Guidelines for field staff to assist people living in ... - Housing NSW
Guidelines for field staff to assist people living in ... - Housing NSW
Guidelines for field staff to assist people living in ... - Housing NSW

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Guidel<strong>in</strong>es</strong> <strong>for</strong> <strong>field</strong> <strong>staff</strong> <strong>to</strong><strong>assist</strong><strong>people</strong> <strong>liv<strong>in</strong>g</strong> <strong>in</strong> severedomestic squalorAugust 2007
TABLE OF CONTENTSSection 1: Introduction 41.1 Background1.2 Purpose of the <strong>Guidel<strong>in</strong>es</strong>Section 2: Expla<strong>in</strong><strong>in</strong>g severe domestic squalor 52.1 Def<strong>in</strong>ition of severe domestic squalor2.2 Incidence of severe domestic squalor2.3 Features of persons <strong>liv<strong>in</strong>g</strong> <strong>in</strong> severe domesticsqualorSection 3: Referral 83.1 Sources of referral3.2 In<strong>for</strong>mation gather<strong>in</strong>g prior <strong>to</strong> <strong>in</strong>itial contact3.3 Gather<strong>in</strong>g resources <strong>for</strong> use at the visitSection 4: The <strong>in</strong>itial visit 104.1 Purpose4.2 Approaches <strong>to</strong> engag<strong>in</strong>g the person4.3 Ensure OH&S requirements can be met4.4 Assess<strong>in</strong>g the level of squalor4.5 Assess<strong>in</strong>g the impact of squalor on the person,family and/or local community4.5.1 Impact of squalor on the person’s healthand lifestyle4.5.2 Impact of squalor on the familyand/or local community4.6 Initiate referrals <strong>to</strong> address critical needs4.6.1 Medical and/or psychiatric review4.6.2 Assistance with activities of daily <strong>liv<strong>in</strong>g</strong> (ADL)4.6.3 Assess<strong>in</strong>g the risk on dependents4.6.4 Relocation of pets4.6.5 Organise a clear up if an urgent OH&Srisk presents, and the person supportsthis <strong>in</strong>terventionSection 5: Interagency cooperation 175.1 Coord<strong>in</strong>ation of services and developmen<strong>to</strong>f Action Plans5.2 Ongo<strong>in</strong>g moni<strong>to</strong>r<strong>in</strong>g5.3 Flow Chart 1: Assessment and support <strong>for</strong><strong>people</strong> <strong>liv<strong>in</strong>g</strong> <strong>in</strong> squalorSection 6: Organis<strong>in</strong>g referrals <strong>to</strong> relevantagencies and service providers 206.1 Clean<strong>in</strong>g up6.2 Service providers and agencies2
Section 7: Strategies <strong>to</strong> help <strong>people</strong> who areunwill<strong>in</strong>g <strong>to</strong> accept <strong>assist</strong>ance 237.1 When the person has decision-mak<strong>in</strong>gcapacity7.2 When the person’s decision-mak<strong>in</strong>gcapacity cannot be assessedSection 8: Strategies <strong>to</strong> <strong>assist</strong> <strong>people</strong> who haveimpaired decision-mak<strong>in</strong>g capacity 258.1 Decision-mak<strong>in</strong>g capacity8.2 Guardianship and F<strong>in</strong>ancial Management Orders8.3 Flow Chart 2: Support <strong>for</strong> <strong>people</strong> who areunwill<strong>in</strong>g <strong>to</strong> accept <strong>assist</strong>anceSection 9: Conclusions 27APPENDICES1. Occupational Health and Safety Checklist 282. Environmental Cleanl<strong>in</strong>ess and ClutterScale (ECCS) 293. Impact of Squalor Checklist 334. Squalor Action Plan 345. Services and agencies support<strong>in</strong>g <strong>people</strong><strong>liv<strong>in</strong>g</strong> <strong>in</strong> domestic squalor 356. Organisations that can <strong>assist</strong> when <strong>people</strong> areunwill<strong>in</strong>g <strong>to</strong> accept <strong>assist</strong>ance 437. Supports <strong>for</strong> <strong>people</strong> with impaired decision-mak<strong>in</strong>gcapacity 468. Case Studies 1–6 499. <strong>NSW</strong> Government and non-Government agencies 5610. Table of abbreviations 5811. Further read<strong>in</strong>g 5912. Acknowledgements 603
SECTION 1: Introduction1.1 BackgroundDur<strong>in</strong>g 2004, the Department of Age<strong>in</strong>g, Disability and Home Care (DADHC) fundeda review of the services provided <strong>to</strong> <strong>people</strong> who live <strong>in</strong> severe domestic squalor. Theaim of this review was <strong>to</strong> develop <strong>Guidel<strong>in</strong>es</strong> <strong>for</strong> personnel who are asked <strong>to</strong><strong>in</strong>tervene <strong>in</strong> cases of severe domestic squalor, particularly <strong>staff</strong> provid<strong>in</strong>g Home andCommunity Care (HACC) funded services.The development of <strong>Guidel<strong>in</strong>es</strong> is an <strong>in</strong>itiative of the (then) Partnerships Aga<strong>in</strong>stHomelessness (PAH) Committee. The project was auspiced by the Central SydneyArea Health Service (now the Sydney South West Area Health Service) andcoord<strong>in</strong>ated <strong>in</strong>itially by a Reference Group 1 , compris<strong>in</strong>g representatives withexperience <strong>in</strong> <strong>assist</strong><strong>in</strong>g <strong>people</strong> <strong>liv<strong>in</strong>g</strong> <strong>in</strong> squalor. Professor John Snowdon, apsychiatrist with a special <strong>in</strong>terest <strong>in</strong> the area, was appo<strong>in</strong>ted Chairperson of theGroup. A consultant was recruited <strong>to</strong> conduct a review of the evidence relevant <strong>to</strong>squalor, <strong>to</strong> consult stakeholder groups and <strong>to</strong> write a report. Based on this report,these <strong>Guidel<strong>in</strong>es</strong> have been developed.1.2 Purpose of the <strong>Guidel<strong>in</strong>es</strong>These <strong>Guidel<strong>in</strong>es</strong> are designed <strong>to</strong> <strong>assist</strong> <strong>field</strong> <strong>staff</strong> 2 of various government and nongovernmentagencies <strong>to</strong> constructively <strong>in</strong>tervene, and improve the situation of <strong>people</strong>who are <strong>liv<strong>in</strong>g</strong> <strong>in</strong> severe domestic squalor. The <strong>in</strong>tention is <strong>to</strong> improve the efficiency,speed of action and coord<strong>in</strong>ation of work between relevant agencies, result<strong>in</strong>g <strong>in</strong>improved health and quality of life <strong>for</strong> <strong>in</strong>dividuals who have been <strong>liv<strong>in</strong>g</strong> <strong>in</strong> severedomestic squalor.These <strong>Guidel<strong>in</strong>es</strong> provide <strong>field</strong> <strong>staff</strong> with:• a step-by-step guide• simplified procedures <strong>to</strong> <strong>assist</strong> <strong>people</strong> <strong>liv<strong>in</strong>g</strong> <strong>in</strong> severe domestic squalor• clear roles and responsibilities of agencies and service providers, <strong>to</strong> enableimproved coord<strong>in</strong>ation and <strong>in</strong>tegration of services• practical <strong>in</strong><strong>for</strong>mation regard<strong>in</strong>g referrals and <strong>in</strong>tervention options.These <strong>Guidel<strong>in</strong>es</strong> <strong>in</strong>clude flow charts <strong>to</strong> summarise the processes <strong>in</strong>volved. Included<strong>in</strong> Appendix 8 are a series of case studies (prepared by Graeme Halliday), whichexpla<strong>in</strong> the issues and current events aris<strong>in</strong>g <strong>in</strong> typical cases of severe domesticsqualor.1 A list of Reference Group participants and other <strong>people</strong> who contributed <strong>to</strong> the project appears at Appendix 12.2 The term ‘<strong>field</strong> <strong>staff</strong>’ is used <strong>to</strong> cover a broad range of front-l<strong>in</strong>e workers <strong>in</strong> government and non-governmentsett<strong>in</strong>gs who, because of deal<strong>in</strong>g face <strong>to</strong> face with clients, come <strong>in</strong><strong>to</strong> contact with or are the first po<strong>in</strong>t of referral<strong>for</strong> <strong>people</strong> <strong>liv<strong>in</strong>g</strong> <strong>in</strong> domestic squalor.4
SECTION 2: Expla<strong>in</strong><strong>in</strong>g severe domestic squalor2.1 Def<strong>in</strong>ition of severe domestic squalorDictionary def<strong>in</strong>itions of squalor refer <strong>to</strong> conditions that are filthy, unclean or foulthrough neglect. Commonly, this results from a person’s failure <strong>to</strong> remove householdwaste and other rubbish <strong>in</strong>clud<strong>in</strong>g papers, wrapp<strong>in</strong>g, food products, cook<strong>in</strong>g waste,conta<strong>in</strong>ers and broken or discarded household items.Cleanl<strong>in</strong>ess varies between homes and between <strong>in</strong>dividuals and can be presumed <strong>to</strong> be<strong>in</strong>fluenced by multiple fac<strong>to</strong>rs, <strong>in</strong>clud<strong>in</strong>g upbr<strong>in</strong>g<strong>in</strong>g, peer and family expectations, <strong>liv<strong>in</strong>g</strong>arrangements, social and f<strong>in</strong>ancial circumstances, cultural background and surround<strong>in</strong>gs.Some <strong>people</strong> live <strong>in</strong> conditions so filthy and unhygienic that almost all observers, <strong>in</strong>whatever culture, would consider them unacceptable.The term ‘severe domestic squalor’ was chosen <strong>in</strong> order <strong>to</strong> emphasise, firstly that thefocus is not on cases where <strong>people</strong> live <strong>in</strong> somewhat unclean surround<strong>in</strong>gs, even if theyhave severe physical or mental disorders. The concern is <strong>for</strong> <strong>people</strong> who live <strong>in</strong>disgust<strong>in</strong>g conditions. This word is used advisedly <strong>in</strong> order <strong>to</strong> make clear that theuncleanl<strong>in</strong>ess <strong>in</strong> relevant cases is extreme. Secondly, the aim is not <strong>to</strong> provide guidance<strong>in</strong> cases of self-neglect where squalor is not an issue, nor <strong>in</strong> cases of hoard<strong>in</strong>g withoutsqualor, i.e., those cases where there has been an accumulation of possessions but <strong>in</strong> anordered, clean and manageable way. What is <strong>in</strong>cluded are cases of hoard<strong>in</strong>g where theaccumulation has led <strong>to</strong> the <strong>liv<strong>in</strong>g</strong> environment be<strong>in</strong>g unclean, unsanitary or dangerous(e.g., because of fire risk).There is a range of types of squalor, <strong>in</strong>clud<strong>in</strong>g:• Neglect, <strong>in</strong>volv<strong>in</strong>g failure <strong>to</strong> remove household waste and other rubbish <strong>in</strong>clud<strong>in</strong>gpapers, wrapp<strong>in</strong>g, food, cook<strong>in</strong>g waste, conta<strong>in</strong>ers and discarded household items.• Multifaceted self-neglect, where the person fails <strong>to</strong> ma<strong>in</strong>ta<strong>in</strong> aspects of their care,health and lifestyle, such as personal care, eat<strong>in</strong>g adequately or fail<strong>in</strong>g <strong>to</strong> takemedications as prescribed.• Deliberate hoard<strong>in</strong>g and the excessive accumulation of items such as cloth<strong>in</strong>g,newspapers, electrical appliances, etc. This may <strong>in</strong>volve hoard<strong>in</strong>g of animals.For the purpose of these <strong>Guidel<strong>in</strong>es</strong>, the term severe domestic squalor <strong>in</strong>cludes:• extreme household uncleanl<strong>in</strong>ess• hoard<strong>in</strong>g, where the accumulation of material has led <strong>to</strong> the <strong>liv<strong>in</strong>g</strong> environment be<strong>in</strong>gunclean, unsanitary or dangerous, e.g., conditions pose a fire risk.The decision regard<strong>in</strong>g whether or not a person lives <strong>in</strong> severe domestic squalor maybe <strong>in</strong>fluenced by the attitude, culture, exposure <strong>to</strong> unclean environments andpersonal <strong>liv<strong>in</strong>g</strong> conditions of the person mak<strong>in</strong>g the assessment. An objectiveassessment <strong>to</strong>ol has been developed <strong>to</strong> assess the level of squalor (see Section4.4).5
2.2 Incidence of severe domestic squalorBetween 2000 and 2005, 120 cases of <strong>people</strong> <strong>liv<strong>in</strong>g</strong> <strong>in</strong> severe domestic squalor werereferred <strong>to</strong> an old age psychiatry team <strong>in</strong> Sydney, suggest<strong>in</strong>g an annual <strong>in</strong>cidence of10 <strong>people</strong> aged over 65 years per 10,000 (Halliday & Snowdon, unpublished data2005). However, s<strong>in</strong>ce numerous cases of severe squalor are never referred <strong>to</strong>medical services, the actual <strong>in</strong>cidence is likely <strong>to</strong> be considerably higher.In 2000, a study <strong>in</strong> London of 81 clients visited by a local authority special clean<strong>in</strong>gservice found that:• 51% were younger than 65 years• 72% were men• 84% lived alone• 70% had one or more mental disorders• 32% were diagnosed with substance abuse and around 50% of those who abusedsubstances also suffered from an organic bra<strong>in</strong> disorder (mostly dementia),schizophrenia or a related disorder• 10% met criteria <strong>for</strong> a developmental disorder• 85% had at least one chronic physical health problem• 26% of the <strong>people</strong> had a physical health problem, such as immobility or sensoryimpairment, contribut<strong>in</strong>g <strong>to</strong> the unclean state of their <strong>liv<strong>in</strong>g</strong> environment• 28% regarded their home as ‘clean’ or ‘very clean’ when asked about their <strong>liv<strong>in</strong>g</strong>conditions (Halliday et al., 2000).2.3 Features of persons <strong>liv<strong>in</strong>g</strong> <strong>in</strong> severe domestic squalorThe evidence suggests that half <strong>to</strong> two-thirds of all persons <strong>liv<strong>in</strong>g</strong> <strong>in</strong> severe domesticsqualor suffer from dementia or alcohol-related bra<strong>in</strong> damage, or mental disorderssuch as schizophrenia and depression. Most studies refer <strong>to</strong> <strong>in</strong>dividuals who areisolated, suspicious and unfriendly, and have features suggestive of pre-exist<strong>in</strong>gpersonality disorders.Studies have also shown moderate <strong>to</strong> high rates of medical problems <strong>for</strong> <strong>people</strong> wholive <strong>in</strong> conditions of severe domestic squalor, particularly <strong>in</strong> relation <strong>to</strong> mobility,cont<strong>in</strong>ence, sensory impairment (especially visual) and nutritional deficiencies suchas diabetes, obesity, etc.An <strong>in</strong>dividual who lives <strong>in</strong> domestic squalor may be completely <strong>in</strong>dependent. If<strong>people</strong> are <strong>liv<strong>in</strong>g</strong> <strong>in</strong> squalor and not caus<strong>in</strong>g any harm <strong>to</strong> themselves or others, thenno <strong>in</strong>tervention is required.A person who lives <strong>in</strong> squalor is frequently opposed <strong>to</strong> assessment and <strong>assist</strong>ance,and may be unaware that there is a problem. The client may be suspicious orevasive, perceiv<strong>in</strong>g the assessment as a potential threat <strong>to</strong> their <strong>in</strong>dependence.Reasons <strong>for</strong> this vary. In some cases it results from apathy associated with anunderly<strong>in</strong>g mental disorder. In others, longstand<strong>in</strong>g habits and the <strong>in</strong>dividual’spersonality traits, <strong>in</strong>clud<strong>in</strong>g rigidity, unfriendl<strong>in</strong>ess, suspiciousness, anxiety oravoidance could be the cause. In the case of Aborig<strong>in</strong>al <strong>people</strong>, there may be ahis<strong>to</strong>ry of unsatisfac<strong>to</strong>ry deal<strong>in</strong>gs with service providers. Cultural and languagebarriers may also contribute <strong>to</strong> opposition <strong>to</strong> assessment and <strong>assist</strong>ance.6
If such persons do agree <strong>to</strong> speak, they are unlikely <strong>to</strong> be prepared <strong>to</strong> leave thedwell<strong>in</strong>g. L<strong>in</strong>ks with social supports and family have often been lost.In the most extreme cases, where there is a substantial risk <strong>to</strong> the <strong>in</strong>dividual orothers, it may be necessary <strong>to</strong> refer <strong>to</strong> agencies and service providers that can<strong>in</strong>tervene <strong>to</strong> provide <strong>assist</strong>ance (see Sections 7 and 8).7
SECTION 3: Referral3.1 Sources of referralPeople <strong>liv<strong>in</strong>g</strong> <strong>in</strong> states of severe domestic squalor may be referred <strong>for</strong> <strong>assist</strong>ance byanyone. Common referrers are relatives, neighbours, concerned local residents,service providers, the Fire Brigade, police and shopkeepers. More commonly,<strong>people</strong> come <strong>to</strong> the attention of various service providers because of the deleteriouseffect that their <strong>liv<strong>in</strong>g</strong> conditions have on themselves and the surround<strong>in</strong>g community.As an example, see Case Study 1 and Case Study 4 <strong>in</strong> Appendix 8.If a person is known <strong>to</strong> have a health problem or <strong>to</strong> receive welfare <strong>assist</strong>ance, helpmay be sought from the relevant health service or from welfare agency <strong>staff</strong>. Theperson’s type of accommodation may determ<strong>in</strong>e whether the person is referred <strong>for</strong><strong>assist</strong>ance <strong>to</strong> the Department of Hous<strong>in</strong>g (DOH) or <strong>to</strong> the local council. Landlords orreal estate agents may need <strong>to</strong> be approached if utilities (such as water) have beendisconnected or the build<strong>in</strong>g is <strong>in</strong> a state of disrepair.3.2 In<strong>for</strong>mation gather<strong>in</strong>g prior <strong>to</strong> <strong>in</strong>itial contactPrior <strong>to</strong> visit<strong>in</strong>g someone who lives <strong>in</strong> squalor, try <strong>to</strong> f<strong>in</strong>d out as much <strong>in</strong><strong>for</strong>mation aspossible about the person. This will <strong>assist</strong> <strong>in</strong> determ<strong>in</strong><strong>in</strong>g who the best person is <strong>to</strong>undertake an <strong>in</strong>itial assessment, and how this assessment should be conducted.Try <strong>to</strong> access the follow<strong>in</strong>g background <strong>in</strong><strong>for</strong>mation from the referrer and any othersources:• best time of day <strong>to</strong> visit• length of time the person has been <strong>liv<strong>in</strong>g</strong> <strong>in</strong> unclean conditions• type of accommodation e.g., homeowner, private rental, Department of Hous<strong>in</strong>g(DoH)• if the person has a next of k<strong>in</strong>, carer, supportive neighbours or <strong>in</strong>volvement of anyhome services• any known medical his<strong>to</strong>ry and/or whether or not the person has a GeneralPractitioner• any potential occupational health and safety issues <strong>for</strong> which special cloth<strong>in</strong>g orprecautions may be required (see OH&S Checklist on page 28).• his<strong>to</strong>ry of the person’s character, habits, and past medical and psychiatric his<strong>to</strong>ry• cultural background (Aborig<strong>in</strong>al person or Torres Strait Islander), culturally andl<strong>in</strong>guistically diverse (CALD) background• if there are language or communication barriers• preferred language spoken and whether an <strong>in</strong>terpreter may be required• his<strong>to</strong>ry of substance abuse, mental illness, aggression or crim<strong>in</strong>al behaviour• whether the person lives alone or with dependents and any details of dependents• whether premises are covered by an exist<strong>in</strong>g Council Order (see page 11).8
3.3 Gather<strong>in</strong>g resources <strong>for</strong> use at the visitResources that may be used at the <strong>in</strong>itial visit <strong>in</strong>clude the follow<strong>in</strong>g:• Occupational Health and Safety (OH&S) Checklist (Appendix 1)• Environmental Cleanl<strong>in</strong>ess and Clutter Scale (ECCS) (Appendix 2)• Impact of Squalor Checklist (Appendix 3)• Squalor Action Plan (Appendix 4).9
