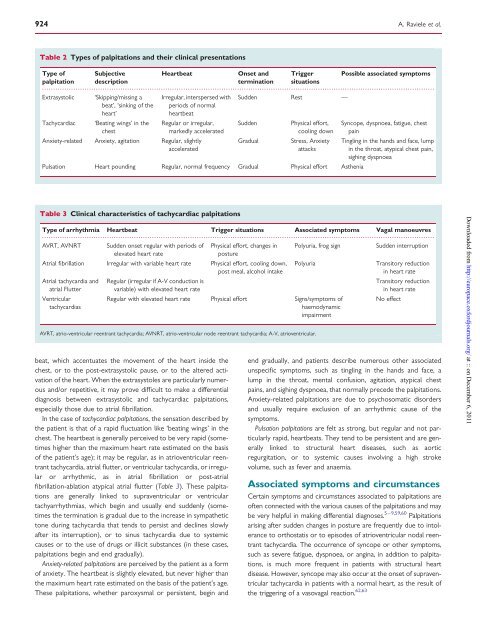
Managing <strong>patients</strong> <strong>with</strong> <strong>palpitations</strong> 923irregular heartbeat, history <strong>of</strong> heart disease, and event duration.5 min were found to be independent predictors <strong>of</strong> a cardiacaetiology. No specific cause <strong>of</strong> <strong>palpitations</strong> could be identified in16% <strong>of</strong> <strong>the</strong> <strong>patients</strong> despite a thorough evaluation including <strong>the</strong>use <strong>of</strong> loop recorders. Indeed, it is not always possible to establisha definite cause <strong>of</strong> <strong>palpitations</strong>; <strong>of</strong>ten, only a likely cause can begiven, and, in some cases, several possible causes have to betaken into consideration. 8,42 In <strong>the</strong> literature, <strong>the</strong>re are insufficientdata about <strong>the</strong> age and gender distribution <strong>of</strong> <strong>palpitations</strong>. Ingeneral, however, older <strong>patients</strong> and men are more likely tohave an arrhythmic cause <strong>of</strong> <strong>palpitations</strong> and younger <strong>patients</strong>47 – 51and women a psychosomatic cause.PrognosisThe prognostic implications <strong>of</strong> <strong>palpitations</strong> are dependent on <strong>the</strong>underlying aetiology as well as clinical characteristics <strong>of</strong> <strong>the</strong>patient. Available data, especially in terms <strong>of</strong> long-term prognosis,are scarce. Although <strong>palpitations</strong> are generally associated <strong>with</strong> lowrates <strong>of</strong> mortality, 4,47 <strong>the</strong>y should bring to attention a potentialserious condition in <strong>patients</strong> <strong>with</strong> structural or arrhythmogenicheart disease or a family history <strong>of</strong> sudden death. This is alsoimportant to keep in mind if <strong>the</strong> <strong>palpitations</strong> are associated <strong>with</strong>symptoms <strong>of</strong> haemodynamic impairment (dyspnoea, syncope, presyncope,dizziness, fatigue, chest pain, neurovegetative symptoms).5 On <strong>the</strong> one hand, depending on <strong>the</strong> clinical characteristics<strong>of</strong> <strong>the</strong> patient, <strong>palpitations</strong> due to arrhythmias, in particular <strong>of</strong> ventricularorigin, but also atrial fibrillation, are associated <strong>with</strong> differentprognostic implications. 15 – 17 On <strong>the</strong> o<strong>the</strong>r hand, in <strong>patients</strong><strong>with</strong>out relevant heart disease, <strong>palpitations</strong> (especially ifanxiety-related or extrasystolic) generally have a benign prognosis.A retrospective American study that analysed case recordsobtained <strong>from</strong> general practitioners found no difference in 5-yearmortality and morbidity between <strong>patients</strong> <strong>with</strong> <strong>palpitations</strong> and agroup <strong>of</strong> asymptomatic control subjects. 4 Also in <strong>the</strong> abovementionedstudy by Weber and Kapoor 47 on a general population <strong>of</strong><strong>patients</strong> presenting <strong>with</strong> <strong>palpitations</strong> at an university medicalcentre, despite <strong>the</strong> high rate <strong>of</strong> cardiac cause, 1-year mortalitywas only 1.6%. However, even in <strong>patients</strong> <strong>with</strong>out severe heartdisease, <strong>palpitations</strong> may be due to significant arrhythmias, suchas atrial fibrillation, atrial flutter, or ventricular ectopic beats, all<strong>of</strong> which require adequate investigation and treatment. Moreover,clinical characteristics <strong>of</strong> <strong>the</strong> patient, such as age, presence <strong>of</strong> heartdisease, and ECG abnormalities, do not always allow <strong>the</strong> physicianto identify a priori those cases in which <strong>palpitations</strong> are caused byclinically significant rhythm disorders. 