

Practice Parameter and Literature Review of the Usefulness of ...
Practice Parameter and Literature Review of the Usefulness of ...
Practice Parameter and Literature Review of the Usefulness of ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
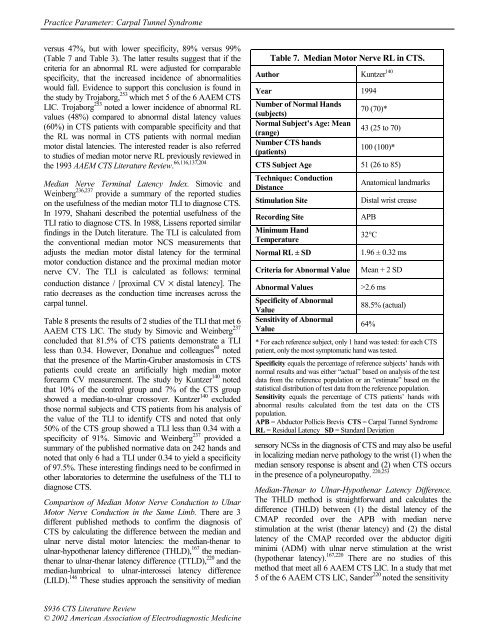
<strong>Practice</strong> <strong>Parameter</strong>: Carpal Tunnel Syndromeversus 47%, but with lower specificity, 89% versus 99%(Table 7 <strong>and</strong> Table 3). The latter results suggest that if <strong>the</strong>criteria for an abnormal RL were adjusted for comparablespecificity, that <strong>the</strong> increased incidence <strong>of</strong> abnormalitieswould fall. Evidence to support this conclusion is found in<strong>the</strong> study by Trojaborg, 253 which met 5 <strong>of</strong> <strong>the</strong> 6 AAEM CTSLIC. Trojaborg 253 noted a lower incidence <strong>of</strong> abnormal RLvalues (48%) compared to abnormal distal latency values(60%) in CTS patients with comparable specificity <strong>and</strong> that<strong>the</strong> RL was normal in CTS patients with normal medianmotor distal latencies. The interested reader is also referredto studies <strong>of</strong> median motor nerve RL previously reviewed in<strong>the</strong> 1993 AAEM CTS <strong>Literature</strong> <strong>Review</strong>. 66,116,137,204Median Nerve Terminal Latency Index. Simovic <strong>and</strong>Weinberg 236,237 provide a summary <strong>of</strong> <strong>the</strong> reported studieson <strong>the</strong> usefulness <strong>of</strong> <strong>the</strong> median motor TLI to diagnose CTS.In 1979, Shahani described <strong>the</strong> potential usefulness <strong>of</strong> <strong>the</strong>TLI ratio to diagnose CTS. In 1988, Lissens reported similarfindings in <strong>the</strong> Dutch literature. The TLI is calculated from<strong>the</strong> conventional median motor NCS measurements thatadjusts <strong>the</strong> median motor distal latency for <strong>the</strong> terminalmotor conduction distance <strong>and</strong> <strong>the</strong> proximal median motornerve CV. The TLI is calculated as follows: terminalconduction distance / [proximal CV × distal latency]. Theratio decreases as <strong>the</strong> conduction time increases across <strong>the</strong>carpal tunnel.Table 8 presents <strong>the</strong> results <strong>of</strong> 2 studies <strong>of</strong> <strong>the</strong> TLI that met 6AAEM CTS LIC. The study by Simovic <strong>and</strong> Weinberg 237concluded that 81.5% <strong>of</strong> CTS patients demonstrate a TLIless than 0.34. However, Donahue <strong>and</strong> colleagues 60 notedthat <strong>the</strong> presence <strong>of</strong> <strong>the</strong> Martin-Gruber anastomosis in CTSpatients could create an artificially high median motorforearm CV measurement. The study by Kuntzer 140 notedthat 10% <strong>of</strong> <strong>the</strong> control group <strong>and</strong> 7% <strong>of</strong> <strong>the</strong> CTS groupshowed a median-to-ulnar crossover. Kuntzer 140 excludedthose normal subjects <strong>and</strong> CTS patients from his analysis <strong>of</strong><strong>the</strong> value <strong>of</strong> <strong>the</strong> TLI to identify CTS <strong>and</strong> noted that only50% <strong>of</strong> <strong>the</strong> CTS group showed a TLI less than 0.34 with aspecificity <strong>of</strong> 91%. Simovic <strong>and</strong> Weinberg 237 provided asummary <strong>of</strong> <strong>the</strong> published normative data on 242 h<strong>and</strong>s <strong>and</strong>noted that only 6 had a TLI under 0.34 to yield a specificity<strong>of</strong> 97.5%. These interesting findings need to be confirmed ino<strong>the</strong>r laboratories to determine <strong>the</strong> usefulness <strong>of</strong> <strong>the</strong> TLI todiagnose CTS.Comparison <strong>of</strong> Median Motor Nerve Conduction to UlnarMotor Nerve Conduction in <strong>the</strong> Same Limb. There are 3different published methods to confirm <strong>the</strong> diagnosis <strong>of</strong>CTS by calculating <strong>the</strong> difference between <strong>the</strong> median <strong>and</strong>ulnar nerve distal motor latencies: <strong>the</strong> median-<strong>the</strong>nar toulnar-hypo<strong>the</strong>nar latency difference (THLD), 167 <strong>the</strong> median<strong>the</strong>narto ulnar-<strong>the</strong>nar latency difference (TTLD), 220 <strong>and</strong> <strong>the</strong>median-lumbrical to ulnar-interossei latency difference(LILD). 146 These studies approach <strong>the</strong> sensitivity <strong>of</strong> medianTable 7. Median Motor Nerve RL in CTS.Author Kuntzer 140Year 1994Number <strong>of</strong> Normal H<strong>and</strong>s(subjects)70 (70)*Normal Subject’s Age: Mean(range)43 (25 to 70)Number CTS h<strong>and</strong>s(patients)100 (100)*CTS Subject Age 51 (26 to 85)Technique: ConductionDistanceAnatomical l<strong>and</strong>marksStimulation SiteDistal wrist creaseRecording SiteMinimum H<strong>and</strong>TemperatureNormal RL ± SDCriteria for Abnormal ValueAbnormal ValuesSpecificity <strong>of</strong> AbnormalValueSensitivity <strong>of</strong> AbnormalValueAPB32°C1.96 ± 0.32 msMean + 2 SD>2.6 ms88.5% (actual)64%* For each reference subject, only 1 h<strong>and</strong> was tested: for each CTSpatient, only <strong>the</strong> most symptomatic h<strong>and</strong> was tested.Specificity equals <strong>the</strong> percentage <strong>of</strong> reference subjects’ h<strong>and</strong>s withnormal results <strong>and</strong> was ei<strong>the</strong>r “actual” based on analysis <strong>of</strong> <strong>the</strong> testdata from <strong>the</strong> reference population or an “estimate” based on <strong>the</strong>statistical distribution <strong>of</strong> test data from <strong>the</strong> reference population.Sensitivity equals <strong>the</strong> percentage <strong>of</strong> CTS patients’ h<strong>and</strong>s withabnormal results calculated from <strong>the</strong> test data on <strong>the</strong> CTSpopulation.APB = Abductor Pollicis Brevis CTS = Carpal Tunnel SyndromeRL = Residual Latency SD = St<strong>and</strong>ard Deviationsensory NCSs in <strong>the</strong> diagnosis <strong>of</strong> CTS <strong>and</strong> may also be usefulin localizing median nerve pathology to <strong>the</strong> wrist (1) when <strong>the</strong>median sensory response is absent <strong>and</strong> (2) when CTS occursin <strong>the</strong> presence <strong>of</strong> a polyneuropathy. 220,253Median-Thenar to Ulnar-Hypo<strong>the</strong>nar Latency Difference.The THLD method is straightforward <strong>and</strong> calculates <strong>the</strong>difference (THLD) between (1) <strong>the</strong> distal latency <strong>of</strong> <strong>the</strong>CMAP recorded over <strong>the</strong> APB with median nervestimulation at <strong>the</strong> wrist (<strong>the</strong>nar latency) <strong>and</strong> (2) <strong>the</strong> distallatency <strong>of</strong> <strong>the</strong> CMAP recorded over <strong>the</strong> abductor digitiminimi (ADM) with ulnar nerve stimulation at <strong>the</strong> wrist(hypo<strong>the</strong>nar latency). 167,220 There are no studies <strong>of</strong> thismethod that meet all 6 AAEM CTS LIC. In a study that met5 <strong>of</strong> <strong>the</strong> 6 AAEM CTS LIC, S<strong>and</strong>er 220 noted <strong>the</strong> sensitivityS936 CTS <strong>Literature</strong> <strong>Review</strong>© 2002 American Association <strong>of</strong> Electrodiagnostic Medicine