SECTION 4: The Initial Visit4.1 PurposeThe purpose of conduct<strong>in</strong>g a home visit <strong>to</strong> the person is <strong>to</strong>:1. assess whether the person lives <strong>in</strong> squalor and <strong>to</strong> rate the extent of the squalor2. assess whether the person hoards excessively and/or self-neglects, i.e., doesnot adequately look after his/her bodily requirements and hygiene3. assess the nature and severity of any associated health and lifestyle issues4. make a prelim<strong>in</strong>ary identification of strategies required <strong>to</strong> address the issuesidentified.If a home assessment is not <strong>in</strong>itially possible, <strong>in</strong><strong>for</strong>mation available <strong>to</strong> the agencymay permit identification of the issues <strong>to</strong> be addressed. Case management plansshould <strong>in</strong>clude eventual entry <strong>to</strong> the home, preferably with the consent and<strong>in</strong>volvement of the occupant.The issue of consent <strong>in</strong> relation <strong>to</strong> decision-mak<strong>in</strong>g capacity is complex and is dealtwith <strong>in</strong> more detail <strong>in</strong> Section 8. Field <strong>staff</strong> should also refer <strong>to</strong> their own agency’sconsent procedures.4.2 Approaches <strong>to</strong> engag<strong>in</strong>g the personPeople <strong>liv<strong>in</strong>g</strong> <strong>in</strong> severe domestic squalor vary markedly <strong>in</strong> their nature, personality style,acceptance, cooperation, <strong>in</strong>sight and perception of their circumstances. As aconsequence, there is a need <strong>for</strong> flexibility <strong>in</strong> the approach taken by caseworkers. Some<strong>people</strong> may respond <strong>to</strong> a series of <strong>in</strong>itial, brief, casual meet<strong>in</strong>gs. Others may be morelikely <strong>to</strong> respond <strong>to</strong> a visit by someone perceived <strong>to</strong> be <strong>in</strong> authority, such as a fire officeror the Police. However, cultural sensitivity and appropriateness is important here, assome <strong>people</strong> may feel uncom<strong>for</strong>table with authority figures, which may <strong>in</strong>tensify feel<strong>in</strong>gsof fear and suspicion.Generally, the person is more likely <strong>to</strong> be successfully engaged if an <strong>in</strong>terest is shown <strong>in</strong>them and their particular reason <strong>for</strong> need<strong>in</strong>g help. If the person agrees <strong>to</strong> accept help,the likelihood of achiev<strong>in</strong>g significant change and improv<strong>in</strong>g conditions <strong>for</strong> the <strong>in</strong>dividualand others is considerably greater.Options that could be considered <strong>in</strong>clude:• If the person is <strong>to</strong>o fearful <strong>to</strong> open the door, try leav<strong>in</strong>g a note <strong>in</strong> the mailbox orunder the door, ask<strong>in</strong>g them <strong>to</strong> make contact. Keep<strong>in</strong>g privacy concerns <strong>in</strong> m<strong>in</strong>d,discrete enquiries with neighbours might be of <strong>assist</strong>ance.• Repeat visits by a key worker. Sometimes call<strong>in</strong>g after hours, vary<strong>in</strong>g the hours orvisit<strong>in</strong>g on several occasions may <strong>assist</strong> <strong>to</strong> engage the person.• If the person is of Aborig<strong>in</strong>al or Torres Strait Islander or CALD background,arrang<strong>in</strong>g <strong>to</strong> visit with a worker from the particular background or with anaccredited <strong>in</strong>terpreter may be appropriate. Check with the client as <strong>to</strong> theirpreference and consent prior <strong>to</strong> mak<strong>in</strong>g any arrangements.10
• If the person is from a CALD background, encourage them <strong>to</strong> use their preferredlanguage.• If the person requests an <strong>in</strong>terpreter or has <strong>in</strong>adequate language skills, aprofessional <strong>in</strong>terpreter should be used. Refer <strong>to</strong> your organisation’s proceduresregard<strong>in</strong>g the engagement and use of <strong>in</strong>terpreters. Cultural and l<strong>in</strong>guistic fac<strong>to</strong>rscan impact on the success of engagement with the person.• Ask the person how he/she feels that they could benefit from help, and identify theperceived needs.• Be persistent, sensitive <strong>to</strong> the person’s needs and careful not <strong>to</strong> overwhelm them.Even if their <strong>in</strong>itial reaction is negative and they reject any <strong>in</strong>tervention, it is stillimportant <strong>to</strong> cont<strong>in</strong>ue <strong>to</strong> try <strong>to</strong> establish a relationship.• Avoid impos<strong>in</strong>g your own values and judgement. Many <strong>people</strong> <strong>liv<strong>in</strong>g</strong> <strong>in</strong> squaloroften do not even perceive that their home is dirty.• Take time. An immediate focus on a need <strong>for</strong> clean<strong>in</strong>g can cause distress, andsabotage chances of achiev<strong>in</strong>g a successful alliance.• Reframe the need <strong>for</strong> clean<strong>in</strong>g <strong>in</strong> terms of the person’s perceived needs andpreferences. The person might agree <strong>to</strong> tidy up as a staged process. Wherepossible, establish an <strong>in</strong>ven<strong>to</strong>ry of possessions, identify valuables and arrange <strong>for</strong>them <strong>to</strong> be placed securely.• Ensure that the person has the capacity 3 <strong>to</strong> make decisions about giv<strong>in</strong>g awayproperty, and that service <strong>staff</strong> do not accept gifts or directly benefit from the cleanup.It is important <strong>to</strong> note that <strong>in</strong> situations of extreme squalor, the assessment of ‘risk’ islikely <strong>to</strong> vary between the relevant authorities. The evaluation of a <strong>field</strong> <strong>staff</strong> may notcorrespond with that of the local council’s environmental health officer . Situationsshould be avoided where one course of action is advised by a <strong>field</strong> <strong>staff</strong> but another ispursued by the local council (as the council does not need the consent of the resident <strong>to</strong><strong>in</strong>voke its clean up powers). It would be useful, there<strong>for</strong>e <strong>for</strong> <strong>field</strong> <strong>staff</strong> <strong>to</strong> liaise with therelevant local council be<strong>for</strong>e mak<strong>in</strong>g an assessment on <strong>in</strong>tervention and advis<strong>in</strong>g theperson on what will happen. This would also allow the <strong>field</strong> <strong>staff</strong> <strong>to</strong> determ<strong>in</strong>e whetherthe residential premises are subject <strong>to</strong> an exist<strong>in</strong>g order (which may be <strong>in</strong> effect <strong>for</strong> aperiod of up <strong>to</strong> five years).When shar<strong>in</strong>g <strong>in</strong><strong>for</strong>mation with other agencies, be sure that disclosure of <strong>in</strong><strong>for</strong>mation isdirectly related <strong>to</strong> the purpose <strong>for</strong> which it was given and collected.4.3 Ensure OH&S requirements can be metThe Occupational Health and Safety (OH&S) of persons enter<strong>in</strong>g premises wheresqualor is evident, and the safety of the person/s <strong>liv<strong>in</strong>g</strong> <strong>in</strong> these conditions is asignificant issue. Workers that provide services <strong>to</strong> <strong>people</strong> <strong>liv<strong>in</strong>g</strong> <strong>in</strong> squalor mustcomply with their organisation’s OH&S policy and procedures.3 The issue of ‘capacity’ is complex and is discussed further <strong>in</strong> Section 8.1 and Appendix 7.11
The checklist at Appendix 1 provides a concise summary of the OH&S issues <strong>to</strong> beassessed and should be considered when gather<strong>in</strong>g <strong>in</strong><strong>for</strong>mation and at the <strong>in</strong>itialvisit.In some cases of severe domestic squalor, OH&S concerns may prevent serviceproviders from enter<strong>in</strong>g the premises and carry<strong>in</strong>g out a comprehensive assessment.Field <strong>staff</strong> should contact their employer’s OH&S adviser or WorkCover <strong>NSW</strong>(www.workcover.nsw.gov.au) <strong>for</strong> advice.Assess<strong>in</strong>g the level of squalorHav<strong>in</strong>g ga<strong>in</strong>ed access <strong>to</strong> the premises, it is advisable <strong>to</strong> assess whether or not theperson is <strong>liv<strong>in</strong>g</strong> <strong>in</strong> squalor. The Environmental Cleanl<strong>in</strong>ess and Clutter Scale (ECCS)at Appendix 2 provides a method <strong>to</strong> objectively assess and record observations ofvarious aspects of personal and environmental cleanl<strong>in</strong>ess.Validation and reliability data have been collected and are available from the authors(Halliday and Snowdon, manuscript <strong>in</strong> preparation). They have provided def<strong>in</strong>itionsthat allow raters <strong>to</strong> consider <strong>to</strong> what degree various aspects of the premises differfrom those that would be considered by <strong>people</strong> from all cultural and social groupsas clean and uncluttered. This does not mean <strong>to</strong> imply 'normality'. A home at the <strong>to</strong>pof a high-rise apartment block would not be normal <strong>for</strong> persons from many areas ofthe world, and the domestic environment there<strong>in</strong> might differ greatly from what thosepersons are used <strong>to</strong>. It is accepted that <strong>people</strong> vary <strong>in</strong> their subjective viewsconcern<strong>in</strong>g cleanl<strong>in</strong>ess, and these differ accord<strong>in</strong>g <strong>to</strong> circumstance and upbr<strong>in</strong>g<strong>in</strong>g.The def<strong>in</strong>itions aim <strong>to</strong> achieve consistency <strong>in</strong> rat<strong>in</strong>gs, though undoubtedly subjectivitywill affect decisions. For example, some aspects relat<strong>in</strong>g <strong>to</strong> a kitchen might suggesta rat<strong>in</strong>g of 1 (somewhat dirty; garbage ma<strong>in</strong>ly <strong>in</strong> the refuse b<strong>in</strong>) while others (e.g.mouldy food on the table) might suggest a rat<strong>in</strong>g of 3 (very dirty and unhygienic).The rater has <strong>to</strong> decide what is more important, and whether <strong>to</strong> give a compromiserat<strong>in</strong>g. Some features will always require a rat<strong>in</strong>g of 3, even if observations of otheraspects do not match the def<strong>in</strong>itions provided <strong>in</strong> the 'very dirty' column.The ECCS has 10 items, rated between 0 and 3. Where possible, all rooms shouldbe <strong>in</strong>spected be<strong>for</strong>e mak<strong>in</strong>g a rat<strong>in</strong>g. The cleaner and less cluttered the home, themore likely the score is <strong>to</strong> be 0. The maximum score <strong>for</strong> these domestic items is 30,and a rat<strong>in</strong>g of at least 20 usually means that the person lives <strong>in</strong> severe domesticsqualor. Rat<strong>in</strong>gs of less than 10 imply that although the person may need helpwith clean<strong>in</strong>g or sort<strong>in</strong>g out possessions, they do not live <strong>in</strong> severe domestic squalor.It is also relevant <strong>to</strong> consider whether they live <strong>in</strong> very cluttered surround<strong>in</strong>gs withoutbe<strong>in</strong>g markedly unclean, and this will be <strong>in</strong>dicated by rat<strong>in</strong>gs on items A and C of thescale.It must be emphasised that the rat<strong>in</strong>gs on the ECCS are ma<strong>in</strong>ly <strong>for</strong> documentationpurposes, <strong>to</strong> record what has been observed <strong>in</strong> order <strong>to</strong> relay this <strong>to</strong> others, and then<strong>to</strong> be able <strong>to</strong> rate changes <strong>in</strong> <strong>liv<strong>in</strong>g</strong> conditions over time. They give an <strong>in</strong>dication ofwhat one observer found on a particular day, and co-rat<strong>in</strong>gs so far have revealedthat different raters tend <strong>to</strong> rate similarly. However, scores do not tell raters how <strong>to</strong>respond <strong>to</strong> a particular situation. How <strong>to</strong> <strong>in</strong>tervene is determ<strong>in</strong>ed by a whole lot ofother fac<strong>to</strong>rs, not just the observed degree of domestic squalor. Supplementaryquestions allow documentation of observations concern<strong>in</strong>g personal cleanl<strong>in</strong>ess,12
availability of essential services, and the structural safety and upkeep ofthe premises.4.5 Assess<strong>in</strong>g the impact of squalor on the person, family and/orlocal communityThe impact of squalor on all relevant persons should be assessed. The checklists <strong>for</strong>this purpose are set out <strong>in</strong> sections 4.5.1 and 4.5.2 below, and these are comb<strong>in</strong>edas one checklist at Appendix 3.4.5.1 Impact of squalor on the person’s health and lifestyleThe f<strong>in</strong>d<strong>in</strong>gs of the ECCS should be summarised <strong>to</strong> identify the issues directlyrelevant <strong>to</strong> the person that need <strong>to</strong> be addressed.Consider<strong>in</strong>g the high <strong>in</strong>cidence of both mental and physical disorders associated withcases of severe domestic squalor, it may be necessary <strong>to</strong> organise a review of theperson’s health and lifestyle needs by experienced <strong>staff</strong>. The important issues <strong>to</strong> beconsidered at the <strong>in</strong>itial visit relate <strong>to</strong>:• the need <strong>for</strong> medical and/or psychiatric <strong>in</strong>tervention• the need <strong>for</strong> <strong>assist</strong>ance with activities of daily <strong>liv<strong>in</strong>g</strong>• whether the person is at risk of homelessness• the person’s decision-mak<strong>in</strong>g capacity (see Section 8.1)• whether the statu<strong>to</strong>ry powers of other agencies (council, DoCS) might overridethe wishes of the person.As a first step <strong>to</strong>wards determ<strong>in</strong><strong>in</strong>g whether further <strong>in</strong>tervention by experienced <strong>staff</strong> fromother agencies is required, the attached checklist provides a list of the fac<strong>to</strong>rs that might bereviewed and services/agencies where additional <strong>in</strong><strong>for</strong>mation may be sought.Fac<strong>to</strong>r/s Sources <strong>for</strong> further <strong>in</strong><strong>for</strong>mation 4Self-neglect with poor nutrition,Medical services (e.g., GP, homedehydration, probable untreated medical nurses, Aborig<strong>in</strong>al Medical Service)problemspsychiatric services (e.g.,community mental health team,Transcultural Mental Health)Confusion, disorientation, memoryimpairment, wander<strong>in</strong>g and gett<strong>in</strong>g lost,delirium, acute psychiatric symp<strong>to</strong>ms suchas halluc<strong>in</strong>ations, threaten<strong>in</strong>g self-harm,suicidal behaviours and symp<strong>to</strong>mssuggestive of severe depressionAggressive behaviour or threatened harm<strong>to</strong> othersMedical, psychiatric services (seeabove)Medical, psychiatric, drug andalcohol services, police4 See Appendix 10 <strong>for</strong> list of abbreviations.13
Fac<strong>to</strong>r/s Sources <strong>for</strong> further <strong>in</strong><strong>for</strong>mation 4Exposure <strong>to</strong> possible f<strong>in</strong>ancial exploitation Office of the Protectiveor abuseCommissioner, Office of the PublicGuardianThreatened eviction and at risk of becom<strong>in</strong>ghomelessLives alone and/or unable <strong>to</strong> access help orsupervision, marked decl<strong>in</strong>e <strong>in</strong> activities ofdaily <strong>liv<strong>in</strong>g</strong> and functional statusLimited mobility and risk of falls,<strong>in</strong>cont<strong>in</strong>enceUtilities not present or not functional, i.e.water, power, sewerage, heat<strong>in</strong>g,telephonesHous<strong>in</strong>g authority (DoH,landlord/real estate agent), NGOsMedical services, <strong>in</strong>take and referralsection of DADHC, ACATMedical services, DADHC, ACATLocal council, local water authority,NGOs, DoH, landlord/real estateagentOther issues that might be considered <strong>in</strong>clude:• The frequency of contact with family, friends or social supports (if any), as ameasure of the person’s safety and ability <strong>to</strong> access help or supervision should itbe required.• Feedback provided by the family and/or the general practitioner, provided theperson has given <strong>in</strong><strong>for</strong>med consent <strong>for</strong> this.• Who owns the premises and the person’s attitude <strong>to</strong>wards a clear up. This will<strong>in</strong>fluence how the clear up process is carried out and who will undertake this (seeSection 6.1).The above f<strong>in</strong>d<strong>in</strong>gs should be discussed with other services agencies <strong>in</strong>volved withthe person, always m<strong>in</strong>dful of privacy considerations (see Section 5).4.5.2 Impact of squalor on the family and/or local communityIn assess<strong>in</strong>g the impact of squalor on family members and the local community, <strong>field</strong><strong>staff</strong> may encounter issues identified below and may need <strong>to</strong> seek further <strong>in</strong><strong>for</strong>mationfrom relevant agencies listed <strong>in</strong> the table below.IssueExcessive hoard<strong>in</strong>g caus<strong>in</strong>g health and safety issues <strong>for</strong>neighbours.Compla<strong>in</strong>ts from adjo<strong>in</strong><strong>in</strong>g neighbours regard<strong>in</strong>g the mess,<strong>in</strong>vasion of space, excessive smells (from rubbish and/orsewerage), fire hazards, or verm<strong>in</strong> <strong>in</strong>festation.Presence of dependent others, eg children, elderly relatives.Pets kept <strong>in</strong> poor health.Agencies and/or services<strong>for</strong> further <strong>in</strong><strong>for</strong>mationDoH, local councilDoH, local council, someclean<strong>in</strong>g services, localwater authorityDoCS, DADHCRSPCA14
4.6 Initiate referrals <strong>to</strong> address critical needsThe need <strong>for</strong> referral <strong>to</strong> another agency is determ<strong>in</strong>ed by the apparent urgency of thesituation and the wishes of the <strong>in</strong>dividual. The person may be clearly very unwell atthe time of assessment and require urgent medical attention, or the person maypresent a relatively significant public health risk <strong>to</strong> the local community.The Local Government Act 1993 was amended <strong>in</strong> 2006 <strong>to</strong> enable councils <strong>to</strong> respondquickly and effectively <strong>to</strong> situations that occur on land used <strong>for</strong> residential purposesthat pose a threat <strong>to</strong> public or <strong>in</strong>dividual health. The amendments deal with highvolumerubbish accumulation that attracts verm<strong>in</strong> and other pests and which pose arisk <strong>to</strong> residents, neighbours and public health.In situations of extreme squalor, the assessment of risk may vary between therelevant authorities. The evaluation of the <strong>field</strong> <strong>staff</strong> may not correspond with that ofthe local council’s environmental health officer. Situations should be avoided whereone course of action is advised by <strong>field</strong> <strong>staff</strong> but another is pursued by the localcouncil (not<strong>in</strong>g that the council does not need the consent of the resident <strong>to</strong> <strong>in</strong>voke itsclean up powers). It is advisable that <strong>field</strong> <strong>staff</strong> liaise with the relevant local councilbe<strong>for</strong>e mak<strong>in</strong>g an assessment on <strong>in</strong>tervention and advis<strong>in</strong>g the resident on what willhappen. This would also allow the <strong>field</strong> <strong>staff</strong> <strong>to</strong> determ<strong>in</strong>e whether the residentialpremises are subject <strong>to</strong> an exist<strong>in</strong>g order (which may be <strong>in</strong> effect <strong>for</strong> a period of up <strong>to</strong>5 years).Interventions could also <strong>in</strong>clude contact with the landlord/real estate agent (if theperson is rent<strong>in</strong>g privately) or the DoH (if a public tenant) and other relevant agencies<strong>to</strong> ensure hous<strong>in</strong>g is res<strong>to</strong>red <strong>to</strong> a habitable standard by mak<strong>in</strong>g necessary repairs orreconnect<strong>in</strong>g amenities (e.g., runn<strong>in</strong>g water, electricity, etc.).In cases where the extent of squalor may not be extreme and there is little apparentrisk <strong>to</strong> the person, neighbours or the fabric of the build<strong>in</strong>g, <strong>in</strong>tervention does not need<strong>to</strong> be immediate, but should aim <strong>to</strong> prevent future problems aris<strong>in</strong>g.4.6.1 Medical and/or psychiatric reviewIf it is believed urgent medical attention is required, or medical review cannot bearranged at home with<strong>in</strong> a reasonable timeframe, arrange <strong>for</strong> the person <strong>to</strong> betransferred <strong>to</strong> hospital. Other medical services that should be considered <strong>in</strong>cludereferral <strong>to</strong>:• the local general practitioner• community services, <strong>in</strong>clud<strong>in</strong>g adult psychiatric services and Aged Care AssessmentTeams (ACATs)• specialist medical services.For an example of this see Case Study 2 <strong>in</strong> Appendix 8.Under the Mental Health Act 1990, <strong>people</strong> may be taken <strong>to</strong> and deta<strong>in</strong>ed <strong>in</strong> a hospitalif they are mentally ill or mentally disordered, permitt<strong>in</strong>g a brief period ofhospitalisation <strong>for</strong> further assessment and decisions regard<strong>in</strong>g ongo<strong>in</strong>g management.This Act is relevant when a person <strong>liv<strong>in</strong>g</strong> <strong>in</strong> squalor:15