8,47,48,52 – 54 An exception tothis is given by changes in <strong>the</strong> resting ECG that are indicative <strong>of</strong>primary electrical heart diseases.In athletes, <strong>palpitations</strong> are not uncommon. Sudden death, inparticular in younger athletes, is rare and mostly associated <strong>with</strong>underlying structural heart disease or primary arrhythmic disorders,and <strong>palpitations</strong> may be <strong>the</strong> initial clinical symptom or anincidental finding possibly leading to <strong>the</strong> recognition <strong>of</strong> a previouslyundiagnosed relevant heart disease. 55,56 Moreover, because <strong>of</strong>potentially life-threatening haemodynamic consequences <strong>of</strong> evensupraventricular arrhythmias, such as rapidly conducted preexcitedatrial fibrillation during exertion, careful cardiac evaluation,in particular <strong>of</strong> symptomatic competitive as well as recreationalathletes, is warranted. 57Although <strong>palpitations</strong> display a low mortality rate, <strong>the</strong> recurrence<strong>of</strong> symptoms is, however, very frequent. In <strong>the</strong> study by Weber andKapoor, 47 77% <strong>of</strong> <strong>patients</strong> experienced at least one recurrence <strong>of</strong><strong>palpitations</strong>, and <strong>the</strong> effect on <strong>the</strong>ir quality <strong>of</strong> life was unfavourable:one-third <strong>of</strong> <strong>patients</strong> reported an impairment <strong>of</strong> <strong>the</strong>ir ability toattend to household chores, 19% claimed that <strong>the</strong>ir workingcapacity had diminished, and 12% said that <strong>the</strong>y had taken days<strong>of</strong>f work. These findings are confirmed by a prospective study conductedby Barsky et al. 58 on 145 <strong>patients</strong> <strong>with</strong> <strong>palpitations</strong>, whowere followed up for 6 months and compared <strong>with</strong> an asymptomaticcontrol group. These authors observed that <strong>patients</strong> <strong>with</strong><strong>palpitations</strong>, in spite <strong>of</strong> having a favourable prognosis in terms <strong>of</strong>mortality, remained symptomatic and functionally impaired overtime and exhibited a high incidence <strong>of</strong> panic attacks and psychologicalsymptoms. 58 Frequent and recurrent <strong>palpitations</strong>, <strong>the</strong>refore,can impair <strong>the</strong> patient’s quality <strong>of</strong> life, giving rise to anxiety and frequentvisits to <strong>the</strong> emergency department. 3 In many respects, <strong>palpitations</strong>seem to behave like a chronic disorder that has afavourable prognosis, but <strong>with</strong> periodic attacks followed by transitoryremission. 3,4Clinical presentationDuration and frequency <strong>of</strong> <strong>palpitations</strong>With regard to duration, <strong>palpitations</strong> may be ei<strong>the</strong>r short-lasting orpersistent. In short-lasting forms, <strong>the</strong> symptom terminates spontaneously<strong>with</strong>in a brief period <strong>of</strong> time. In persistent forms, <strong>the</strong> <strong>palpitations</strong>are ongoing and terminate only after adequate medicaltreatment. With regard to frequency, <strong>palpitations</strong> may occurdaily, weekly, monthly, oryearly.Types <strong>of</strong> <strong>palpitations</strong>Patients report a wide range <strong>of</strong> sensations to describe <strong>the</strong>ir symptoms.The most common descriptions, and those most useful inclinical practice in differential diagnoses among <strong>the</strong> variouscauses <strong>of</strong> <strong>palpitations</strong>, enable <strong>palpitations</strong> to be classified accordingto <strong>the</strong> rate, rhythm, and intensity <strong>of</strong> heartbeat 5 – 9,59,60 : extrasystolic<strong>palpitations</strong>, tachycardiac <strong>palpitations</strong>, anxiety-related <strong>palpitations</strong>,and pulsation <strong>palpitations</strong> (Table 2). It should, however, be stressedthat <strong>patients</strong> are not always able to describe <strong>the</strong> characteristics <strong>of</strong><strong>the</strong>ir symptoms precisely. It may <strong>the</strong>refore be difficult to identify<strong>the</strong> type <strong>of</strong> palpitation accurately, especially in <strong>the</strong> case <strong>of</strong> normalrate<strong>palpitations</strong>. 