

Journal 1pages FINAL 34- - National Board Of Examination
Journal 1pages FINAL 34- - National Board Of Examination
Journal 1pages FINAL 34- - National Board Of Examination

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
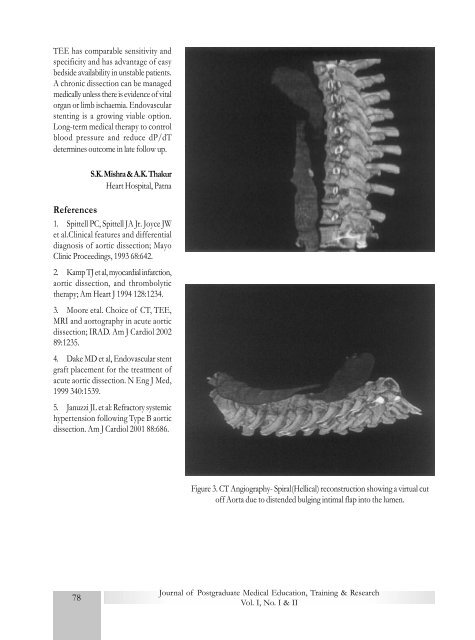
TEE has comparable sensitivity andspecificity and has advantage of easybedside availability in unstable patients.A chronic dissection can be managedmedically unless there is evidence of vitalorgan or limb ischaemia. Endovascularstenting is a growing viable option.Long-term medical therapy to controlblood pressure and reduce dP/dTdetermines outcome in late follow up.S.K. Mishra & A.K. ThakurHeart Hospital, PatnaReferences1. Spittell PC, Spittell JA Jr. Joyce JWet al.Clinical features and differentialdiagnosis of aortic dissection; MayoClinic Proceedings, 1993 68:642.2. Kamp TJ et al, myocardial infarction,aortic dissection, and thrombolytictherapy; Am Heart J 1994 128:12<strong>34</strong>.3. Moore etal. Choice of CT, TEE,MRI and aortography in acute aorticdissection; IRAD. Am J Cardiol 200289:1235.4. Dake MD et al, Endovascular stentgraft placement for the treatment ofacute aortic dissection. N Eng J Med,1999 <strong>34</strong>0:1539.5. Januzzi JL et al: Refractory systemichypertension following Type B aorticdissection. Am J Cardiol 2001 88:686.Figure 3. CT Angiography- Spiral(Hellical) reconstruction showing a virtual cutoff Aorta due to distended bulging intimal flap into the lumen.78<strong>Journal</strong> of Postgraduate Medical Education, Training & ResearchVol. I, No. I & II