• has a sign of a mental illness, such as disturbance of mood, thought disorder,sensory misperceptions or behaviour suggest<strong>in</strong>g any of these, and• is at risk of harm <strong>to</strong> themself or others.For further <strong>in</strong><strong>for</strong>mation about the provisions of the Mental Health Act 1990, see Section7.2.4.6.2 Assistance with activities of daily <strong>liv<strong>in</strong>g</strong> (ADL)If the person is at extreme risk of falls or requires urgent <strong>assist</strong>ance with personalcare, consider referr<strong>in</strong>g the person <strong>to</strong> the local ACAT and/or DADHC. Detailsregard<strong>in</strong>g these agencies are located at Appendix 5.4.6.3 Assess<strong>in</strong>g the risk on dependentsAssess<strong>in</strong>g the risk <strong>to</strong> dependent children and young <strong>people</strong> is a particularly complextask. Where there are dependent children or young <strong>people</strong> <strong>liv<strong>in</strong>g</strong> <strong>in</strong> the same dwell<strong>in</strong>gwho may be at risk of abuse or neglect, a report of risk of harm may need <strong>to</strong> be made<strong>to</strong> DoCS. The 2006 <strong>NSW</strong> Interagency <strong>Guidel<strong>in</strong>es</strong> <strong>for</strong> Child Protection Intervention(see Chapter 2, ‘Mak<strong>in</strong>g a Child Protection Report’) provides a guide <strong>to</strong> the processand requirements <strong>for</strong> the report<strong>in</strong>g of children and young <strong>people</strong>.If the dependents have a disability or there are no other suitable accommodationoptions, refer the matter <strong>to</strong> DADHC as soon as practicable.4.6.4 Relocation of petsIn cases of suspected or observed failure <strong>to</strong> provide adequate care of pets andanimals, report the matter <strong>to</strong> the Royal Society <strong>for</strong> the Protection and Care ofAnimals (RSPCA) or other animal welfare agencies.4.6.5 Organise a clear up if an urgent OH&S risk presents and theperson supports this <strong>in</strong>terventionThe options <strong>for</strong> a clean up are described <strong>in</strong> Section 6.1. These options should bediscussed with the person, bear<strong>in</strong>g <strong>in</strong> m<strong>in</strong>d that <strong>in</strong> cases where council deems therisk <strong>to</strong> be serious or the situation an emergency, council may <strong>in</strong>voke powers underamendments <strong>to</strong> the Local Government Act 1993 that override the resident’s choice.16
SECTION 5: Interagency cooperationFor the majority of cases, a number of agencies and services will be <strong>in</strong>volved <strong>in</strong>provid<strong>in</strong>g support <strong>to</strong> persons <strong>liv<strong>in</strong>g</strong> <strong>in</strong> domestic squalor. It is essential <strong>to</strong> ensure thatall service providers and agencies have a consistent approach <strong>to</strong> the person. Thiscould be arranged through a case meet<strong>in</strong>g where agencies identify their roles andresponsibilities and a case manager is appo<strong>in</strong>ted.5.1 Coord<strong>in</strong>ation of services and development of Action PlansThe pr<strong>in</strong>cipal aims of cooperation between agencies are <strong>to</strong>:• identify a key worker or case manager responsible <strong>for</strong> ongo<strong>in</strong>g liaison with theperson <strong>liv<strong>in</strong>g</strong> <strong>in</strong> squalor• report on the <strong>in</strong>itial assessment of the person and the proposed <strong>in</strong>terventions• determ<strong>in</strong>e the course of action, agreed <strong>in</strong>terventions, moni<strong>to</strong>r<strong>in</strong>g arrangementsand the <strong>in</strong>dividual’s responsible.Often the person who makes the <strong>in</strong>itial contact with the client will assume the role ofcase manager. In some cases, the person who receives the referral will contactanother agency and request that this agency assume the coord<strong>in</strong>at<strong>in</strong>g role. Theservice that conducted the <strong>in</strong>itial assessment might wish <strong>to</strong> convene a jo<strong>in</strong>t agencycase conference with representatives from the relevant services. However, it may bedifficult <strong>to</strong> coord<strong>in</strong>ate a meet<strong>in</strong>g quickly, there<strong>for</strong>e phone/e-mail communicationshould be considered as the next best option.Identify<strong>in</strong>g the <strong>in</strong>terventions required should be determ<strong>in</strong>ed through a jo<strong>in</strong>t careplann<strong>in</strong>g process, <strong>in</strong> consultation with the relevant agencies. Resource constra<strong>in</strong>tsapply <strong>to</strong> human service agencies, and there<strong>for</strong>e the resources available will need <strong>to</strong>be prioritised on a case-by-case basis.The case manager should complete a Squalor Action Plan (see Appendix 4), whichidentifies the actions <strong>to</strong> be undertaken, the person(s) responsible, and review dates.The case manager should distribute the Squalor Action Plan <strong>to</strong> all <strong>in</strong>volved agencies.This will enable coord<strong>in</strong>ation of the services <strong>to</strong> be provided.5.2 Ongo<strong>in</strong>g moni<strong>to</strong>r<strong>in</strong>gWhere clean<strong>in</strong>g of squalor is successfully completed and there is a substantialimprovement <strong>in</strong> the person’s <strong>liv<strong>in</strong>g</strong> conditions, ongo<strong>in</strong>g moni<strong>to</strong>r<strong>in</strong>g or follow-up is highlydesirable, as there is a high risk of recurrence.The service that provides ongo<strong>in</strong>g moni<strong>to</strong>r<strong>in</strong>g will be determ<strong>in</strong>ed by the follow<strong>in</strong>g:• the need <strong>for</strong> a cont<strong>in</strong>u<strong>in</strong>g role <strong>for</strong> the case worker• the nature of the <strong>in</strong>tervention required• the need <strong>for</strong> other services, such as residential support services.Ongo<strong>in</strong>g moni<strong>to</strong>r<strong>in</strong>g and follow up of the person could be provided by a number of<strong>in</strong>dividuals, <strong>in</strong>clud<strong>in</strong>g the general practitioner, mental health <strong>staff</strong>, NGOs, local council17
community officers, ACAT or DoH. An appropriate medical practitioner should provideongo<strong>in</strong>g medical care if there are chronic physical health problems or disabilities.Feedback on progress should be reported regularly <strong>to</strong> all <strong>in</strong>volved agencies.18
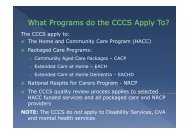
5.3 FLOWCHART 1: ASSESSMENT & SUPPORT FOR PEOPLE LIVING IN SQUALORPOSSIBLEINTERVENTIONSTAKE IMMEDIATEACTION IF REQUIRED1. For person (eg transfer<strong>to</strong> hospital)2. For dependents (egrefer <strong>to</strong> DoCS, RSPCA)Individual work& casemanagementClean<strong>in</strong>gREFERRALObta<strong>in</strong>background<strong>in</strong><strong>for</strong>mation:<strong>in</strong>clud<strong>in</strong>g potentialOH&S issuesHOME VISIT1. Assessment of- Level – squalor- Risk- Person- Dependents- Capacity2. Engage & ga<strong>in</strong> trust ofpersonJOINT AGENCY CASECONFERENCEConvene meet<strong>in</strong>g with delegates fromrelevant services <strong>to</strong> identify casemanager and determ<strong>in</strong>e action plan,with<strong>in</strong> context of;1. Person’s physical/mental health2. Person’s capacity; does the personhave impaired decision mak<strong>in</strong>g reaccommodation, services, health andor f<strong>in</strong>ancial management?3. Acceptance of <strong>assist</strong>ance.Medical &psychiatricservicesHome servicesCouncilservicesONGOING FOLLOWUP & SUPERVISIONTO PREVENTRECURRENCE.(Case management; NGOservices; CommunityTreatment Order & MentalHealth; GP)REFUSESASSESSMENTRESISTS HELPor LACKS CAPACITYDoHReal EstateAgentPEOPLE WHO RESISTASSESSMENT ORHELP(See Flowchart 2)Residential care19
SECTION 6: Organis<strong>in</strong>g referrals <strong>to</strong> relevant agenciesand service providers6.1 Clean<strong>in</strong>g upThe need <strong>to</strong> clean up the premises must be discussed with the person, <strong>to</strong> determ<strong>in</strong>ewhether the person supports the need <strong>for</strong> this <strong>to</strong> be undertaken (bear<strong>in</strong>g <strong>in</strong> m<strong>in</strong>d that<strong>in</strong> cases of extreme domestic squalor, the person’s choice may be limited oroverridden). Examples of reasons <strong>for</strong> a clean up <strong>in</strong>clude the follow<strong>in</strong>g:• Makes it possible <strong>to</strong> <strong>in</strong>vite family, friends or partners back <strong>to</strong> their home. Whilesome <strong>people</strong> who live <strong>in</strong> squalor are isolated because of personal preference,others may be lonely and desire more contact.• Reduces the risk of fall<strong>in</strong>g and reta<strong>in</strong>s <strong>in</strong>dependence. Some <strong>people</strong> will acceptthat reduc<strong>in</strong>g clutter, remov<strong>in</strong>g excessive possessions and clean<strong>in</strong>g are necessary<strong>to</strong> ma<strong>in</strong>ta<strong>in</strong> <strong>in</strong>dependence and reduce risk. Others may accept clean<strong>in</strong>g <strong>to</strong> allowthem <strong>to</strong> rema<strong>in</strong> <strong>in</strong>dependent <strong>in</strong> their own home.• S<strong>to</strong>ps a bad habit and saves money. Some <strong>people</strong> will know that their tendency<strong>to</strong> collect th<strong>in</strong>gs is out of their control and is negatively affect<strong>in</strong>g their quality of life.The offer of help can be presented as an opportunity <strong>to</strong> break a bad habit, savemoney and enjoy a more positive lifestyle.• Helps f<strong>in</strong>d a good home <strong>for</strong> some of the th<strong>in</strong>gs they have collected. People whocollect th<strong>in</strong>gs often do so because they consider these th<strong>in</strong>gs have great value. Itmay be argued that the item cannot be valued on an <strong>in</strong>dividual basis when part ofa vast collection and may be lost or damaged.• Contributes <strong>to</strong> a worthy cause. It may be possible <strong>to</strong> conv<strong>in</strong>ce the person <strong>to</strong> giveaway excess property (furniture, appliances, collectibles, <strong>for</strong> example) if it is be<strong>in</strong>gdonated <strong>to</strong> a worthy charity or cause. Emphasise the benefits of recycl<strong>in</strong>g.• Avoids further compla<strong>in</strong>ts. Sometimes <strong>people</strong> will agree <strong>to</strong> make changes just <strong>to</strong>avoid be<strong>in</strong>g hassled aga<strong>in</strong> and/or avoid prosecution, f<strong>in</strong>es or legal action. There isa particularly high likelihood of the problem recurr<strong>in</strong>g aga<strong>in</strong> <strong>in</strong> this situation, eventhough this type of client is the least likely <strong>to</strong> agree <strong>to</strong> ongo<strong>in</strong>g moni<strong>to</strong>r<strong>in</strong>g or<strong>assist</strong>ance.• Avoids the risk of cessation of services. Some services e.g., community nurses,meals on wheels, personal care and domestic <strong>assist</strong>ance may be at risk, as thecont<strong>in</strong>uation of these services is related <strong>to</strong> OH&S issues.Clean<strong>in</strong>g, rubbish removal and pest exterm<strong>in</strong>ation service providers contracted <strong>to</strong>undertake work must comply with OH&S requirements and have adequate PublicLiability Insurance and Workers Compensation cover.The local council may arrange <strong>for</strong> the removal of excess property and clearance of thegarden. Councils have powers <strong>to</strong> recover expenses <strong>in</strong>curred <strong>in</strong> carry<strong>in</strong>g out work wherethere has been a failure <strong>to</strong> comply with an Order. Options that councils may consider <strong>for</strong>recovery of the costs of clean<strong>in</strong>g <strong>in</strong>clude:• charg<strong>in</strong>g the owner or occupier of the premises (depend<strong>in</strong>g on whom the CouncilOrder was served) <strong>for</strong> the removal and disposal of waste services;20
• plac<strong>in</strong>g a lien on the property, i.e., keep the property until the debt owed is paid;• if a protected person has a F<strong>in</strong>ancial Manager, then a F<strong>in</strong>ancial ManagementOrder (see Section 8.2) could be sought <strong>to</strong> seek approval <strong>for</strong> a clean up andany necessary repairs <strong>to</strong> take place. Approval of this Order would depend onthe funds available from the person’s estate.The local council should be able <strong>to</strong> provide <strong>in</strong><strong>for</strong>mation on sub-contrac<strong>to</strong>rs andprivate cleaners who provide heavy-duty clean<strong>in</strong>g services. For further <strong>in</strong><strong>for</strong>mationabout the role of local council see Appendix 6.Some clean<strong>in</strong>g services may also be able <strong>to</strong> remove rubbish and excess propertyand arrange <strong>for</strong> tradesmen <strong>to</strong> carry out repairs and fumigate <strong>for</strong> pests. Field <strong>staff</strong>,when plann<strong>in</strong>g a clean up, need <strong>to</strong> be conscious of the costs <strong>in</strong>volved and who willpay these costs, <strong>in</strong>clud<strong>in</strong>g the person’s capacity <strong>to</strong> pay.Some NGOs may be able <strong>to</strong> <strong>assist</strong> with the costs of clean up activities themselves if theperson cannot pay. Some fund<strong>in</strong>g from Community Aged Care Packages (CACPs) maybe available <strong>for</strong> clean ups, but use of these funds <strong>for</strong> this purpose may be limited.Another program which NGOs may be able <strong>to</strong> access <strong>for</strong> <strong>people</strong> with complex needsrequir<strong>in</strong>g case management is the Community Options Program (COPS). Carel<strong>in</strong>k canprovide <strong>in</strong><strong>for</strong>mation about local Community Options project case managers locatedthroughout the State.Forensic clean<strong>in</strong>g is required where there is a concern about exposure <strong>to</strong> humanwaste, body fluids or excretions, needle stick <strong>in</strong>juries, or there is an <strong>in</strong>fection risk.Forensic cleaners have tra<strong>in</strong><strong>in</strong>g <strong>in</strong> relation <strong>to</strong> health and hygiene, and use specialisedclean<strong>in</strong>g detergents <strong>to</strong> ensure sterilisation and <strong>to</strong> remove <strong>for</strong>ensic science chemicals.They can also provide pest control fumigation when required. In some situations,government departments <strong>in</strong>clud<strong>in</strong>g police, local government, hospitals, andambulance services will provide <strong>for</strong>ensic clean<strong>in</strong>g. The cost of heavy-duty and<strong>for</strong>ensic clean<strong>in</strong>g is frequently prohibitive.Most <strong>people</strong> want <strong>to</strong> rema<strong>in</strong> <strong>in</strong> their home while it is be<strong>in</strong>g cleaned, even though this canbe very stressful. They are likely <strong>to</strong> protest at attempts <strong>to</strong> dispose of excess or damagedproperty and disused possessions. In their absence, however, subsequent allegations ofloss or theft of valuables may be made.Be<strong>for</strong>e clean<strong>in</strong>g, where possible, <strong>to</strong>gether with the person:• establish an <strong>in</strong>ven<strong>to</strong>ry of possessions• identify valuables and arrange <strong>for</strong> them <strong>to</strong> be placed securely dur<strong>in</strong>g clean<strong>in</strong>g• estimate the cost of clean<strong>in</strong>g.For a case study example, see Case Study 3 <strong>in</strong> Appendix 8.21
6.2 Service providers and agenciesServices and agencies who can support persons <strong>liv<strong>in</strong>g</strong> <strong>in</strong> domestic squalor <strong>in</strong>cludethe follow<strong>in</strong>g:• mental health services• community health services• residential care services• Aged Care Assessment Teams (ACATs)• Department of Age<strong>in</strong>g, Disability and Home Care (DADHC)• Home and Community Care (HACC) services• local government services• non-government organisations (NGOs).• Department of Hous<strong>in</strong>g (DoH)• drug and alcohol services.Details of these services are provided at Appendix 5.22
SECTION 7: Strategies <strong>to</strong> help <strong>people</strong> who are unwill<strong>in</strong>g <strong>to</strong>accept <strong>assist</strong>ance7.1 Where the person has decision-mak<strong>in</strong>g capacityWhere a person has decision-mak<strong>in</strong>g capacity but has <strong>in</strong>itially resisted help, the casemanager and others <strong>in</strong>volved should cont<strong>in</strong>ue <strong>to</strong> try <strong>to</strong> persuade the person <strong>to</strong> agree <strong>to</strong>accept <strong>assist</strong>ance. Although this can be time consum<strong>in</strong>g, voluntary <strong>in</strong>tervention is likely<strong>to</strong> be more efficient and result <strong>in</strong> a better outcome. Sometimes, <strong>people</strong> who wereopposed <strong>to</strong> <strong>in</strong>tervention at the beg<strong>in</strong>n<strong>in</strong>g will be more accept<strong>in</strong>g when they have had time<strong>to</strong> consider the potential consequences of this decision.Where there is a concern about a person’s <strong>liv<strong>in</strong>g</strong> conditions and they cannot beconv<strong>in</strong>ced <strong>to</strong> address the matter voluntarily, it may be necessary <strong>to</strong> refer the matter<strong>to</strong> agencies that have the appropriate legal authority <strong>to</strong> take further action. Theseorganisations <strong>in</strong>clude the follow<strong>in</strong>g:• local councils• Department of Hous<strong>in</strong>g (<strong>for</strong> public rental tenancies only)• <strong>NSW</strong> Fire Brigade• <strong>NSW</strong> Police.The role of these organisations <strong>in</strong> ga<strong>in</strong><strong>in</strong>g access <strong>to</strong> properties is described atAppendix 6.For examples, see Case Study 2 and Case Study 6 <strong>in</strong> Appendix 8.7.2 Where the person’s decision-mak<strong>in</strong>g capacity cannot be assessedThere may be cases where capacity cannot be assessed because the personrefuses <strong>to</strong> open the door or speak <strong>to</strong> anyone. Field <strong>staff</strong> could consider ga<strong>in</strong><strong>in</strong>g<strong>in</strong><strong>for</strong>mation or <strong>assist</strong>ance by referr<strong>in</strong>g <strong>to</strong> the follow<strong>in</strong>g:The Mental Health Act 1990The Mental Health Act 1990 is relevant when a person <strong>liv<strong>in</strong>g</strong> <strong>in</strong> squalor has signs of amental illness and is at risk of harm <strong>to</strong> self or others. The Act makes provision <strong>for</strong> thefollow<strong>in</strong>g:• Involuntary admission of a person scheduled as a mentally ill person or as amentally disordered person.• Voluntary admission at the person’s oral or written request <strong>to</strong> theSuper<strong>in</strong>tendent of the hospital.The Mental Health Act 1990 def<strong>in</strong>es a mental illness as a condition that seriouslyimpairs, either temporarily or permanently, mental function<strong>in</strong>g, and characterised byone or more of the follow<strong>in</strong>g: delusions, halluc<strong>in</strong>ations, and severe disturbance ofmood, serious thought disorder or susta<strong>in</strong>ed behaviour that is suggestive of these.Because this def<strong>in</strong>ition of mental illness is fairly narrow, it may not always be possible23