5,9,61Extrasystolic <strong>palpitations</strong>, due to ectopic beats, generally producefeelings <strong>of</strong> ‘missing/skipping a beat’ and/or a ‘sinking <strong>of</strong> <strong>the</strong> heart’interspersed <strong>with</strong> periods during which <strong>the</strong> heart beats normally;<strong>patients</strong> report that <strong>the</strong> heart seems to stop and <strong>the</strong>n startagain, causing an unpleasant, almost painful, sensation <strong>of</strong> a blowto <strong>the</strong> chest. Linked to <strong>the</strong> presence <strong>of</strong> atrial or ventricular extrasystolicbeats, this type <strong>of</strong> palpitation is frequently encounteredeven in young subjects, <strong>of</strong>ten in <strong>the</strong> absence <strong>of</strong> heart disease,and generally has a benign prognosis. In extrasystolic <strong>palpitations</strong>,particularly if <strong>the</strong>y are <strong>of</strong> ventricular origin, <strong>the</strong> sensation is dueto <strong>the</strong> increased strength <strong>of</strong> contraction <strong>of</strong> <strong>the</strong> post-extrasystolicDownloaded <strong>from</strong> http://europace.oxfordjournals.org/ at :: on December 6, 2011
924A. Raviele et al.Table 2 Types <strong>of</strong> <strong>palpitations</strong> and <strong>the</strong>ir clinical presentationsType <strong>of</strong> SubjectiveHeartbeatOnset and Trigger Possible associated symptomspalpitation descriptiontermination situations...............................................................................................................................................................................Extrasystolic ‘Skipping/missing a Irregular, interspersed <strong>with</strong> Sudden Rest —beat’, ‘sinking <strong>of</strong> <strong>the</strong> periods <strong>of</strong> normalheart’heartbeatTachycardiac‘Beating wings’ in <strong>the</strong>chestRegular or irregular,markedly acceleratedAnxiety-related Anxiety, agitation Regular, slightlyacceleratedSuddenGradualPhysical effort,cooling downStress, AnxietyattacksPulsation Heart pounding Regular, normal frequency Gradual Physical effort As<strong>the</strong>niaSyncope, dyspnoea, fatigue, chestpainTingling in <strong>the</strong> hands and face, lumpin <strong>the</strong> throat, atypical chest pain,sighing dyspnoeaTable 3 Clinical characteristics <strong>of</strong> tachycardiac <strong>palpitations</strong>Type <strong>of</strong> arrhythmia Heartbeat Trigger situations Associated symptoms Vagal manoeuvres...............................................................................................................................................................................AVRT, AVNRT Sudden onset regular <strong>with</strong> periods <strong>of</strong> Physical effort, changes in Polyuria, frog signSudden interruptionelevated heart ratepostureAtrial fibrillation Irregular <strong>with</strong> variable heart rate Physical effort, cooling down,post meal, alcohol intakeAtrial tachycardia andatrial FlutterVentriculartachycardiasbeat, which accentuates <strong>the</strong> movement <strong>of</strong> <strong>the</strong> heart inside <strong>the</strong>chest, or to <strong>the</strong> post-extrasystolic pause, or to <strong>the</strong> altered activation<strong>of</strong> <strong>the</strong> heart. When <strong>the</strong> extrasystoles are particularly numerousand/or repetitive, it may prove difficult to make a differentialdiagnosis between extrasystolic and tachycardiac <strong>palpitations</strong>,especially those due to atrial fibrillation.In <strong>the</strong> case <strong>of</strong> tachycardiac <strong>palpitations</strong>, <strong>the</strong> sensation described by<strong>the</strong> patient is that <strong>of</strong> a rapid fluctuation like ‘beating wings’ in <strong>the</strong>chest. The heartbeat is generally perceived to be very rapid (sometimeshigher than <strong>the</strong> maximum heart rate estimated on <strong>the</strong> basis<strong>of</strong> <strong>the</strong> patient’s age); it may be regular, as in atrioventricular reentranttachycardia, atrial flutter, or ventricular tachycardia, or irregularor arrhythmic, as in atrial fibrillation or post-atrialfibrillation-ablation atypical atrial flutter (Table 3). These <strong>palpitations</strong>are generally linked to supraventricular or ventriculartachyarrhythmias, which begin and usually end suddenly (sometimes<strong>the</strong> termination is gradual due to <strong>the</strong> increase in sympa<strong>the</strong>tictone during tachycardia that tends to persist and declines slowlyafter its interruption), or to sinus tachycardia due to systemiccauses or to <strong>the</strong> use <strong>of</strong> drugs or illicit substances (in <strong>the</strong>se cases,<strong>palpitations</strong> begin and end gradually).Anxiety-related <strong>palpitations</strong> are perceived by <strong>the</strong> patient as a form<strong>of</strong> anxiety. The heartbeat is slightly elevated, but never higher than<strong>the</strong> maximum heart rate estimated on <strong>the</strong> basis <strong>of</strong> <strong>the</strong> patient’s age.These <strong>palpitations</strong>, whe<strong>the</strong>r paroxysmal or persistent, begin andPolyuriaRegular (irregular if A-V conduction isvariable) <strong>with</strong> elevated heart rateRegular <strong>with</strong> elevated heart rate Physical effort Signs/symptoms <strong>of</strong>haemodynamicimpairmentAVRT, atrio-ventricular reentrant tachycardia; AVNRT, atrio-ventricular node reentrant tachycardia; A-V, atrioventricular.Transitory reductionin heart rateTransitory reductionin heart rateNo effectend gradually, and <strong>patients</strong> describe numerous o<strong>the</strong>r associatedunspecific symptoms, such as tingling in <strong>the</strong> hands and face, alump in <strong>the</strong> throat, mental confusion, agitation, atypical chestpains, and sighing dyspnoea, that normally precede <strong>the</strong> <strong>palpitations</strong>.Anxiety-related <strong>palpitations</strong> are due to psychosomatic disordersand usually require exclusion <strong>of</strong> an arrhythmic cause <strong>of</strong> <strong>the</strong>symptoms.Pulsation <strong>palpitations</strong> are felt as strong, but regular and not particularlyrapid, heartbeats. They tend to be persistent and are generallylinked to structural heart diseases, such as aorticregurgitation, or to systemic causes involving a high strokevolume, such as fever and anaemia.Associated symptoms and circumstancesCertain symptoms and circumstances associated to <strong>palpitations</strong> are<strong>of</strong>ten connected <strong>with</strong> <strong>the</strong> various causes <strong>of</strong> <strong>the</strong> <strong>palpitations</strong> and maybe very helpful in making differential diagnoses. 5–9,59,60 Palpitationsarising after sudden changes in posture are frequently due to intoleranceto orthostatis or to episodes <strong>of</strong> atrioventricular nodal reentranttachycardia. The occurrence <strong>of</strong> syncope or o<strong>the</strong>r symptoms,such as severe fatigue, dyspnoea, or angina, in addition to <strong>palpitations</strong>,is much more frequent in <strong>patients</strong> <strong>with</strong> structural heartdisease. However, syncope may also occur at <strong>the</strong> onset <strong>of</strong> supraventriculartachycardia in <strong>patients</strong> <strong>with</strong> a normal heart, as <strong>the</strong> result <strong>of</strong><strong>the</strong> triggering <strong>of</strong> a vasovagal reaction. 62,63Downloaded <strong>from</strong> http://europace.oxfordjournals.org/ at :: on December 6, 2011