery is best if rescuersminimize the time between last compression and shockdelivery, so rescuers should be prepared to coordinate (brief)interruptions in chest compressions to deliver shocks, andshould resume compressions immediately after shockdelivery.DefibrillatorsDefibrillators are either manual or automated (AED), withmonophasic or biphasic waveforms. For further informationsee Part 6, “Electrical Therapies: Automated External Defibrillators,Defibrillation, Cardioversion, and Pacing.”AEDs in institutions caring for children at risk for arrhythmiasand cardiac arrest (eg, hospitals, EDs) must be capableof recognizing <strong>pediatric</strong> cardiac rhythms and should ideallyhave a method of adjusting the energy level for children.The following should be considered when using a manualdefibrillator:Paddle SizeIn general, manual defibrillators have two sizes of hand-heldpaddles: adult and infant. The infant paddles may slide overor be located under the adult paddles. Manual defibrillatorscan also be used with hands-free pads that are self adhesive.Downloaded from circ.ahajournals.org by on October 20, <strong>2010</strong>