<strong>to</strong> schedule a person <strong>liv<strong>in</strong>g</strong> <strong>in</strong> severe domestic squalor under the Mental Health Act1990. Apply<strong>in</strong>g <strong>to</strong> the Guardianship Tribunal <strong>for</strong> a guardianship order may be themore appropriate course of action <strong>for</strong> <strong>people</strong> who lack cognitive capacity but are notmentally ill or mentally disordered. If the person is admitted <strong>to</strong> a hospital as amentally disordered person and not subsequently found <strong>to</strong> be mentally ill, thedetention is <strong>for</strong> a limited time.Local Government Act or Residential Tenancy ActIn cases where there is no clear evidence of a mental illness, it may be possible <strong>to</strong>compel an occupant <strong>to</strong> at least have an <strong>in</strong>spection of their property. The relevant lawis determ<strong>in</strong>ed by whether the person is rent<strong>in</strong>g their accommodation or is ahomeowner.In the case of homeowners, council can seek an order <strong>for</strong> an <strong>in</strong>spection (with Police)under the Local Government Act 1993.In the case of rental accommodation, DoH, other hous<strong>in</strong>g associations or landlordscan apply <strong>to</strong> the Consumer Trader and Tenancy Tribunal <strong>to</strong> conduct an <strong>in</strong>spection <strong>in</strong>accordance with the Residential Tenancy Act 1987.24
SECTION 8: Strategies <strong>to</strong> <strong>assist</strong> <strong>people</strong> who haveimpaired decision-mak<strong>in</strong>g capacity8.1 Decision-mak<strong>in</strong>g capacityDeterm<strong>in</strong><strong>in</strong>g a person’s decision-mak<strong>in</strong>g capacity can <strong>in</strong>volve complex issues. Whilethere are well-established legal mechanisms and government agencies whichrespond <strong>to</strong> the needs of a person who requires a substitute decision maker once ithas been determ<strong>in</strong>ed the person is <strong>in</strong>capable of mak<strong>in</strong>g a decision, there is nocomprehensive approach <strong>to</strong> assess<strong>in</strong>g or address<strong>in</strong>g the support needs of a personwhose capacity is <strong>in</strong> question. 5 If the <strong>field</strong> <strong>staff</strong> is uncerta<strong>in</strong> about the decisionmak<strong>in</strong>gcapacity of the person, they should seek advice from the GuardianshipTribunal, a GP or a psychiatrist.In some cases, a person <strong>liv<strong>in</strong>g</strong> <strong>in</strong> squalor who refuses assessment will be aware ofthe potential consequences of their decision and the risks associated with this.Although their decision <strong>to</strong> refuse assessment may be considered unwise, as long asthey can demonstrate adequate understand<strong>in</strong>g of the choices they could make, andthe consequences of these choices, then they would generally be considered <strong>to</strong> havedecision-mak<strong>in</strong>g capacity.Once it has been determ<strong>in</strong>ed that a person <strong>liv<strong>in</strong>g</strong> <strong>in</strong> severe domestic squalor lacksthe cognitive capacity <strong>to</strong> make decisions about their circumstances, such asaccommodation, health, lifestyle choices and f<strong>in</strong>ancial management, decisions mayneed <strong>to</strong> be made on their behalf. However, this approach requires carefulconsideration of the ethical pr<strong>in</strong>ciples <strong>in</strong>volved. It is important <strong>to</strong> respect the person’sau<strong>to</strong>nomy and values, while at the same time protect<strong>in</strong>g the person from furtherharm, and m<strong>in</strong>imis<strong>in</strong>g the risk of harm <strong>to</strong> others.Where the decision-mak<strong>in</strong>g capacity of the person is determ<strong>in</strong>ed <strong>to</strong> be impaired,appo<strong>in</strong>tment of a substitute decision-maker is required. This is the role of a guardian.8.2 Guardianship and F<strong>in</strong>ancial Management OrdersApply<strong>in</strong>g <strong>for</strong> guardianship or f<strong>in</strong>ancial management orders may sometimes be auseful option when there are concerns about the cognitive capacity of the person<strong>liv<strong>in</strong>g</strong> <strong>in</strong> severe domestic squalor. Appo<strong>in</strong>tment of a guardian or f<strong>in</strong>ancial manager<strong>for</strong> the person authorises someone else <strong>to</strong> make decisions <strong>for</strong> the person concerned.Most <strong>people</strong> with impaired decision-mak<strong>in</strong>g do not require a guardian, becausefamily or friends provide <strong>assist</strong>ance without the need <strong>for</strong> a legal order. In othercases, when the circumstances are such that a private guardian will not be able <strong>to</strong>achieve the best <strong>in</strong>terests of the person with a disability, particularly where no one isavailable, or there is conflict among family members, the Public Guardian may beappo<strong>in</strong>ted.See Appendix 7 <strong>for</strong> details regard<strong>in</strong>g the Guardianship Tribunal, appo<strong>in</strong>tment of aguardian and the role of the Office of the Protective Commissioner.For an example see Case Study 5 <strong>in</strong> Appendix 8.5 At<strong>to</strong>rney General’s Department of <strong>NSW</strong>, Are the rights of <strong>people</strong> whose capacity is <strong>in</strong> question be<strong>in</strong>gadequately promoted and protected: A discussion Paper, March 2006, pg. 425
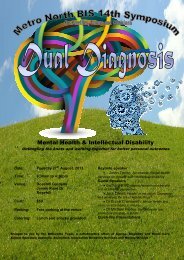
8.3 FLOWCHART 2: SUPPORT FOR PEOPLE WHO ARE UNWILLING TO ACCEPTASSISTANCEPEOPLE WHORESIST ASSESSMENTOR HELPDO THEY HAVECAPACITY?MEDICAL &PSYCHIATRICASSESSMENTKEY WORKER/CASE MANAGER<strong>to</strong> cont<strong>in</strong>ue <strong>to</strong> liaise& persuade person <strong>to</strong>accept helpApply <strong>for</strong> a guardian <strong>to</strong>be appo<strong>in</strong>ted <strong>to</strong> makedecisions about healthand services, &accommodation (<strong>in</strong>consultation with casemanager etc.)and/orUse Mental Health Act<strong>to</strong> compel treatmentApply <strong>for</strong> f<strong>in</strong>ancialmanager <strong>to</strong> beappo<strong>in</strong>tedREFER TOCOUNCILGuardian can makedecisions about<strong>in</strong>terventions<strong>in</strong>clud<strong>in</strong>g clean<strong>in</strong>gand medicaltreatmentF<strong>in</strong>ancial Manager canmake decisions aboutAccess <strong>to</strong> property,services required,clean<strong>in</strong>g and payment<strong>for</strong> clean<strong>in</strong>gNO, lackscapacity or capacity unclearYES, hascapacityDON’T KNOWCAPACITYDETERMINEDIf unsuccessful& homeownerENVIRONMENTALHEALTH OFFICER (±FIRE BRIGADE,RSPCA, POLICE)assessment of risk <strong>to</strong>neighbours & communityINTERVENTIONSie clean<strong>in</strong>g,medical treatmentCONTINUINGFOLLOWUP &SUPERVISIONTo preventrecurrence.SUBSTANTIAL RISKeg fire risk,rodents, <strong>in</strong>festationCANNOT EVEN ASSESS CAPACITY BECAUSEPERSON REFUSES TO OPEN DOOR OR SPEAK TOPEOPLEConsider;1. Mental Health Act, Section 27 Assessment (if evidenceof likely mental illness, apply <strong>to</strong> Magistrate <strong>for</strong> order <strong>to</strong>conduct assessment of patient <strong>in</strong> presence of Police)2. Council can order <strong>in</strong>spection (with Police) under LocalGovernment Act3. DoH or Landlord can apply <strong>to</strong> conduct <strong>in</strong>spection underResidential Tenancy ActDoH orLANDLORDUSE APPROPRIATELEGISLATION/AUTHORITIES<strong>to</strong> compel owner/occupant <strong>to</strong> remove risk &permit clean<strong>in</strong>gIf unsuccessful& public/privaterentalRISKuncerta<strong>in</strong>SUBSTANTIALRISKapparent26
SECTION 9: ConclusionsThe key po<strong>in</strong>ts conta<strong>in</strong>ed <strong>in</strong> these <strong>Guidel<strong>in</strong>es</strong> can be summarised as follows:• Severe domestic squalor may develop <strong>in</strong> the homes of young, middle-aged andolder <strong>people</strong>.• The perception of squalor may be affected by the cultural perspectives of both theperson and the <strong>field</strong> <strong>staff</strong>.• Language/communication and/or cultural barriers may be impediments <strong>to</strong> ga<strong>in</strong><strong>in</strong>gthe trust and cooperation of a person <strong>liv<strong>in</strong>g</strong> <strong>in</strong> squalor.• The evidence suggests that half <strong>to</strong> two-thirds of all persons <strong>liv<strong>in</strong>g</strong> <strong>in</strong> squalor sufferfrom one or more mental disorders.• When <strong>assist</strong><strong>in</strong>g <strong>people</strong> <strong>liv<strong>in</strong>g</strong> <strong>in</strong> severe domestic squalor, it is important <strong>to</strong>understand the fac<strong>to</strong>rs that have led <strong>to</strong> the squalor situation, and how <strong>to</strong> assesswhat needs <strong>to</strong> be done. Field workers need <strong>to</strong> be flexible <strong>in</strong> their approach butconscious of the statu<strong>to</strong>ry role of authorities such as the police, local council andDoCS.• The impact of squalor on the person, his/her family and the community should beassessed.• Follow<strong>in</strong>g assessment of the person <strong>liv<strong>in</strong>g</strong> <strong>in</strong> severe domestic squalor, urgent<strong>in</strong>tervention may be required. In such cases, authorities (such as local councils)may <strong>in</strong>voke powers that are contrary <strong>to</strong> a resident’s choice.• In cases where the squalor is not assessed <strong>to</strong> be extreme or of risk <strong>to</strong> the residen<strong>to</strong>r neighbours, referral <strong>to</strong> other agencies may not need <strong>to</strong> be immediate, butshould aim <strong>to</strong> prevent future problems aris<strong>in</strong>g.• Where more than one agency is <strong>in</strong>volved, <strong>in</strong><strong>for</strong>mation needs <strong>to</strong> be shared <strong>to</strong>enable a coord<strong>in</strong>ated approach. In these cases all agencies need <strong>to</strong> be m<strong>in</strong>dful ofprivacy considerations.• There is a high risk of recurrence of severe domestic squalor, even when clean<strong>in</strong>ghas been successfully completed and there is a substantial improvement <strong>to</strong> theperson’s <strong>liv<strong>in</strong>g</strong> conditions. There<strong>for</strong>e, ongo<strong>in</strong>g follow up of <strong>in</strong>volved persons ishighly recommended.27
APPENDIX 1: Occupational Health and Safety Checklist 6• Is the structure of and fabric of the build<strong>in</strong>g safe and secure? Y/N• Are the premises safe <strong>to</strong> enter (floorboards, ceil<strong>in</strong>gs)? Y/N• Are the electricity, gas and water connected? Y/N• Are there <strong>in</strong>sulated or damaged power l<strong>in</strong>es that could cause electric shock? Y/N• Are there animals on the premises? Y/N• Is there a fire hazard? Y/N• Are protective cloth<strong>in</strong>g, gloves, safety helmet, mask, safety spectacles or gogglesrequired? Y/N• Is special equipment required? Y/N• Is there a health risk? Y/N• Are there weapons or explosive materials on the premises? Y/N• Are there booby traps on private property? Y/N• Are there slip hazards because of faeces? Y/N• Are there fall hazards from climb<strong>in</strong>g over barricades Y/N• Will there be the likelihood or probability of physical attack from the occupant? Y/NNote: It would be helpful if as many as possible of the above questions can be answeredprior <strong>to</strong> the first home visit, i.e., at the po<strong>in</strong>t when referral is taken (see Section 3).6 Checklist developed from material provided by Waverley Council and the <strong>NSW</strong> RSPCA28
ENVIRONMENTAL CLEANLINESS AND CLUTTERSCALE (ECCS)To rate cleanl<strong>in</strong>ess of client’s accommodationRaters should circle the box or number that best fits their observations <strong>in</strong> relation <strong>to</strong> thedifferent items. These descriptions are meant <strong>to</strong> be <strong>in</strong>dicative but raters may decidebetween one category and another based on aspects not mentioned <strong>in</strong> the boxes.7Rater: …………………………………………………..Rater’s phone no: …………………………..Date: .….…/……../………A.B.C.ACCESSIBILITY (clutter):0 1 2 3EASY TO ENTERand move aboutdwell<strong>in</strong>g.SOMEWHAT IMPAIREDaccess but can get <strong>in</strong><strong>to</strong> allrooms.MODERATELY IMPAIREDaccess. Difficult or impossible<strong>to</strong> get <strong>in</strong><strong>to</strong> one or two roomsor areas.SEVERELY IMPAIREDaccess, e.g. obstructed frontdoor. Unable <strong>to</strong> reach most orall areas <strong>in</strong> the dwell<strong>in</strong>g.0-29% 30 <strong>to</strong> 59% 60 <strong>to</strong> 89% 90 <strong>to</strong> 100%of floor-space <strong>in</strong>accessible <strong>for</strong> use or walk<strong>in</strong>g acrossACCUMULATION OF REFUSE or GARBAGEIn general, is there evidence of excessive accumulation of garbage or refuse e.g. food waste,packag<strong>in</strong>g, plastic wrapp<strong>in</strong>g, discarded conta<strong>in</strong>ers (t<strong>in</strong>s, bottles, car<strong>to</strong>ns, bags) or other unwantedmaterial?0 1 2 3NONEA LITTLEB<strong>in</strong>s overflow<strong>in</strong>g and/or up<strong>to</strong> 10 emptied conta<strong>in</strong>ersscattered around.MODERATEGarbage and refuse litteredthroughout dwell<strong>in</strong>g.accumulated bags, boxesand/or piles of garbage thatshould have been disposed of.A LOTGarbage and food waste piledknee-high <strong>in</strong> kitchen andelsewhere. Clearly no recentattempt <strong>to</strong> remove refuse andgarbageACCUMULATION OF ITEMS OF LITTLE OBVIOUS VALUE:In general, is there evidence of accumulation of items that most <strong>people</strong> would consider are uselessor should be thrown away?0 1 2 3NONESOME ACCUMULATIONbut collected items areorganised <strong>in</strong> some way anddo not much impedemovement or preventclean<strong>in</strong>g or access <strong>to</strong>furniture and appliances.MODERATE EXCESSIVEACCUMULATIONItems cover furniture <strong>in</strong> mostareas, and have accumulatedthroughout the dwell<strong>in</strong>g sothat it would be very difficult <strong>to</strong>keep clean.PLEASE INDICATE TYPES OF ITEMS THAT HAVE BEEN ACCUMULATEDMARKEDLY EXCESSIVEACCUMULATIONItems piled at least waist-high<strong>in</strong> all or most areas. Clean<strong>in</strong>gwould be virtually impossible:most furniture and appliancesare <strong>in</strong>accessible.Newspapers, pamphlets, etc. Cloth<strong>in</strong>g Other items(what?.................................................) Electrical appliances Plastic bags full of items(If known, what items? ………….……….……….…..)7 Developed by G. Halliday and J. Snowdon (2006). This scale is based on the version devised by Snowdon (1986) whichmostly used item listed by Macmillan & Shaw (1966). Some descriptions used by Samios (1996) <strong>in</strong> her adaptation of thescale have been <strong>in</strong>cluded.29
D.CLEANLINESS of floors and carpets (exclud<strong>in</strong>g <strong>to</strong>ilet and bathroom) :0 1 2 3Acceptably clean <strong>in</strong> allrooms.MILDLY DIRTYFloors and carpets look as ifnot cleaned or swept <strong>for</strong> days.Scattered rubbish.VERY DIRTYFloors and carpets very dirty &look as if not cleaned <strong>for</strong>months.Rate 1 if only one room orsmall area affected.EXCEEDINGLY FILTHYWith rubbish or dirt throughoutdwell<strong>in</strong>g.Excrement usually merits a 3score.E.CLEANLINESS of walls and visible furniture surfaces and w<strong>in</strong>dow-sills :0 1 2 3Acceptably clean <strong>in</strong> allrooms.MILDLY DIRTYDusty or dirty surfaces. Dirtcomes off walls on damp ragor f<strong>in</strong>ger.VERY DIRTYGrime or dirt on walls.Cobwebs and other signs ofneglect. Greasy, messy, wetand/or grubby furniture.EXCEEDINGLY FILTHYWalls, furniture, surfaces areso dirty (e.g. with faeces orur<strong>in</strong>e) that rater wouldn’t want<strong>to</strong> <strong>to</strong>uch them.F.G.H.I.BATHROOM and TOILET :0 1 2 3Reasonably clean.KITCHEN and FOOD:MILDLY DIRTYUntidy, uncleaned, grubbyfloor, bas<strong>in</strong>, <strong>to</strong>ilet, walls, etc.Toilet may be unflushed.MODERATELY DIRTYLarge areas of floor, bas<strong>in</strong>,shower/bath, are dirty, withscattered rubbish, hair,cigarette ends, etc. Faecesand/or ur<strong>in</strong>e on outside of<strong>to</strong>ilet bowl.VERY DIRTY.Rubbish and/or excrement onfloor and <strong>in</strong> bath or showerand/or bas<strong>in</strong>. Uncleaned <strong>for</strong>months or years. Toilet maybe blocked and bowl full ofexcreta.0 1 2 3CleanHygienic.ODOUR:SOMEWHAT DIRTYAND UNHYGIENICCook-<strong>to</strong>p, s<strong>in</strong>k untidy andsurfaces dirty, maybe withsome spilt food. Refusema<strong>in</strong>ly <strong>in</strong> garbage b<strong>in</strong>. Foodthat could go off (e.g. meat,rema<strong>in</strong>s of meal) leftuncovered and out of fridge.Rate 1 If no food but fridgedirty.MODERATELY DIRTYAND UNHYGIENICOven, s<strong>in</strong>k, surfaces, floor aredirty, with piles of unwashedcrockery and utensils etc. B<strong>in</strong>soverflow<strong>in</strong>g. Some rotten ormouldy food. Fridge unclean.VERY DIRTYAND UNHYGIENICS<strong>in</strong>k, cook-<strong>to</strong>p, <strong>in</strong>sides of allcupboards filthy. Largeamount of refuse and garbageover surfaces and floor. Muchof the food is putrid, coveredwith mould and/or rotten, andunsafe <strong>to</strong> eat.Rate 3 if maggots seen.0 1 2 3Nil / pleasantUNPLEASANTe.g. ur<strong>in</strong>e smell, unaired.MODERATELY MALODOROUS.Bad but rater can stay<strong>in</strong> room.VERMIN (Please circle: rats, mice, cockroaches, flies, fleas, other):UNBEARABLY MALODOROUS.Rater has <strong>to</strong> leave room verysoon because of smell.0 1 2 3NoneA FEW(e.g. cockroaches)MODERATE.Visible evidence of verm<strong>in</strong> <strong>in</strong>moderate numbers e.g.dropp<strong>in</strong>gs and chewednewspapers.INFESTATION.Alive and/or dead <strong>in</strong> largenumbers.30
J.SLEEPING AREA:0 1 2 3Reasonablyclean & tidy.MILDLY UNCLEAN.Untidy. Bed unmade. Sheetsunwashed <strong>for</strong> weeks.MODERATELY DIRTY.Bed sheets unclean & sta<strong>in</strong>ed,e.g. with faeces or ur<strong>in</strong>e.Clothes and/or rubbish oversurround<strong>in</strong>g floor areas.VERY DIRTY.Mattress or sleep<strong>in</strong>g surfaceunclean or damaged. Eitherno sheets or (if present)extremely dirty bedd<strong>in</strong>g/l<strong>in</strong>en.Surround<strong>in</strong>g area filthy.Add up circled numbers <strong>to</strong> provide a TOTAL SCORE:DO YOU THINK THISPERSON IS LIVING INSQUALOR?(circle one)NOClutter (lots),not squalorYES, mildNot clutterYes, mild+ clutter (lots)YES, moderateNot clutterYes, moderate+ clutter (lots)YES, severeNot clutterYes, severe+ clutter (lots)31
SUPPLEMENTARY QUESTIONS ( <strong>to</strong> add <strong>to</strong> description but not <strong>to</strong> score )Comments or description <strong>to</strong> clarify / amplify / justify or expand upon above rat<strong>in</strong>gs:PERSONAL CLEANLINESSDescribe the cloth<strong>in</strong>g worn by the occupant and their general appearance:0 1 2 3CLEAN AND NEAT.Well cared <strong>for</strong>.UNTIDY, CRUMPLEDOne or two dirty marks and <strong>in</strong>need of a washMODERATELY DIRTYWith unpleasant odour.sta<strong>in</strong>ed cloth<strong>in</strong>g.VERY DIRTYSta<strong>in</strong>ed, <strong>to</strong>rn clothes,malodorous.Is there runn<strong>in</strong>g water <strong>in</strong> the dwell<strong>in</strong>g ? YES or NO ?Is electricity connected and work<strong>in</strong>g? YES or NO ?Can the dwell<strong>in</strong>g be locked up and made secure? YES or NO ?MAINTENANCE, UPKEEP, STRUCTUREThis rates the state of repair and upkeep by owner/landlord. If the accommodation was cleaned up asmuch as possible, <strong>to</strong> what extent would the dwell<strong>in</strong>g require pa<strong>in</strong>t<strong>in</strong>g, refurbishment, structural repairs, etcbe<strong>for</strong>e it would be reasonably habitable?0 1 2 3NONEA LITTLEM<strong>in</strong>or repairs & somepa<strong>in</strong>t<strong>in</strong>g.A FAIR AMOUNTSome structural repairs pluspa<strong>in</strong>t<strong>in</strong>g.LOTSMajor structural repairs required,and then pa<strong>in</strong>t<strong>in</strong>g.TO WHAT EXTENT DO THE LIVING CONDITIONS MAKE THE DWELLING UNSAFEOR UNHEALTHY FOR VISITORS OR OCCUPANT(S)?0 1 2 3NOT AT ALLPOSSIBLE RISKof <strong>in</strong>jury e.g. by fall<strong>in</strong>gCONSIDERABLE RISKof fire, <strong>in</strong>jury or healthproblemVERY UNSAFEThe dwell<strong>in</strong>g is so cluttered andunhealthy that <strong>people</strong> should notenter it, (except if specialists withappropriate cloth<strong>in</strong>g and equipment)and/or there is a high fire-risk.32
APPENDIX 3: Impact of Squalor ChecklistIssueRelevant Agency/ServiceExcessive hoard<strong>in</strong>g caus<strong>in</strong>g health and safety issues <strong>for</strong>neighboursCompla<strong>in</strong>ts from adjo<strong>in</strong><strong>in</strong>g neighbours regard<strong>in</strong>g themess, <strong>in</strong>vasion of space, excessive smells (from rubbishand/or sewerage), fire hazards, or verm<strong>in</strong> <strong>in</strong>festationPresence of dependent others, eg children, elderlyrelativesPets kept <strong>in</strong> poor healthDoH, local councilDoH, local council, someclean<strong>in</strong>g services, localwater authorityDoCS, DADHCRSPCAConditionRelevant Agency/ServiceSelf-neglect with poor nutrition, dehydration, probableuntreated medical problemsConfusion, disorientation, memory impairment,wander<strong>in</strong>g and gett<strong>in</strong>g lost, delirium, acute psychiatricsymp<strong>to</strong>ms such as halluc<strong>in</strong>ations, threaten<strong>in</strong>g self-harm,suicidal behaviours or symp<strong>to</strong>ms suggestive of severedepressionAggressive behaviour or threatened harm <strong>to</strong> othersExposure <strong>to</strong> possible f<strong>in</strong>ancial exploitation or abuseThreatened eviction and at risk of becom<strong>in</strong>g homelessLives alone and/or unable <strong>to</strong> access help or supervision,marked decl<strong>in</strong>e <strong>in</strong> activities of daily <strong>liv<strong>in</strong>g</strong> and functionalstatusLimited mobility and risk of falls, <strong>in</strong>cont<strong>in</strong>enceUtilities not present or not function<strong>in</strong>g, i.e. water, power,sewerage, heat<strong>in</strong>g, telephoneMedical, psychiatric servicesMedical, psychiatric servicesMedical, psychiatric, drugand alcohol services, policeOffice of the ProtectiveCommissioner, Office of thePublic Guardian, ACAT,NGOsHous<strong>in</strong>g authority (DoH,landlord/real estate agent),NGOsMedical services, DADHC,ACATMedical services, <strong>in</strong>take andreferral section of DADHC,ACATLocal council, local waterauthority, NGOs, DoH,landlord/real estate agent33
APPENDIX 4:Squalor Action PlanClient Name:Client Address:Case Manager:Employer:Referral :SourceDateInitial Visit DateIssues Identified (<strong>in</strong>clud<strong>in</strong>g Aborig<strong>in</strong>al or Torres Strait Islander background, CALD,language/communication barriers)1.2.3.4.Actions Required Agency Review DateThis Plan will be reviewed oncc34
APPENDIX 5:<strong>liv<strong>in</strong>g</strong> <strong>in</strong> severe domestic squalorServices and agencies support<strong>in</strong>g <strong>people</strong>The follow<strong>in</strong>g government and service agencies may provide <strong>assist</strong>ance <strong>to</strong> <strong>people</strong><strong>liv<strong>in</strong>g</strong> <strong>in</strong> severe domestic squalor.Local Government servicesLocal council community officers can provide <strong>assist</strong>ance by:• arrang<strong>in</strong>g referrals <strong>to</strong> appropriate health and community services• liais<strong>in</strong>g (and sometimes visit<strong>in</strong>g) with mental health, aged care, drug and alcohol,NGO or DADHC <strong>staff</strong> where appropriate• organis<strong>in</strong>g rubbish removal and clean<strong>in</strong>g of the premises• arrang<strong>in</strong>g an authorised council officer <strong>in</strong>spection, where the condition of the home orgarden substantially impacts upon neighbours and the local community, or there arepublic health concerns such as verm<strong>in</strong>, fire risk or sewerage problems.For further <strong>in</strong><strong>for</strong>mation, contact the Department of Local Government on(02) 4428 4100 (www.dlg.nsw.gov.au)<strong>NSW</strong> Health<strong>NSW</strong> Health provides acute care facilities (public hospitals), community health servicesand public health programs. In addition, it directly operates some residential andcommunity care services, and provides some longer-term hospital care through publicsec<strong>to</strong>r mental health and aged care services. Area Health Services (AHSs) provide arange of population-based aged care, mental health, drug and alcohol and rehabilitationservices, <strong>in</strong> addition <strong>to</strong> general health services. <strong>NSW</strong> Health shares responsibility with theAustralian Government Department of Health and Age<strong>in</strong>g (DoHA) <strong>for</strong> the operation ofACATs under the Aged Care Assessment Program. <strong>NSW</strong> Health also adm<strong>in</strong>isters thehealth component of the HACC Program, under which it provides community nurs<strong>in</strong>g,allied health and some day care services.Mental Health ServicesSpecialist mental health services are <strong>in</strong> place <strong>in</strong> the public sec<strong>to</strong>r and also <strong>in</strong> theprivate sec<strong>to</strong>r. AHSs provide mental health services across the age spectrum,<strong>in</strong>clud<strong>in</strong>g crisis response, assessment, <strong>in</strong>patient and community treatment,rehabilitation and support <strong>to</strong> <strong>people</strong> experienc<strong>in</strong>g mental health problems anddisorders, and their families and carers. In a number of AHSs, there are designatedSpecialist Mental Health Services <strong>for</strong> Older People that have a specialist capacity <strong>to</strong>assess, treat and manage a complex range of mental health disorders <strong>in</strong> older<strong>people</strong>, and these specialist services are currently be<strong>in</strong>g further developed across<strong>NSW</strong>.People who live <strong>in</strong> severe domestic squalor are often referred <strong>to</strong> Specialist MentalHealth Services <strong>for</strong> Older People or adult mental health services, <strong>in</strong> order <strong>to</strong> assesswhether a mental health problem may have precipitated or led <strong>to</strong> the unclean <strong>liv<strong>in</strong>g</strong>35
situation. Some <strong>people</strong> may be transferred <strong>to</strong> an <strong>in</strong>patient unit under the Mental HealthAct as mentally ill or mentally disordered, permitt<strong>in</strong>g a brief period of hospitalisation <strong>for</strong>assessment and ongo<strong>in</strong>g management.For further <strong>in</strong><strong>for</strong>mation, contact <strong>NSW</strong> Health on (02) 9391 9000 (www.health.nsw.gov.au)Drug and Alcohol ServicesIf substance use is identified as a component or fac<strong>to</strong>r contribut<strong>in</strong>g <strong>to</strong> a person <strong>liv<strong>in</strong>g</strong><strong>in</strong> a condition of severe domestic squalor, referral <strong>to</strong> specialist drug health servicesmay be appropriate. Explor<strong>in</strong>g treatment options when <strong>people</strong> are <strong>in</strong><strong>to</strong>xicated is notrecommended, as they are not able <strong>to</strong> make an <strong>in</strong><strong>for</strong>med choice. A small number of<strong>people</strong> may be admitted <strong>in</strong>voluntarily under the Mental Health Act. 1990. However,engag<strong>in</strong>g <strong>people</strong> <strong>in</strong> treatment services requires motivation and commitment, as drugand alcohol services are not provided on a compulsory basis. Substance abuse canimpact on broader relationship issues <strong>in</strong>volv<strong>in</strong>g family or friends, and referrals <strong>for</strong>counsell<strong>in</strong>g and/or advice <strong>for</strong> significant others may <strong>assist</strong>.Drug and alcohol services provide a range of <strong>in</strong>terventions, which may <strong>in</strong>clude:• counsell<strong>in</strong>g, <strong>in</strong>patient and outpatient de<strong>to</strong>xification• Magistrates Early Referral <strong>in</strong><strong>to</strong> Treatment program (MERIT)• pharmacotherapies <strong>for</strong> drug and alcohol dependence• residential rehabilitation• services <strong>for</strong> <strong>in</strong>ject<strong>in</strong>g drug users <strong>in</strong>clud<strong>in</strong>g clean equipment, specialist medicalconsultations and telephone consultancy.For further <strong>in</strong><strong>for</strong>mation contact the Area Health Service Drug and Alcohol Services on1300 889 788.Alcohol and Drug In<strong>for</strong>mation Service (ADIS)Offers a 24-hours, 7-day-a-week confidential telephone <strong>in</strong><strong>for</strong>mation, advice andcounsell<strong>in</strong>g service <strong>for</strong> <strong>people</strong> with problems related <strong>to</strong> drugs and alcohol.Phone (02) 9361 8000 or 1800 422 599 (<strong>for</strong> callers outside Sydney)(wwwsvh.stv<strong>in</strong>cents.com.au/drugandalc.htm)Hospitalisation and Residential CareIn some cases, depend<strong>in</strong>g upon diagnosis and the level of risk, hospitalisation or transfer<strong>to</strong> alternative accommodation, such as residential care, may be required, e.g., where<strong>in</strong>dividuals have severe medical and psychiatric problems or disabilities, such asmoderate <strong>to</strong> severe dementia or stroke-related immobility, sensory deficits and<strong>in</strong>cont<strong>in</strong>ence.If available, a brief period of hospitalisation or respite residential care can provide idealtemporary accommodation while clean<strong>in</strong>g is be<strong>in</strong>g carried out. Respite residential caremay also provide some <strong>people</strong> with an opportunity <strong>to</strong> become familiar with alternative<strong>liv<strong>in</strong>g</strong> arrangements and the benefits of the <strong>in</strong>creased support provided <strong>in</strong> supervisedaccommodation. The person’s GP would arrange <strong>for</strong> transfer <strong>to</strong> hospital. ACAT approvalmust be obta<strong>in</strong>ed <strong>for</strong> transfer <strong>to</strong> residential care.36
Aged Care Assessment Teams (ACATs)Aged Care Assessment Teams (ACATs) comprehensively assess the needs of frail older<strong>people</strong> and <strong>assist</strong> them and their carers <strong>to</strong> access available care services appropriate <strong>to</strong>their needs. ACATs provide <strong>in</strong><strong>for</strong>mation on suitable care options, and can help arrangeaccess or referral <strong>to</strong> appropriate residential or community care services such as Homeand Community Care (HACC). ACAT assessment and approval is required be<strong>for</strong>e <strong>people</strong>can access residential aged care, Community Aged Care Packages (CACPs) orExtended Aged Care at Home (EACH) Packages.ACATs provide a range of assessments, <strong>in</strong>clud<strong>in</strong>g:• the duration and severity of domestic squalor• whether the person has dementia or other health issues• how the person is manag<strong>in</strong>g f<strong>in</strong>ancially• whether the person is at risk of abuse.Other ACAT services <strong>in</strong>clude:• negotiat<strong>in</strong>g with family/friends and offer<strong>in</strong>g appropriate support• organis<strong>in</strong>g clean<strong>in</strong>g.For further <strong>in</strong><strong>for</strong>mation contact:• Commonwealth Carel<strong>in</strong>k Centre 1800 052 222 (www.commcarel<strong>in</strong>k.health.gov.au)• Local Aged Care Assessment Teams (ACAT) through the local Area Health Service• Aged and Community Care In<strong>for</strong>mation L<strong>in</strong>e 1800 500 853 (www.seniors.gov.au).Department of Hous<strong>in</strong>g (DoH)The <strong>NSW</strong> Department of Hous<strong>in</strong>g (DoH) provides hous<strong>in</strong>g services <strong>to</strong> <strong>people</strong> of<strong>NSW</strong>, and supports its tenants <strong>to</strong> live safely and <strong>in</strong> harmony with neighbours. Itassumes the responsibilities of a landlord under the Residential Tenancy Act 1987and will <strong>in</strong>tervene and <strong>in</strong>vestigate allegations of extreme hoard<strong>in</strong>g and uncleanconditions where these are breaches of the Tenancy Agreement that the Departmenthas with its tenants.The Department will make every ef<strong>for</strong>t <strong>to</strong> salvage tenancies where unacceptable,unclean or hoard<strong>in</strong>g behaviours are evident by support<strong>in</strong>g and referr<strong>in</strong>g clients.These ef<strong>for</strong>ts will be balanced aga<strong>in</strong>st threats <strong>to</strong> tenant safety and the rights ofneighbours <strong>to</strong> have reasonable peace, com<strong>for</strong>t and privacy, and <strong>to</strong> live <strong>in</strong> a healthyenvironment.The Department’s responsibilities <strong>in</strong>clude the moni<strong>to</strong>r<strong>in</strong>g of Tenancy Agreementsand:• ensur<strong>in</strong>g that tenants do not <strong>in</strong>terfere with the reasonable peace com<strong>for</strong>t orprivacy of neighbours• ensur<strong>in</strong>g that tenants are aware of the agency supports available <strong>to</strong> them <strong>to</strong>reduce their exposure <strong>to</strong> at-risk situations37
• report<strong>in</strong>g <strong>in</strong>cidents or <strong>liv<strong>in</strong>g</strong> conditions where a child is considered at risk due<strong>to</strong> neglect or unhealthy <strong>liv<strong>in</strong>g</strong> conditions• implement<strong>in</strong>g responsible property management strategies that ensuresusta<strong>in</strong>ability of public hous<strong>in</strong>g s<strong>to</strong>ck• ma<strong>in</strong>ta<strong>in</strong><strong>in</strong>g a partnership approach with other human service agencies <strong>to</strong>support and <strong>assist</strong> tenants experienc<strong>in</strong>g difficulties• provid<strong>in</strong>g Client Service visits <strong>to</strong> tenants at risk of or with a his<strong>to</strong>ry of <strong>liv<strong>in</strong>g</strong> <strong>in</strong>severe domestic squalor• DoH employs Client Service Officers (CSOs), and Specialist Client ServiceOfficers (SCSOs) who provide specialist <strong>assist</strong>ance <strong>to</strong> clients with complex orhigh support needs. These <strong>staff</strong> can work closely with other agencies <strong>in</strong>develop<strong>in</strong>g an approach <strong>to</strong> the management of extreme hoard<strong>in</strong>g or uncleanbehaviours, and <strong>in</strong> some cases provide an early <strong>in</strong>tervention role <strong>in</strong> identify<strong>in</strong>grisk behaviours of DoH tenants.• Where tenants refuse supports and their behaviours are <strong>in</strong> breach of theirTenancy Agreement, action may be taken through the Consumer Traders andTenancy Tribunal (CTTT) <strong>to</strong> ga<strong>in</strong> access <strong>to</strong> premises or <strong>to</strong> ratify SpecificPer<strong>for</strong>mance Orders.<strong>NSW</strong> Office of Community Hous<strong>in</strong>gThe Office of Community Hous<strong>in</strong>g is a bus<strong>in</strong>ess unit of the Department of Hous<strong>in</strong>gthat develops and manages the community hous<strong>in</strong>g sec<strong>to</strong>r <strong>in</strong> <strong>NSW</strong>. The sec<strong>to</strong>r iscomprised of hous<strong>in</strong>g associations, co-operatives and churches, local governmentand other community organisations with properties <strong>for</strong> long-term hous<strong>in</strong>g <strong>for</strong> low<strong>in</strong>comehouseholds as well as crisis and medium term accommodation.Orders available <strong>to</strong> the DoH through the Consumer Traders and Tenancy Tribunalare not as a matter of course available <strong>to</strong> the properties managed by organisationsfunded by the Office of Community Hous<strong>in</strong>g. However, Access Orders can beobta<strong>in</strong>ed by the Office of Community Hous<strong>in</strong>g <strong>to</strong> per<strong>for</strong>m <strong>in</strong>spections <strong>to</strong> determ<strong>in</strong>ewhether a breach of the Agreement has occurred because of property neglect.<strong>NSW</strong> Aborig<strong>in</strong>al Hous<strong>in</strong>g OfficeThe Department of Hous<strong>in</strong>g manages properties and tenancies on behalf of theAborig<strong>in</strong>al Hous<strong>in</strong>g Office (AHO) <strong>for</strong> Aborig<strong>in</strong>al & Torres Strait Islander clients.Under the Service Agreement, there is the need <strong>for</strong> the Department of Hous<strong>in</strong>g <strong>to</strong>seek approval from the AHO <strong>in</strong> matters relat<strong>in</strong>g <strong>to</strong> ma<strong>in</strong>tenance and repairs of AHOproperties. For further <strong>in</strong><strong>for</strong>mation on the AHO please contact your local Departmen<strong>to</strong>f Hous<strong>in</strong>g office.For further <strong>in</strong><strong>for</strong>mation, contact the Department of Hous<strong>in</strong>g (<strong>NSW</strong>) 1800 629 212(www.hous<strong>in</strong>g.nsw.gov.au)38
Department of Age<strong>in</strong>g, Disability and Home Care (DADHC)The Department of Age<strong>in</strong>g, Disability and Home Care (DADHC) is responsible <strong>for</strong><strong>assist</strong><strong>in</strong>g older <strong>people</strong> and <strong>people</strong> with a disability <strong>to</strong> participate fully <strong>in</strong> community life, <strong>in</strong>order <strong>to</strong> improve their quality of life. The Department provides a range of services <strong>to</strong> frailaged <strong>people</strong> and younger <strong>people</strong> with a disability, under the Home and Community Care(HACC) and the Disability Services Programs (DSP).• Under the HACC Program, the Department provides <strong>assist</strong>ance <strong>to</strong> older <strong>people</strong>,<strong>people</strong> with a disability and their carers with domestic help, and personal care. Otherservices funded under the HACC Program <strong>in</strong>clude social support, food services,community transport, dementia moni<strong>to</strong>r<strong>in</strong>g, respite and day centre services.• HACC Community Options (COPS) services provide case management <strong>for</strong> <strong>people</strong>requir<strong>in</strong>g multiple <strong>in</strong>terventions. Its brokerage funds can facilitate <strong>in</strong>terventions <strong>in</strong>support of those unable <strong>to</strong> ma<strong>in</strong>ta<strong>in</strong> adequate care of themselves or theiraccommodation.• Under the Disability Service Program (DSP), the Department funds services thatprovide <strong>people</strong> with a disability with opportunities <strong>to</strong> participate <strong>in</strong> community life.Services <strong>in</strong>clude accommodation, respite, community support, behaviour<strong>in</strong>terventions and day programs.• Both Programs provide services <strong>for</strong> <strong>people</strong> from non-English speak<strong>in</strong>g backgroundsand Aborig<strong>in</strong>al <strong>people</strong> through a range of <strong>in</strong>itiatives that recognise the cultural andl<strong>in</strong>guistic diversity of these groups.• The provision of service is dependent on the person’s assessed need, the availabilityof fund<strong>in</strong>g and the capacity of services <strong>to</strong> provide the services required.For further <strong>in</strong><strong>for</strong>mation, contact DADHC on (02) 8270 2000 (www.dadhc.nsw.gov.au)Home and Community Care (HACC) support servicesTarget population <strong>for</strong> HACC services <strong>in</strong>clude <strong>people</strong> who are frail aged, <strong>people</strong> withdisabilities and carers of these two groups. Services that can be provided through HACCfund<strong>in</strong>g <strong>in</strong>clude:Personal care services, which may <strong>in</strong>volve one or more of the follow<strong>in</strong>g:• <strong>assist</strong>ance with (or supervision of) bath<strong>in</strong>g, shower<strong>in</strong>g or spong<strong>in</strong>g, dress<strong>in</strong>g andundress<strong>in</strong>g• <strong>assist</strong>ance with shav<strong>in</strong>g, hair care and groom<strong>in</strong>g and limited nail care• <strong>assist</strong>ance with mobility such as <strong>to</strong> sit up, <strong>to</strong> turn, <strong>to</strong> stand and walk, <strong>to</strong> sit, <strong>to</strong> transfer<strong>to</strong> commode, wheelchair, chair or vehicle• <strong>assist</strong>ance with <strong>to</strong>ilet<strong>in</strong>g• <strong>assist</strong>ance with prescribed exercise or therapy programme• <strong>assist</strong>ance with fitt<strong>in</strong>g and use of appliances such as spl<strong>in</strong>ts and callipers or hoists• <strong>assist</strong>ance with hear<strong>in</strong>g aids and communication devices• moni<strong>to</strong>r<strong>in</strong>g self medication.39
Domestic <strong>assist</strong>ance services <strong>in</strong>clud<strong>in</strong>g:• Essential clean<strong>in</strong>g of house areas regularly used by the service user, such asbathrooms, <strong>to</strong>ilets, kitchens, laundries, <strong>liv<strong>in</strong>g</strong> areas and bedrooms. Workers undertaketasks such as clean<strong>in</strong>g s<strong>to</strong>ves, bench <strong>to</strong>ps and fridges as well as mopp<strong>in</strong>g orvacuum<strong>in</strong>g floors, dust<strong>in</strong>g, dishwash<strong>in</strong>g, chang<strong>in</strong>g bed l<strong>in</strong>en, wash<strong>in</strong>g, dry<strong>in</strong>g anddo<strong>in</strong>g essential iron<strong>in</strong>g.• The provision of a range of services <strong>to</strong> meet the support needs of service users.Workers can <strong>assist</strong> with meal preparation, and where this is not the primary purposeof the occasion of service, do shopp<strong>in</strong>g, undertake small errands and pay bills onbehalf of the client as required.• In remote areas service may <strong>in</strong>clude activities such as the collection of firewood.Nurs<strong>in</strong>g care, referr<strong>in</strong>g <strong>to</strong> professional nurs<strong>in</strong>g care provided by a registered or enrollednurse and services may <strong>in</strong>clude:• Teach<strong>in</strong>g <strong>in</strong>dividuals and carers how best <strong>to</strong> manage their daily care• Provid<strong>in</strong>g <strong>in</strong><strong>for</strong>mation on general health care and other community support servicesavailable, and giv<strong>in</strong>g advice on the management of particular health problems, suchas diabetes and <strong>in</strong>cont<strong>in</strong>ence• Cl<strong>in</strong>ical assessment• Direct cl<strong>in</strong>ical nurs<strong>in</strong>g• Personal care <strong>for</strong> consumers where provision by a nurse is required due <strong>to</strong> particularhealth conditions, or unstable health and/or complex needs• Supervision and tra<strong>in</strong><strong>in</strong>g of health aides and personal care workers provid<strong>in</strong>g directcare• Provision of health <strong>in</strong><strong>for</strong>mation and education• The coord<strong>in</strong>ation of home health care services and moni<strong>to</strong>r<strong>in</strong>g of an <strong>in</strong>dividual’shealth status and/or care plan.Meals, referr<strong>in</strong>g <strong>to</strong> the preparation and cook<strong>in</strong>g of food items that contributes <strong>to</strong> meet<strong>in</strong>g aclient’s daily nutrition requirements. Services <strong>in</strong>clude:• Provision of a range of meal types. The meal may be delivered <strong>to</strong> the place where aclient lives or be provided <strong>in</strong> a group environment such as centre-based day care orcommunity restaurant.• Assistance with eat<strong>in</strong>g and dr<strong>in</strong>k<strong>in</strong>g.• Ensur<strong>in</strong>g access, wherever possible, <strong>to</strong> a range and choice of different meal types<strong>in</strong>clud<strong>in</strong>g culturally appropriate meals.• Assistance with the preparation and cook<strong>in</strong>g of food and provid<strong>in</strong>g advice aboutnutrition, menus and special diets and <strong>assist</strong>ance with food shopp<strong>in</strong>g and s<strong>to</strong>rage.Transport, referr<strong>in</strong>g <strong>to</strong> provid<strong>in</strong>g transport or <strong>assist</strong><strong>in</strong>g an <strong>in</strong>dividual <strong>to</strong> use private, publicor community transport.For further <strong>in</strong><strong>for</strong>mation, contact DADHC on (02) 8270 2000 (www.dadhc.nsw.gov.au)40
Department of Community Services (DoCS)The Department of Community Services (DoCS) is responsible <strong>for</strong> the protection ofchildren and young <strong>people</strong> who are considered <strong>to</strong> be at risk of harm. To report suspectedabuse or neglect of children or young <strong>people</strong> call 13 2111. DoCS Helpl<strong>in</strong>e operates 24hours a day, seven days a week. You can r<strong>in</strong>g state-wide <strong>for</strong> the cost of a local call(www.community.nsw.gov.au)Phone:13 3627 <strong>for</strong> manda<strong>to</strong>ry reporter.13 2111 <strong>for</strong> non-manda<strong>to</strong>ry reporters.For def<strong>in</strong>itions of ‘manda<strong>to</strong>ry’ and ‘non-manda<strong>to</strong>ry’ reporter, and the circumstancesunder which phone report<strong>in</strong>g is preferred, please consult Chapter 2 of the 2006 <strong>NSW</strong>Interagency <strong>Guidel<strong>in</strong>es</strong> <strong>for</strong> Child Protection Interventions.Royal Society <strong>for</strong> the Protection and Care of Animals (RSPCA)The RSPCA can enter and <strong>in</strong>spect homes where they have received notification ofsuspected neglect or hoard<strong>in</strong>g of animals.For further <strong>in</strong><strong>for</strong>mation contact the RSPCA on 9770 7555 (www.rspcansw.org.au)Non-government organisations (NGOs)The non-government (NGOs) sec<strong>to</strong>r, <strong>in</strong>clud<strong>in</strong>g agencies such as Mercy Arms, LucanCare, the Benevolent Society, the Brown Sisters, (which are all Sydney-based), have afocus on respond<strong>in</strong>g <strong>to</strong> clients’ immediate needs, as opposed <strong>to</strong> address<strong>in</strong>g the squalorissue. The capacity of an <strong>in</strong>dividual NGO <strong>to</strong> provide a service would depend on availablefund<strong>in</strong>g and resources.Some NGOs adm<strong>in</strong>ister Community Aged Care Packages (CACPs), funded by theCommonwealth Department of Health and Age<strong>in</strong>g, that are particularly important <strong>for</strong> theongo<strong>in</strong>g management of older <strong>people</strong> who have lived <strong>in</strong> squalor. CACPs offer analternative <strong>to</strong> residential care and can bridge the gap between hous<strong>in</strong>g and governmentcare services. NGOs may be able <strong>to</strong> access services under the Community OptionsProgram (COPS) when the person <strong>liv<strong>in</strong>g</strong> <strong>in</strong> squalor is aged under 65.NGOs provide the required services directly, or purchase them from other public orprivate agencies. They offer flexible solutions <strong>to</strong> meet <strong>in</strong>dividual needs. NGOs can alsoprovide follow-up moni<strong>to</strong>r<strong>in</strong>g and support after secure accommodation has been atta<strong>in</strong>ed.Care options may <strong>in</strong>clude:• transitional hous<strong>in</strong>g• personal care and clean ups• housework and shopp<strong>in</strong>g• delivered meals, or meal preparation• case management41
• <strong>assist</strong>ance with medication and therapy• home ma<strong>in</strong>tenance• l<strong>in</strong>ks <strong>to</strong> community supports (activity centres, transport),• social activities and <strong>liv<strong>in</strong>g</strong> skill programs.For further <strong>in</strong><strong>for</strong>mation regard<strong>in</strong>g contact details <strong>for</strong> selected NGOs see Appendix 9.42
APPENDIX 6:Organisations that can <strong>assist</strong> when<strong>people</strong> are unwill<strong>in</strong>g <strong>to</strong> accept <strong>assist</strong>anceLocal CouncilsUnder the Local Government Act 1993, the local council may conduct <strong>in</strong>spections ofresidential premises, and order removal and disposal of waste, under certa<strong>in</strong>circumstances. If the person is known <strong>to</strong> other services such as mental health, agedcare, drug and alcohol or a non-government organisation (NGOs), it is beneficial <strong>to</strong> havethe health or welfare worker accompany the council <strong>staff</strong> at the time of <strong>in</strong>spection.If required, council officers may order clean<strong>in</strong>g, removal of property and repairs, undercerta<strong>in</strong> circumstances. A council is authorised <strong>to</strong> recover the reasonable costs of theentry or <strong>in</strong>spection and the clean up work.If council officers are concerned about fire safety, they may <strong>in</strong>vite Fire Brigade officers <strong>to</strong>attend dur<strong>in</strong>g the <strong>in</strong>spection.Councils are generally not permitted <strong>to</strong> unilaterally enter a property and remove materialwithout first giv<strong>in</strong>g notice of their <strong>in</strong>tention <strong>to</strong> do so. However, entry without notice ispermitted <strong>in</strong> circumstances where there is a reasonable likelihood of serious risk <strong>to</strong> healthand safety. Whenever possible, an <strong>in</strong>dependent advocate such as a family member orneighbour should be present <strong>to</strong> record the items removed from the premises.<strong>NSW</strong> Department of Hous<strong>in</strong>g (DoH)<strong>NSW</strong> Department of Hous<strong>in</strong>g (DOH) has responsibilities under provisions of theResidential Tenancy Agreement <strong>to</strong> moni<strong>to</strong>r public rental tenancies, and ensure thattenants keep premises reasonably clean, do not cause a nuisance, and do not<strong>in</strong>terfere with the reasonable peace, privacy and com<strong>for</strong>t of their neighbours.Where extreme tenant hoard<strong>in</strong>g or unclean behaviours creates a public health orsafety risk (such as fire risks), then engagement with the tenants will occur <strong>in</strong> anegotiated way by us<strong>in</strong>g techniques such as discussions on the safety, aesthetic andaccess implications. Advice could be provided on techniques <strong>for</strong> break<strong>in</strong>g downlarger tasks <strong>in</strong><strong>to</strong> more manageable smaller ones, and choos<strong>in</strong>g target areas whereprogress is more easily apparent and thus more reward<strong>in</strong>g. The Department’s <strong>staff</strong>will attempt <strong>to</strong> build rapport and endeavour <strong>to</strong> use a sympathetic and collaborativeapproach with the client on the issues.However, if a tenant is unwill<strong>in</strong>g <strong>to</strong> accept supports or alter their behaviours throughconsultative approaches, and a breach of their Tenancy Agreement is evident, thenan approach <strong>to</strong> the Consumer Trader and Tenancy Tribunal (CTTT) may be made.This could result <strong>in</strong> orders that:• Create <strong>for</strong>mally ratified agreements on acceptable behaviours of the tenant.The agreement content may be developed <strong>in</strong> conjunction with other agenciesand be <strong>in</strong>tended <strong>to</strong> support longer-term changes <strong>for</strong> the client.43
• Manda<strong>to</strong>ry access orders <strong>for</strong> Department of Hous<strong>in</strong>g <strong>staff</strong>. Such a DoH visitmay <strong>in</strong>volve a locksmith <strong>to</strong> ga<strong>in</strong> entry, and are an opportunity <strong>for</strong> a coord<strong>in</strong>atedagency approach with the <strong>in</strong>volvement of other agencyprofessionals will<strong>in</strong>g <strong>to</strong> provide assessments.Orders available <strong>to</strong> public hous<strong>in</strong>g through the CTTT are not as a matter of courseavailable <strong>to</strong> the properties managed by organisations funded by the Office ofCommunity Hous<strong>in</strong>g. However, Access Orders can be obta<strong>in</strong>ed by the Office ofCommunity Hous<strong>in</strong>g <strong>to</strong> per<strong>for</strong>m <strong>in</strong>spections <strong>to</strong> determ<strong>in</strong>e whether a breach of theAgreement has occurred because of property neglect.In addition, there are major strategic level policy <strong>in</strong>itiatives, led by DoH, <strong>in</strong>tended <strong>to</strong><strong>in</strong>crease the quality of service <strong>to</strong> social hous<strong>in</strong>g tenants with mental health issues.Jo<strong>in</strong>t Guarantee of ServiceThe Jo<strong>in</strong>t Guarantee of Service (JGOS) supports local <strong>for</strong>ums <strong>for</strong> the co-ord<strong>in</strong>ation ofdelivery of services <strong>to</strong> <strong>people</strong> <strong>liv<strong>in</strong>g</strong> <strong>in</strong> social hous<strong>in</strong>g that have mental healthproblems and disorders with ongo<strong>in</strong>g support needs. For further <strong>in</strong><strong>for</strong>mation onJGOS <strong>in</strong> your region, please contact your local DoH office.<strong>NSW</strong> Hous<strong>in</strong>g and Human Services Accord (the Accord)The Accord establishes a partnership approach across <strong>NSW</strong> Government humanservices <strong>for</strong> the provision of hous<strong>in</strong>g, health, welfare and other social supportservices. The Accord’s aim is <strong>to</strong> ensure the most vulnerable and disadvantaged <strong>in</strong>our community receive reliable hous<strong>in</strong>g and support services, reduc<strong>in</strong>g the need <strong>for</strong>crisis <strong>in</strong>tervention. The Accord sets out service pr<strong>in</strong>ciples, agency roles andcommitments <strong>to</strong> plan <strong>for</strong> specific agreements regard<strong>in</strong>g client groups.<strong>NSW</strong> Fire Brigade<strong>NSW</strong> Fire Brigade has the right <strong>to</strong> enter build<strong>in</strong>gs where it is believed that there is a fire,or where it is believed that a fire has occurred. They can take possession of the build<strong>in</strong>gand can take any procedures <strong>to</strong> render the situation safe. However, the Fire Brigadecannot <strong>in</strong>spect residential premises, even if they suspect them <strong>to</strong> be a fire hazard,without permission.The <strong>NSW</strong> Fire Brigade does not have official procedures <strong>for</strong> deal<strong>in</strong>g with a squalorsituation. This means that it is up <strong>to</strong> the <strong>in</strong>dividual officer <strong>to</strong> determ<strong>in</strong>e action <strong>to</strong> mitigatethe problem. From 1 May, 2006 it became compulsory <strong>for</strong> all residential accommodation<strong>in</strong> <strong>NSW</strong> <strong>to</strong> have al least one work<strong>in</strong>g smoke alarm.44
<strong>NSW</strong> PoliceThe Police are often the <strong>in</strong>itial po<strong>in</strong>t of contact and the referr<strong>in</strong>g body. They are asked <strong>to</strong>check on an <strong>in</strong>dividual when neighbours are concerned that mail is not be<strong>in</strong>g collected, ora person has not been seen <strong>for</strong> some time.The <strong>NSW</strong> Police service is empowered <strong>to</strong> conduct checks on <strong>people</strong>, and can use PoliceRescue <strong>to</strong> ga<strong>in</strong> access, <strong>in</strong>volv<strong>in</strong>g <strong>for</strong>ced entry if necessary. There are however, somerestrictions on their powers of entry.Police work <strong>in</strong> collaboration with <strong>NSW</strong> Mental Health services, particularly when deal<strong>in</strong>gwith mental health crisis <strong>in</strong>terventions. Police have the responsibility <strong>to</strong> protect the safetyof all parties, and <strong>to</strong> protect all persons from <strong>in</strong>jury or death, while attempt<strong>in</strong>g <strong>to</strong> preservethe rights and freedom of <strong>in</strong>dividuals.45
APPENDIX 7:decision-mak<strong>in</strong>g capacitySupports <strong>for</strong> <strong>people</strong> with impairedRole and procedures of the Guardianship TribunalThe Guardianship Tribunal is a legal body that exercises quasi-judicial powers. Its ma<strong>in</strong>role is <strong>to</strong> appo<strong>in</strong>t guardians and/or f<strong>in</strong>ancial managers <strong>for</strong> <strong>people</strong> with decision-mak<strong>in</strong>gdisabilities. It can also consent <strong>to</strong> medical treatment <strong>for</strong> adults who lack capacity <strong>to</strong> givetheir own consent.Anyone with a genu<strong>in</strong>e concern <strong>for</strong> the welfare of the person may make anapplication <strong>to</strong> the Guardianship Tribunal <strong>to</strong> have a guardian or f<strong>in</strong>ancial managerappo<strong>in</strong>ted <strong>for</strong> the person.On receipt of an application by the Guardianship Tribunal, the matter is allocated <strong>to</strong> aCoord<strong>in</strong>ation and Investigation Officer who liaises with the applicant, makes enquiriesabout the application and arranges a hear<strong>in</strong>g date.If an application is made <strong>for</strong> guardianship or f<strong>in</strong>ancial management, then the personconcerned must be supplied with a copy of the application, and has the right <strong>to</strong> come<strong>to</strong> the hear<strong>in</strong>g and express their views about the application.Guardianship Tribunal hear<strong>in</strong>gs are conducted as <strong>in</strong><strong>for</strong>mally as possible. TheTribunal usually requires two medical or professional reports address<strong>in</strong>g the issue ofcapacity be<strong>for</strong>e it can make an order. The Tribunal also considers any written or oralevidence provided by professionals, family, friends and neighbours.The Tribunal does not conduct assessments and does not have the power <strong>to</strong> compela person <strong>to</strong> co-operate with assessments aga<strong>in</strong>st their wishes.The Tribunal has a free telephone enquiries service on (02) 9555 8500 (<strong>to</strong>ll free 1800463 928), which provides <strong>in</strong><strong>for</strong>mation and advice about whether it is appropriate <strong>for</strong>an application <strong>to</strong> be made <strong>for</strong> guardianship and f<strong>in</strong>ancial management orders.Be<strong>for</strong>e mak<strong>in</strong>g an application <strong>for</strong> a person <strong>liv<strong>in</strong>g</strong> <strong>in</strong> severe domestic squalor, it isworthwhile first discuss<strong>in</strong>g the situation with a <strong>staff</strong> member from the Tribunal’sEnquiries service.Apply<strong>in</strong>g <strong>for</strong> a Guardianship OrderA Guardianship Order may be needed if a person <strong>liv<strong>in</strong>g</strong> <strong>in</strong> severe domestic squalorhas a disability which results <strong>in</strong> impaired judgement and reduced decision-mak<strong>in</strong>gcapacity. For example, a person may need help <strong>in</strong> mak<strong>in</strong>g decisions about their<strong>liv<strong>in</strong>g</strong> conditions and/or their accommodation.There is no need <strong>for</strong> a guardian <strong>to</strong> be appo<strong>in</strong>ted if the person or their family or friendsare able <strong>to</strong> resolve accommodation and services issues with service providers.Be<strong>for</strong>e a Guardianship Order can be made, the Tribunal must be satisfied that:1. the person concerned is ‘<strong>in</strong> need of a guardian’ with<strong>in</strong> the def<strong>in</strong>ition <strong>in</strong> Section 3 of theAct. This means that the person:46
• must have a disability with<strong>in</strong> the quite wide def<strong>in</strong>ition conta<strong>in</strong>ed <strong>in</strong> Section 3 (2),and• is wholly or partially <strong>in</strong>capable of manag<strong>in</strong>g themselves because of thatdisability.2. the person lacks the degree of <strong>in</strong>sight necessary <strong>to</strong> be able <strong>to</strong> make an <strong>in</strong><strong>for</strong>meddecision <strong>for</strong> himself/ herself, as dist<strong>in</strong>ct from hav<strong>in</strong>g the ability <strong>to</strong> express a view aboutsuch decisions3. matters cannot be resolved <strong>in</strong><strong>for</strong>mally.Guardianship orders are made <strong>for</strong> fixed periods, and are usually reviewed at the endof that period <strong>to</strong> assess if they are still required.Guardian’s PowerWhen the Tribunal makes a Guardianship Order it can appo<strong>in</strong>t a private guardian (suchas a relative or friend) or the Public Guardian, <strong>to</strong> make decisions on behalf of that person.A guardian is not a caseworker, but is a legally appo<strong>in</strong>ted substitute decision-makerresponsible <strong>for</strong> mak<strong>in</strong>g major life decisions, exclud<strong>in</strong>g decisions about money or f<strong>in</strong>ancialmatters. Guardianship Orders usually limit the scope of powers (functions) given <strong>to</strong> theappo<strong>in</strong>ted guardian.The functions given <strong>to</strong> a guardian will depend on <strong>in</strong>dividual circumstances and mightrelate <strong>to</strong> the follow<strong>in</strong>g areas:• Accommodation. Decisions as <strong>to</strong> where the person should live. The guardiancan seek <strong>to</strong> have the person under guardianship admitted <strong>to</strong> a psychiatric facility as avoluntary patient under the Mental Health Act 1990. Coercive powers of vary<strong>in</strong>gdegrees can be added <strong>to</strong> support this function.• Limited accommodation decision-mak<strong>in</strong>g. Decisions about respiteaccommodation and/or a move <strong>to</strong> a hospital <strong>for</strong> assessment purposes, withcoercive powers if need be.• Health care and medical and dental consent. Decisions about health care <strong>for</strong> aperson and <strong>to</strong> give consent <strong>to</strong> medical or dental treatment. Special power canalso be given under Section 46A of the Act <strong>for</strong> the guardian <strong>to</strong> override anyobjection of the person <strong>to</strong> medical treatment.• Services. Decisions about the provision of services <strong>to</strong> a person, which may<strong>in</strong>clude the authority <strong>to</strong> authorise such services be provided, despite the expresswishes of the person.The Public Guardian does not provide case management, organise clean<strong>in</strong>g or providedirect services, and will only act if there is strong evidence that <strong>liv<strong>in</strong>g</strong> <strong>in</strong> a state of severedomestic squalor is plac<strong>in</strong>g the person’s health or well be<strong>in</strong>g seriously at risk.For further <strong>in</strong><strong>for</strong>mation, contact the Guardianship Tribunal (02) 9555 8500 (<strong>to</strong>ll free 1800463 928) www.gt.nsw.gov, and Office of the Public Guardian (02) 9265 3184 (<strong>to</strong>ll free1800 451 510) www.lawl<strong>in</strong>k.nsw.gov.au/opg47
Role of the Office of the Protective Commissioner (OPC)The Office of the Protective Commissioner (OPC) can be appo<strong>in</strong>ted <strong>to</strong> manage aperson’s f<strong>in</strong>ances by the Supreme Court, the Mental Health Review Tribunal, theGuardianship Tribunal or a visit<strong>in</strong>g magistrate. When the Protective Commissionermakes ‘substitute decisions’ regard<strong>in</strong>g a person's f<strong>in</strong>ances, consideration is given <strong>to</strong>their overall best <strong>in</strong>terests, <strong>in</strong>clud<strong>in</strong>g their immediate and long-term needs,aspirations and family commitments. In cases of severe domestic squalor, theProtective Commissioner is only appo<strong>in</strong>ted if a person is <strong>in</strong>capable of mak<strong>in</strong>gdecisions about their f<strong>in</strong>ancial affairs.The Protective Commissioner is responsible <strong>for</strong> decisions about the follow<strong>in</strong>g:• F<strong>in</strong>ancial matters related <strong>to</strong> the property, its contents and any associated legalissues aris<strong>in</strong>g from the condition of the property.• Access <strong>to</strong> the property and payment <strong>for</strong> the costs of clean<strong>in</strong>g.The Protective Commissioner cannot make ‘substitute’ decisions about medicaltreatment, hospitalisation, home services and accommodation. If a decision is required <strong>in</strong>relation <strong>to</strong> these matters, the person would require the appo<strong>in</strong>tment of a guardian.If a person whose estate is managed by OPC refuses entry and entry is desired <strong>to</strong>undertake an <strong>in</strong>spection of the property, then an officer from OPC, <strong>in</strong> certa<strong>in</strong>circumstances, can enter, or authorise an agent <strong>to</strong> enter a property owned by a clientwithout their consent. This can be considered if such an action is <strong>in</strong> the <strong>in</strong>terests of theestate, and is required <strong>in</strong> order <strong>to</strong> exercise a function associated with the care andmanagement of the estate. Such an action would generally only occur after the OPC hassought and considered the views of the person and any significant others.In extreme cases, where vacant possession is required, OPC can <strong>for</strong>cibly remove a clientfrom their property if such an action relates <strong>to</strong> the care and management of the estate.This may require a direction from the Supreme Court.The OPC’s powers are not as clearly def<strong>in</strong>ed <strong>in</strong> situations where a person is <strong>liv<strong>in</strong>g</strong> <strong>in</strong>premises owned and occupied by someone else. It is generally not possible <strong>for</strong> OPC <strong>to</strong><strong>for</strong>ce entry <strong>in</strong><strong>to</strong> property owned and occupied by a person who does not lack capacity,even if the OPC’s client resides there.Further <strong>in</strong><strong>for</strong>mation can be obta<strong>in</strong>ed from the Guardianship Tribunal (02) 9555 8500 or<strong>to</strong>ll free 1800 463 928 (www.gt.nsw.gov.au) and from Office of the ProtectiveCommissioner 1300 360 466 (local call) or <strong>to</strong>ll free 1800 882 889(www.lawl<strong>in</strong>k.nsw.gov.au/opc)48
APPENDIX 8: Case studiesCASE 1An elderly male who has lived <strong>in</strong> the same private rental flat <strong>for</strong> morethan 10 years, was referred <strong>to</strong> a local ACAT by his GP. He receivesan aged pension and although he reliably pays rent, he spends therest of his <strong>in</strong>come on cigarettes and alcohol, leav<strong>in</strong>g no money <strong>to</strong> pay<strong>for</strong> food or medication. He has chronic smok<strong>in</strong>g-related lung disease,high blood pressure and leg ulcers but even though he uses a stick <strong>to</strong>walk and is unsteady, he goes out every day.After a recent admission <strong>to</strong> hospital with a chest <strong>in</strong>fection he wasdischarged <strong>to</strong> a nurs<strong>in</strong>g home. When his health improved, he<strong>in</strong>sisted on return<strong>in</strong>g <strong>to</strong> his home. His flat is very dirty, dark andneglected. It requires pa<strong>in</strong>t<strong>in</strong>g, has several broken w<strong>in</strong>dows and onlyone work<strong>in</strong>g power po<strong>in</strong>t. There are no carpets or floor covers.A local charity group removed a large amount of refuse be<strong>for</strong>e hereturned but quite a bit of rubbish has re-accumulated. He does notwant anyone <strong>to</strong> approach the owner about repairs <strong>in</strong> case the rent is<strong>in</strong>creased. He has been receiv<strong>in</strong>g home-delivered meals but refuses<strong>to</strong> pay the nom<strong>in</strong>al fee and they have threatened <strong>to</strong> withdraw. HomeHelp refuse <strong>to</strong> provide clean<strong>in</strong>g because of the condition of theaccommodation. Community nurses visit every second day <strong>to</strong> dressa leg ulcer.He denies dr<strong>in</strong>k<strong>in</strong>g any alcohol and has been refus<strong>in</strong>g <strong>to</strong> takeprescribed medications even when the purpose <strong>for</strong> these has beenclearly expla<strong>in</strong>ed. He is dishevelled, irritable and suspicious. Ontest<strong>in</strong>g of memory and orientation he per<strong>for</strong>ms well, however he hassignificant impairment on tests of frontal lobe function.Dur<strong>in</strong>g his recent admission <strong>to</strong> hospital, tests showed he hadabnormal liver function consistent with alcohol abuse. A bra<strong>in</strong> scanshowed changes due <strong>to</strong> stroke-related or cerebrovascular disease.His diagnosis is dementia due <strong>to</strong> alcohol and cerebrovasculardisease. He is aware his flat is ‘untidy’ but isn’t concerned anddoesn’t want <strong>to</strong> consider alternative accommodation.DiscussionThis man’s neglected and unclean <strong>liv<strong>in</strong>g</strong> conditions are a concern butdo not appear <strong>to</strong> present a high immediate risk, possibly because ofthe recent clean<strong>in</strong>g. The fact that his home is becom<strong>in</strong>g dirty aga<strong>in</strong>highlights the importance of ongo<strong>in</strong>g supervision and follow-up wherepossible. He shows little awareness of any problems or the potentialrisks of not tak<strong>in</strong>g his medication, cont<strong>in</strong>u<strong>in</strong>g alcohol abuse, loss ofhome services or the state of his accommodation.49
CASE 2Mr B is a 33-year-old male with chronic schizophrenia who lives alone<strong>in</strong> a DoH bed-sit. Mr B was most recently hospitalised with an acuteepisode of schizophrenia over a year earlier. He has little <strong>in</strong>sight andhas avoided contact with mental health services s<strong>in</strong>ce his CommunityTreatment Order (CTO), compell<strong>in</strong>g him <strong>to</strong> comply with medication,lapsed more than six months previously. Mr B is generally suspiciousand irritable and the DoH had difficulty organis<strong>in</strong>g a rout<strong>in</strong>e <strong>in</strong>spectionof his accommodation. When the <strong>in</strong>spection was conducted, Mr Bwas found <strong>to</strong> be <strong>in</strong> a severe state of self-neglect. He has m<strong>in</strong>imalfurniture, but all the walls, fixtures and surfaces are severely dirty anddamaged by cigarette burns and moisture. The bathroom andkitchen are <strong>in</strong> a particularly bad state and the floor has beenextensively damaged by water. Mr B reports deliberately leav<strong>in</strong>g tapsdripp<strong>in</strong>g <strong>to</strong> obscure distress<strong>in</strong>g persecu<strong>to</strong>ry audi<strong>to</strong>ry halluc<strong>in</strong>ations.On the threat of eviction, Mr B agrees <strong>to</strong> see the mental health teambut refuses <strong>to</strong> go <strong>to</strong> hospital.DiscussionMr B has active psychotic symp<strong>to</strong>ms possibly associated with noncompliancewith treatment. Liv<strong>in</strong>g <strong>in</strong> conditions of severe domesticsqualor partly results from his psychotic symp<strong>to</strong>ms. The DoH shouldtake advantage of Mr B’s consent <strong>to</strong> see the mental health team andconduct an urgent or priority assessment. Although it is likely that MrB will require re-admission <strong>to</strong> hospital until his mental state improves(<strong>to</strong> permit clean<strong>in</strong>g and repairs and application <strong>for</strong> a further CTO) itmay be possible <strong>to</strong> recommence treatment <strong>in</strong> his currentaccommodation. If required, the DoH may be able <strong>to</strong> providealternative accommodation until clean<strong>in</strong>g and repairs are completed.Based on his response <strong>to</strong> treatment and his lack of <strong>in</strong>sight, it wouldprobably be advisable <strong>for</strong> the CTO <strong>to</strong> be ma<strong>in</strong>ta<strong>in</strong>ed. Educat<strong>in</strong>g Mr Babout his condition and the need <strong>for</strong> medication and m<strong>in</strong>imis<strong>in</strong>g anyadverse affects may improve compliance. Mr B may benefit fromattend<strong>in</strong>g a rehabilitation or <strong>liv<strong>in</strong>g</strong> skills program.If Mr B’s capacity <strong>to</strong> ma<strong>in</strong>ta<strong>in</strong> his own accommodation rema<strong>in</strong>s poordespite resolution of psychotic symp<strong>to</strong>ms and compliance withtreatment, consideration may need <strong>to</strong> be given <strong>to</strong> group hous<strong>in</strong>g,where he would have more supervision and support. Otherwise,s<strong>in</strong>ce the risk of relapse is high, ongo<strong>in</strong>g follow-up and moni<strong>to</strong>r<strong>in</strong>g byMental Health Services or the DoH or both would be highly desirable.If Mr B had changed his m<strong>in</strong>d and refused assessment by the mentalhealth team, an application <strong>to</strong> conduct an assessment under theMental Health Act 1990 may have been required. If Mr B hadcont<strong>in</strong>ued <strong>to</strong> resist <strong>in</strong>spection, the DoH could have applied <strong>to</strong> theConsumer Trader and Tenancy Tribunal (CTTT) <strong>to</strong> issue an accessorder, and authorise an <strong>in</strong>spection under the Residential TenancyAct. 1997. The DoH has the right <strong>to</strong> <strong>in</strong>spect public rental properties up<strong>to</strong> four times a year.50
CASE 3Ms D, who had been <strong>liv<strong>in</strong>g</strong> <strong>in</strong> public rental accommodation, washospitalised <strong>for</strong> an acute episode of a mental illness. In preparation <strong>for</strong>discharge, the occupational therapist went with Ms D <strong>to</strong> her home anddiscovered the severe neglect of property that had resulted from herillness. This <strong>in</strong>volved hoard<strong>in</strong>g, poor disposal of excreta, large amountsof rotten food and a major <strong>in</strong>festation of verm<strong>in</strong>. In addition, Ms D hadhad her electricity and gas disconnected. Application had been made <strong>to</strong>the Guardianship Tribunal <strong>for</strong> f<strong>in</strong>ancial management and this wasapproved. Ms D expressed considerable dismay at the condition of herflat and agreed <strong>to</strong> <strong>in</strong>dustrial clean<strong>in</strong>g. As part of the HACC TransitionPilot Project, 28 hours of clean<strong>in</strong>g was undertaken and Ms D returnedhome with the follow up support of workers from Community MentalHealth and Assistance with Care and Hous<strong>in</strong>g <strong>for</strong> the Aged (ACHA)Program. Ms D’s situation had not come <strong>to</strong> the attention of neighbours,the community or public hous<strong>in</strong>g workers.CASE 4Mr M was referred <strong>for</strong> <strong>assist</strong>ance with Care and Hous<strong>in</strong>g <strong>for</strong> the Aged(ACHA) Care and Assessment team by DoH, who had discoveredsevere domestic squalor whilst undertak<strong>in</strong>g a regular <strong>in</strong>spection of theproperty. DoH <strong>staff</strong> had also received compla<strong>in</strong>ts from neighboursabout Mr M’s behaviour <strong>in</strong>clud<strong>in</strong>g his abusive language and threats ofviolence affected by alcohol abuse. DoH <strong>staff</strong> attempted <strong>to</strong> negotiatethe organisation and disposal of some of his hundreds of books andother items. They enlisted the aid of the ACAT’s psycho-geriatricianand social worker, <strong>staff</strong> from ACHA and the Fire Brigade. Mr Mvacillated between be<strong>in</strong>g cooperative and agree<strong>in</strong>g <strong>to</strong> the idea ofgett<strong>in</strong>g rid of some of his th<strong>in</strong>gs, <strong>to</strong> outright refusal and hostility <strong>to</strong>wardsthose attempt<strong>in</strong>g <strong>to</strong> make him do th<strong>in</strong>gs he didn’t want <strong>to</strong> do. Inaddition, he thought his place was no more of a fire risk than thebookshop down the road. Strategies <strong>to</strong> address his situation <strong>in</strong>cludedbuild<strong>in</strong>g rapport over a long period of time, with the recognition that anychange <strong>in</strong> his home was likely <strong>to</strong> take a considerable amount of time.However, the DoH has a duty of care <strong>to</strong> other residents and if theproperty care issues pose a fire risk, the DoH would need <strong>to</strong> resolve itquickly. Additionally, council may also <strong>in</strong>voke its clean up powers if thecase was deemed <strong>to</strong> be a risk <strong>to</strong> the resident or neighbours.51
CASE 5A 62-year-old female lives <strong>in</strong> her own home unit, which is <strong>in</strong> a state ofsevere domestic squalor. She has a his<strong>to</strong>ry of head <strong>in</strong>jury and alcoholabuse result<strong>in</strong>g <strong>in</strong> moderate <strong>to</strong> severe frontal lobe damage. She is alsonoted <strong>to</strong> be <strong>in</strong> poor health and her diabetes is poorly controlled. Shehas a long his<strong>to</strong>ry of refus<strong>in</strong>g access, and has become verbally andphysically aggressive <strong>to</strong> workers when access has been soughtpreviously. Other residents <strong>in</strong> the block of units have compla<strong>in</strong>edbecause of the smell. Community Health services have received callsfrom the council and the units’ body corporate. The woman has beenserved a notice from the council request<strong>in</strong>g her <strong>to</strong> have her propertycleaned or she will be taken <strong>to</strong> court <strong>in</strong> accordance with the LocalGovernment Act 1993. The Public Guardian has been appo<strong>in</strong>ted <strong>to</strong>make decisions on her behalf and the Protective Commissionerappo<strong>in</strong>ted <strong>to</strong> manage her f<strong>in</strong>ances. Her GP is of the op<strong>in</strong>ion that,although she is extremely th<strong>in</strong> and <strong>in</strong> poor health, she does not needhospitalisation or placement <strong>in</strong> an aged care facility.DiscussionIn this case the person was recognised <strong>to</strong> have impaired decisionmak<strong>in</strong>gcapacity and sufficient need such that the GuardianshipTribunal has appo<strong>in</strong>ted the Public Guardian <strong>to</strong> be a substitute decisionmaker.Guardianship is decision-specific and <strong>in</strong>itially only the legalauthority <strong>to</strong> make decisions with relation <strong>to</strong> consent<strong>in</strong>g <strong>to</strong> medicaltreatment and accept<strong>in</strong>g home services was granted. A GuardianshipOrder is usually limited <strong>in</strong> time and scope. It is the responsibility of theGuardian <strong>to</strong> review the person’s circumstances and act <strong>in</strong> the best<strong>in</strong>terests of the person. Although the person may not have the capacity<strong>to</strong> make decisions, they may still be able <strong>to</strong> express a view orpreference and where possible this should be taken <strong>in</strong><strong>to</strong> account.Although the Guardian has legal authority <strong>for</strong> mak<strong>in</strong>g decisions on theperson’s behalf, it is the job of others, such as a case manager (if thereis one) <strong>to</strong> implement those decisions.Sometimes, areas of decision-mak<strong>in</strong>g <strong>in</strong>itially granted by theGuardianship Tribunal may be <strong>in</strong>sufficient. It may become apparentthat the substitute decision-maker also needs authority <strong>to</strong> makedecisions on behalf of the client <strong>in</strong> other areas, such as a change ofaccommodation. Alternatively, it may be impossible <strong>to</strong> implement anorder without the use of <strong>for</strong>ce, <strong>in</strong> which case ‘coercive powers’ will berequired. Authority <strong>for</strong> decision-mak<strong>in</strong>g <strong>in</strong> other areas or the use of‘coercion’ requires a further application <strong>to</strong> the Guardianship Tribunal.52
CASE 6Mr A. is a 70-year-old man who lives alone <strong>in</strong> his own home. He wasreferred <strong>to</strong> mental health services by his neighbour, who wasconcerned that he was <strong>in</strong> a severe state of self-neglect, and that hismental and physical health were decl<strong>in</strong><strong>in</strong>g. The neighbour reportedsee<strong>in</strong>g Mr A. talk<strong>in</strong>g <strong>to</strong> himself, and that he was becom<strong>in</strong>g<strong>in</strong>creas<strong>in</strong>gly pale and los<strong>in</strong>g weight. His house was extremelyneglected and dilapidated. There were several holes <strong>in</strong> the roof, noglass <strong>in</strong> the w<strong>in</strong>dows, no electricity and no water.Mental health services visited his home on several occasions but MrA. was never at home or refused <strong>to</strong> answer the door. He did notrespond <strong>to</strong> written requests <strong>to</strong> see him sent <strong>in</strong> by mail. He was notknown <strong>to</strong> have any <strong>liv<strong>in</strong>g</strong> friends or relatives. Mental health recordsconfirmed Mr A. had been admitted <strong>to</strong> hospital 30 years ago withschizophrenia, but was not known <strong>to</strong> have had any contact s<strong>in</strong>ce. MrA. was known <strong>to</strong> the local council, who had received compla<strong>in</strong>ts <strong>in</strong>relation <strong>to</strong> the neglected state of the property, and that the yard andgarden were over-grown. The council had cleared the yard onseveral occasions after his failure <strong>to</strong> respond <strong>to</strong> compulsory ordersunder the Local Government Act. Mr A.’s rates were <strong>in</strong> arrears, buthe made payments from time <strong>to</strong> time and last visited the counciloffices several months be<strong>for</strong>e. Otherwise, Mr A. is not known <strong>to</strong> havecaused any problems and is not known <strong>to</strong> be a danger <strong>to</strong> himself orothers.DiscussionBased upon the report of his neighbour, Mr A. may be at risk (fromuntreated mental illness, self neglect, poor nutrition) and furtherassessment is warranted. Whether further <strong>in</strong>tervention is required willdepend upon whether or not it is possible <strong>to</strong> see Mr A. at his home (orelsewhere) and his will<strong>in</strong>gness <strong>to</strong> cooperate. Assum<strong>in</strong>g it is possible<strong>to</strong> contact him, and he agrees <strong>to</strong> an assessment, a number of areasneed <strong>to</strong> be addressed.Medical and psychiatric assessment.As Mr A. has halluc<strong>in</strong>a<strong>to</strong>ry behaviour and a past his<strong>to</strong>ry of mentalillness, mental health services (the local psycho-geriatric service orcrisis team, <strong>for</strong> example) would need <strong>to</strong> undertake the <strong>in</strong>itialassessment. They would then determ<strong>in</strong>e whether furtherassessment by other medical specialists is required. Sometimes aperson may agree <strong>to</strong> see a general practitioner or a geriatrician (fromthe ACAT <strong>for</strong> example) be<strong>for</strong>e see<strong>in</strong>g a psychiatrist.Because of the suggestion of physical health problems and nutritionaldeficiencies (weight loss and pale appearance) a review of Mr A.’sphysical health is likely <strong>to</strong> be <strong>in</strong>dicated <strong>in</strong> any case. A physicalexam<strong>in</strong>ation and further <strong>in</strong>vestigations, such as blood tests, may alsobe required. In less urgent situations, workers from the Assistance53
with Care and Hous<strong>in</strong>g <strong>for</strong> the Aged program and non-governmen<strong>to</strong>rganisations are sometimes able <strong>to</strong> <strong>for</strong>ge an <strong>in</strong>itial relationship withthe client and obta<strong>in</strong> their consent <strong>to</strong> arrange medical appo<strong>in</strong>tments.Assess<strong>in</strong>g capacity. An important question <strong>to</strong> be addressed fromthe outset is whether or not Mr A. has the capacity <strong>to</strong> decide whetheror not he needs <strong>to</strong> receive further medical treatment (e.g.medications, hospitalisation, <strong>in</strong>vestigations) and rema<strong>in</strong> <strong>in</strong> his currentaccommodation. He needs <strong>to</strong> be able <strong>to</strong> understand the optionsavailable <strong>to</strong> him and the potential benefits and risks associated witheach of these.Environmental and public health assessment. Severe domesticsqualor can present the follow<strong>in</strong>g significant health risks <strong>to</strong> theoccupant, <strong>to</strong> neighbours and <strong>to</strong> the local community: fire from theaccumulation of large quantities of flammable material; rodents andother pests; and the spread of disease associated with lack of runn<strong>in</strong>gwater or lack of sewage. If these concerns are apparent <strong>in</strong> Mr A.’scase, it would be necessary <strong>to</strong> notify Environmental Health Officers(EHOs) with the local council.Clean<strong>in</strong>g. Clean<strong>in</strong>g is often difficult <strong>to</strong> organise and <strong>to</strong> pay <strong>for</strong>. If MrA.’s <strong>liv<strong>in</strong>g</strong> conditions are extreme and there are concerns aboutexposure <strong>to</strong> human waste, body fluids, excretions and an <strong>in</strong>fectionrisk, ‘<strong>for</strong>ensic’ clean<strong>in</strong>g may be required. The local council may beable <strong>to</strong> provide contact details <strong>for</strong> local clean<strong>in</strong>g services and <strong>assist</strong>with removal of property and rubbish. In milder cases, with less<strong>in</strong>fectious risk, particularly if Mr A. were voluntarily accept<strong>in</strong>g<strong>assist</strong>ance, some NGOs (such as Mercy Arms or the Brown Sisters)may undertake some of the clean<strong>in</strong>g themselves. A small amount offund<strong>in</strong>g is available from the Department of Age<strong>in</strong>g, Disability andHome Care (DADHC) <strong>to</strong> broker clean<strong>in</strong>g services <strong>in</strong> some cases.What happens if Mr A. persistently resists assessment and/or<strong>in</strong>tervention?Should Mr A. be cont<strong>in</strong>ually unavailable <strong>for</strong> assessment and theconcerns <strong>in</strong> relation <strong>to</strong> his health and <strong>liv<strong>in</strong>g</strong> conditions persist, thereare several ways <strong>in</strong> which his case could be dealt with. These arelikely <strong>to</strong> be <strong>in</strong>fluenced by which service has had the most<strong>in</strong>volvement. In Mr A.’s case, this would be mental health servicesand the local council. A jo<strong>in</strong>t approach (tak<strong>in</strong>g as much care <strong>to</strong>ma<strong>in</strong>ta<strong>in</strong> confidentiality as possible), with one service tak<strong>in</strong>g on therole of the ‘lead agency’ and identify<strong>in</strong>g a coord<strong>in</strong>a<strong>to</strong>r or ‘key worker’,is probably the ideal. Cont<strong>in</strong>u<strong>in</strong>g ef<strong>for</strong>ts should be made <strong>to</strong> engageMr A. and conv<strong>in</strong>ce him <strong>to</strong> accept help voluntarily.If Mr A. cont<strong>in</strong>ues <strong>to</strong> resist, legal authorisation <strong>to</strong> enter his home <strong>to</strong>conduct an assessment, is required. If there is evidence of a likelymental illness, mental health services could apply <strong>to</strong> the local court <strong>for</strong>authority <strong>to</strong> conduct an assessment under the Mental Health Act. This54
would permit a psychiatrist <strong>to</strong> enter his home (<strong>in</strong> the presence ofPolice and, if necessary, by <strong>for</strong>ce) <strong>to</strong> enable a medical exam<strong>in</strong>ation,<strong>in</strong>clud<strong>in</strong>g an assessment of capacity and risk.If Mr A. were determ<strong>in</strong>ed <strong>to</strong> be mentally ill and at risk, the psychiatristcould request the police <strong>to</strong> hospitalise him <strong>for</strong> further assessmentand/or treatment under the Mental Health Act 1990.If authority <strong>to</strong> undertake an assessment was not granted <strong>to</strong> themental health services, then the council could <strong>in</strong>voke its powersunder the amended Local Government Act 1993 and order a cleanup without Mr. A.’s consent.55
APPENDIX 9: <strong>NSW</strong> Government and non-Governmentagencies 8GovernmentDepartment of Local GovernmentO’Keefe AvenueNowra <strong>NSW</strong> 2541Phone: (02) 4428 4100www.dlg.nsw.gov.auDepartment of Community Services4-6 Cavill AvenueAsh<strong>field</strong> <strong>NSW</strong> 2131Phone: (02) 9716 2222www.community.nsw.gov.auDepartment of Health (<strong>NSW</strong>)73 Miller StreetNorth Sydney <strong>NSW</strong> 2060Phone: (02) 9391 9000www.health.nsw.gov.auDepartment of Disability, Age<strong>in</strong>gand Home Care (<strong>NSW</strong>)Level 5, 83 Clarence StreetSydney <strong>NSW</strong> 2000Phone: (02) 8270 2000TTY: (02) 8270 2167 (Hear<strong>in</strong>g Impaired)www.dadhc.nsw.gov.auOffice of the Protective CommissionerLevel 15, 133 Castlereagh StreetSydney <strong>NSW</strong> 2000Phone: 1300 360 466 (local call)1800 882 889www.lawl<strong>in</strong>k.nsw.gov.au/opcCommonwealth Carel<strong>in</strong>k CentreGPO Box 9848Sydney <strong>NSW</strong> 2001Phone: 1800 052 222www.commcarel<strong>in</strong>k.health.gov.auAged and Community Care In<strong>for</strong>mation L<strong>in</strong>eGPO Box 9848Canberra ACT 2601Phone: 1800 500 853www.seniors.gov.auOffice of the Public GuardianLevel 15133 Castlereagh StreetSydney 2000Phone: (02) 9265 3184 Toll-free: 1800 451 510www.lawl<strong>in</strong>k.nsw.gov.au/opgGuardianship TribunalLevel 3, 2a Rowntree StreetBalma<strong>in</strong> <strong>NSW</strong> 2041Phone: (02) 9555 8500Toll free 1800 463 928www.gt.nsw.govDepartment of Hous<strong>in</strong>g (<strong>NSW</strong>)223-239 Liverpool StreetAsh<strong>field</strong> <strong>NSW</strong> 2131Phone: Toll Free 1800 629 212www.hous<strong>in</strong>g.nsw.gov.auOffice of Fair Trad<strong>in</strong>g1 Fitzwilliam StreetParramatta <strong>NSW</strong> 250Phone: 13 3220www.fairtrad<strong>in</strong>g.nsw.gov.auPolice (<strong>NSW</strong>)1 Charles StParramatta <strong>NSW</strong> 2150Phone: (02) 9281 0000 (ask <strong>for</strong> local station)www.police.nsw.gov.auFire Brigade (<strong>NSW</strong>)Risk Management Direc<strong>to</strong>rateLocked Bag 12P.O. Greenacre <strong>NSW</strong> 2190Phone: (02) 9742 7400www.nswfb.nsw.gov.auAborig<strong>in</strong>al Hous<strong>in</strong>g OfficeLevel 6, 33 Argyle StreetParramatta <strong>NSW</strong> 2050Phone: (02) 8836 9444www.aho.nsw.gov.au8 This is not an exhaustive list of services, but rather a start<strong>in</strong>g po<strong>in</strong>t <strong>for</strong> <strong>in</strong><strong>for</strong>mation. Most governmentagencies have state-wide coverage, while some non-government agencies may extend <strong>to</strong> or provide <strong>in</strong><strong>for</strong>mationon similar services <strong>in</strong> other areas of <strong>NSW</strong>.56
Non-GovernmentAssistance with Care and Hous<strong>in</strong>g <strong>for</strong> theAged (ACHA) Unit<strong>in</strong>g Care1 Glover StreetLeichhardt <strong>NSW</strong> 2040Phone: 9810 1561Brown Sisters Inner City12 Leichhardt StreetDarl<strong>in</strong>ghurst <strong>NSW</strong> 2010Phone: 9360 543Mercy Arms Community Care(<strong>for</strong> Botany, City of Sydney, Hurstville, Kogarah,Leichhardt, Marrickville, Randwick, Rockdale,Waverley and Woollahra)Ph: 1800 225 474Mercy Community Care, Lower North Shore(<strong>for</strong> Mosman, Lane Cove, North Sydney,Willoughby)Ph: 8425 7100Mercy Community Care, Thornleigh(<strong>for</strong> Hornsby/Ku-r<strong>in</strong>g-gai, Ryde/Hunters Hill andManly/Warr<strong>in</strong>gah/Pittwater)Ph: 9479 3333St Lukes Community Home Care18 Roslyn StreetPotts Po<strong>in</strong>t <strong>NSW</strong> 2011Phone: (02) 9356 0424Alcohol and Drug In<strong>for</strong>mation Service (ADIS)St. V<strong>in</strong>cent’s Hospital,Vic<strong>to</strong>ria StreetDarl<strong>in</strong>ghurst <strong>NSW</strong>Free call outside Sydney: 1800 422 599Phone: 9361 8000wwwsvh.stv<strong>in</strong>cents.com.au/drugsandalc.htmTenants Advice and In<strong>for</strong>mation Service88 Bett<strong>in</strong>g<strong>to</strong>n StreetMillers Po<strong>in</strong>t <strong>NSW</strong> 2000Phone: (02) 9251 6590Freecall: 1800 251 101www.tenants.org.auMulticultural DisabilityAdvocacy Association40 Albion StreetHarris Park <strong>NSW</strong> 2150Phone: (02) 9635 5355www.mdaa.org.auAborig<strong>in</strong>al Medical ServiceP.O. Box 1174Strawberry Hills <strong>NSW</strong> 2012Phone: (02) 9319 5823Ethnic Communities Council221 Cope StreetWaterloo <strong>NSW</strong> 2017Phone: (02) 9319 0288www.eccnsw.org.auRSPCA201 Rookwood RdYagoona <strong>NSW</strong> 2199Phone: (02) 9770 7555www.rspcansw.org.au57
APPENDIX 10:Table of abbreviationsACATADISCACPCTOCTTTDADHCDoCSDSPDoHEHOFMOHACCMERITNGOOPCOPGAged Care Assessment TeamAlcohol and Drug In<strong>for</strong>mation ServiceCommunity Aged Care PackagesCommunity Treatment OrderConsumer Traders and Tenancy TribunalDepartment of Age<strong>in</strong>g, Disability and Home CareDepartment of Community ServicesDisability Services ProgramsDepartment of Hous<strong>in</strong>gEnvironmental Health OfficerF<strong>in</strong>ancial Management OrderHome and Community CareMagistrates Early Referral <strong>in</strong><strong>to</strong> Treatment ProgramNon-government organisationOffice of the Protective CommissionerOffice of the Public Guardian58
APPENDIX 11:Further read<strong>in</strong>gClark ANG, Manikar GO, Gray J (1975) Diogenes' Syndrome: a cl<strong>in</strong>ical study ofgross self-neglect <strong>in</strong> old age. Lancet, ii, 366-368.Cooney C, Hamid W (1995) Review: Diogenes Syndrome. Age & Age<strong>in</strong>g, 24, 451-453.Cybulska E, Ruc<strong>in</strong>ski J (1986) Gross-self neglect <strong>in</strong> old age. British Journal of HospitalMedic<strong>in</strong>e, 36, 21-24.Clutter Workshop Organisation. www.clutterworkshop.comDrummond LM, Turner J, Reid S (1997) Diogenes' Syndrome - a load of old rubbish.Irish Journal of Psychological Medic<strong>in</strong>e, 14, 99-102.Frost RO, Steketee G Williams L (2000) Hoard<strong>in</strong>g: a community health problem.Health and Social Care <strong>in</strong> the Community, 8, 229-34.Halliday G, Banerjee S, Philpott M, MacDonald A (2000) Community study of <strong>people</strong>who live <strong>in</strong> squalor. Lancet, 355, 882-886.Macmillan D, Shaw P (1966) Senile breakdown <strong>in</strong> standards of personal andenvironmental cleanl<strong>in</strong>ess. British Medical Journal, 2, 1032-1037.New York City Hoard<strong>in</strong>g Task Forcewww.cornellag<strong>in</strong>g.com/gem/hoa_nyc_hoa_tas.htmlOffice of the Medical Officer of Health (2000) Middlesex-London Health Unit, TaskForce on Senile Squalor, F<strong>in</strong>al Report.Orrell M, Sahakian B, Bergmann K (1989) Self-neglect and frontal lobe dysfunction.British Journal of Psychiatry, 155, 101-105.Patronek GJ (1999) Hoard<strong>in</strong>g of animals: and under recognised public healthproblem <strong>in</strong> a difficult <strong>to</strong> study population. Public health reports, 114, 81-87.Reifler B (1996) Diogenes Syndrome: of Omelettes and Souffles. Journal of theAmerican Geriatric Society, 44, 1484-1485.Samios K (1996) In<strong>to</strong> the loathsome den: the characteristics of persons <strong>liv<strong>in</strong>g</strong> <strong>in</strong>squalor Sydney: Royal Australian and New Zealand College of Psychiatrists(dissertation).Scallon E, De La Harpe D, Johnson H Hurley M (2000). Adult service refusers <strong>in</strong> theGreater Dubl<strong>in</strong> area. Irish Medical Journal, 93, 208-211.Snowdon J (1987) Uncleanl<strong>in</strong>ess among persons seen by community health workers.Hospital and Community Psychiatry, 38, 491-494.Snowdon J, Shah A, Halliday G (2006) ‘Severe domestic squalor: a review’ <strong>in</strong>International Psychogeriatrics, www.journals.cambridge.org/jid_IPGSteketee G, Frost RO, Kim H-J (2001) Hoard<strong>in</strong>g by elderly <strong>people</strong>. Health & SocialWork, 26, 176-184.Wrigley M, Cooney C (1992) Diogenes syndrome: an Irish series. Irish Journal ofPsychological Medic<strong>in</strong>e, 9, 37-41.59
APPENDIX 12:AcknowledgementsMembers of Reference GroupJohn Snowdon Psycho-geriatrician Central Sydney Area HealthGraeme Halliday Psycho-geriatrician Central Sydney Area HealthBrett Simpson Psycho-geriatrician Central Sydney Area HealthMarcia Sherr<strong>in</strong>g Community Services Worker/Cl<strong>in</strong>ician Central Sydney Drug & AlcoholDeborah Baunach Crime Prevention Officer <strong>NSW</strong> Police DepartmentChris Lewis Risk Management Fire Brigade – <strong>NSW</strong>Anne Lear Risk Management Fire Brigade – <strong>NSW</strong>Chris Codd<strong>in</strong>g<strong>to</strong>n Metropolitan Team Leader RSPCAJacki Campisi Community Worker <strong>for</strong> Older People Waverely Council Comm. ServicesNat Ryan Shared Accommodation Officer Sydney Municipal CouncilValerie Joy Community Worker Leichhhardt Municipal CouncilRobyn Craw<strong>for</strong>d Senior Client Service Officer <strong>NSW</strong> Department of Hous<strong>in</strong>gDoug Boquist Senior Client Service Officer <strong>NSW</strong> Department of Hous<strong>in</strong>gAlexandra Matt<strong>in</strong>son Senior Client Service Officer <strong>NSW</strong> Department of Hous<strong>in</strong>gHeather McGillivray Team Leader HATSOS <strong>NSW</strong> Department of Hous<strong>in</strong>gNarelle Lyons Aborig<strong>in</strong>al Liaison <strong>NSW</strong> Department of Hous<strong>in</strong>gSue Cripps Manager HATSOS <strong>NSW</strong> Department of Hous<strong>in</strong>gLeslee Murphy A/Assistant Direc<strong>to</strong>r, Disability Advisory Service Protective commissioner of <strong>NSW</strong>Frances Rush Regional Manager Office of Public GuardianPatricia Davidson Regional Manager Office of Public GuardianRobyn Murray Manager Cl<strong>in</strong>ical Policy and Practice <strong>NSW</strong> Department of HealthStephen Cashen Case Manager Redfern Community Health CentreRosemary Sheehy Geriatrician Balma<strong>in</strong> HospitalAnne Wag<strong>staff</strong> Cl<strong>in</strong>ical Nurse Consultant SE Sydney Area HealthKate Daley Social Worker SE Sydney Area HealthWilliam S<strong>to</strong>ne Cl<strong>in</strong>ical Nurse Consultant SE Sydney Area HealthLeo Barre<strong>to</strong> Social Worker SE Sydney Area HealthMargaret Flynn Cl<strong>in</strong>ical Nurse Consultant Mid North Coast Area HealthJohn Hislop Lawyer <strong>NSW</strong> Guardianship TribunalEsther Cho Legal Officer <strong>NSW</strong> Guardianship TribunalNick O’Neil President <strong>NSW</strong> Guardianship TribunalJanet McNeill Project Officer DADHCCathy Murphy Regional Manager DADHCKev<strong>in</strong> Reilly A/Regional Manager DADHCDavid Bate Regional Direc<strong>to</strong>r DADHCSaul Hanly Service Coord<strong>in</strong>a<strong>to</strong>r, Eastern Sydney DADHCRuth Melville Coord<strong>in</strong>a<strong>to</strong>r Mercy ArmsKay Kavanagh Manager Mercy ArmsPaul<strong>in</strong>e Fogarty Coord<strong>in</strong>a<strong>to</strong>r Brown NursesJoel deFreitas Outreach Worker Lucan Care (ACHA)Maida Chand Manager Lucan CareMaureen Bensoc Coord<strong>in</strong>a<strong>to</strong>r Community Care Community OptionsKath<strong>in</strong>aka L<strong>in</strong>ahan Manager Community Care Community OptionsGrace Noonan Case Manager St Lukes Community Home CareTony Fl<strong>in</strong>n Case Manager Anglican Retirement VillagesRoslyn McLoughl<strong>in</strong> Community Case Worker Mosman Municipal CouncilKate Sale Environmental Health Officer Mosman Municipal CouncilMart<strong>in</strong> Ellis Direc<strong>to</strong>r Community & Library Services North Sydney Municipal CouncilElle McK<strong>in</strong>non Manager Aurora Property ServicesChris Lynch Manager Aurora Property ServicesOther Contribu<strong>to</strong>rsLocal government services <strong>in</strong> Graf<strong>to</strong>n, Taree60