<strong>Assessment</strong> <strong>of</strong> <strong>quality</strong> <strong>of</strong> <strong>care</strong> <strong>for</strong> <strong>children</strong> <strong>in</strong> <strong>selected</strong> <strong>hospitals</strong> <strong>in</strong> Ghanasurgeries <strong>in</strong>cluded <strong>in</strong>cision and dra<strong>in</strong>age, hernia repair, hydrocoelectomy, excision <strong>of</strong> lumps,and repair <strong>of</strong> lacerations. Circumcision was commonly per<strong>for</strong>med <strong>in</strong> the <strong>hospitals</strong> but notdocumented, thus records were not available <strong>in</strong> most cases. Additional surgeries carried outwere reduction and immobilisation <strong>of</strong> fractures <strong>in</strong> one regional hospital, and sk<strong>in</strong>graft<strong>in</strong>g/reconstructive surgery <strong>in</strong> a district hospital with<strong>in</strong> a buruli ulcer endemic area.Essential drugs, equipment and suppliesThe full complement <strong>of</strong> essential drugs, equipment and supplies needed <strong>for</strong> paediatric <strong>care</strong>were not available <strong>in</strong> all the facilities as shown <strong>in</strong> the table below. In some facilities, drugswere available at the pharmacy but were not found at the emergency area or ward. Alsosome programme drugs, such as anti‐tuberculous drugs, were managed at the DistrictHealth Directorate. Essential equipment and supplies, such as oxygen, nebulizers andglucometers, were not available <strong>in</strong> some <strong>children</strong>’s units.The hospital laboratories provided 24 hour support services <strong>in</strong> all the facilities visited,however some tests, such as cerebrosp<strong>in</strong>al fluid (CSF) microscopy, blood group<strong>in</strong>g andcross‐match<strong>in</strong>g, were not available <strong>in</strong> some <strong>of</strong> the facilities. If a differential diagnosis <strong>of</strong>men<strong>in</strong>gitis was made, there was usually no way <strong>of</strong> confirm<strong>in</strong>g it due to the absence <strong>of</strong> a CSFmicroscopy test. In the case <strong>of</strong> one hospital, a private firm provides laboratory services.In most facilities, other emergency laboratory tests, such as haemoglob<strong>in</strong>, blood film, andgroup<strong>in</strong>g and cross match<strong>in</strong>g, were provided not only dur<strong>in</strong>g regular bus<strong>in</strong>ess hours, butalso at night, at weekends and dur<strong>in</strong>g holidays. Most <strong>of</strong> the laboratory tests were able to bedone with<strong>in</strong> two hours and <strong>for</strong> <strong>in</strong>patients, the results were obta<strong>in</strong>ed with<strong>in</strong> 24 hours.Table 2: Availability <strong>of</strong> drugs, equipment, supplies and laboratory supportNumber <strong>of</strong> facilities out <strong>of</strong> 10 found to be:Care assessed Good In need <strong>of</strong> someimprovementCommentsAvailability <strong>of</strong> essential drugs 4 6Availability <strong>of</strong> paediatric equipment 2 8 Infant-sized equipment notavailable <strong>in</strong> some facilities.Adequate equipment is available <strong>in</strong>the emergency area and on theward2 8Essential laboratory tests availableand timely2.3 Emergency <strong>care</strong> servicesPatient flow4 6 Test<strong>in</strong>g <strong>for</strong> CSF not available <strong>in</strong>all facilities.There was no separate outpatient department <strong>for</strong> <strong>children</strong> <strong>in</strong> any <strong>of</strong> the health facilities and<strong>children</strong> jo<strong>in</strong>ed adults <strong>in</strong> the same queue <strong>for</strong> their hospital cards <strong>in</strong> all the facilities. Therewere designated health pr<strong>of</strong>essionals to see sick <strong>children</strong> at the OPD <strong>in</strong> three facilities. Twohad paediatricians, while <strong>in</strong> the other a staff member tra<strong>in</strong>ed <strong>in</strong> <strong>in</strong>tegrated management <strong>of</strong><strong>children</strong>’s illnesses (IMCI) solely sees <strong>children</strong> less than five years <strong>of</strong> age. All sick <strong>children</strong> atthese three facilities, <strong>in</strong>clud<strong>in</strong>g emergencies and severely ill <strong>children</strong>, were received at thesame place <strong>in</strong> the OPD.Page 6
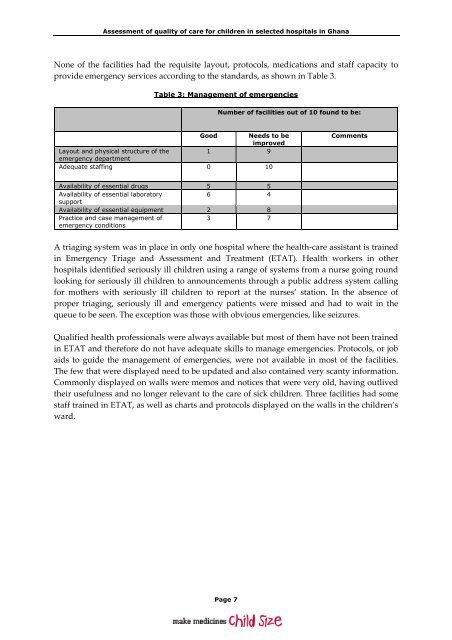
<strong>Assessment</strong> <strong>of</strong> <strong>quality</strong> <strong>of</strong> <strong>care</strong> <strong>for</strong> <strong>children</strong> <strong>in</strong> <strong>selected</strong> <strong>hospitals</strong> <strong>in</strong> GhanaNone <strong>of</strong> the facilities had the requisite layout, protocols, medications and staff capacity toprovide emergency services accord<strong>in</strong>g to the standards, as shown <strong>in</strong> Table 3.Table 3: Management <strong>of</strong> emergenciesNumber <strong>of</strong> facilities out <strong>of</strong> 10 found to be:GoodNeeds to beimprovedLayout and physical structure <strong>of</strong> the1 9emergency departmentAdequate staff<strong>in</strong>g 0 10CommentsAvailability <strong>of</strong> essential drugs 5 5Availability <strong>of</strong> essential laboratory6 4supportAvailability <strong>of</strong> essential equipment 2 8Practice and case management <strong>of</strong>emergency conditions3 7A triag<strong>in</strong>g system was <strong>in</strong> place <strong>in</strong> only one hospital where the health‐<strong>care</strong> assistant is tra<strong>in</strong>ed<strong>in</strong> Emergency Triage and <strong>Assessment</strong> and Treatment (ETAT). Health workers <strong>in</strong> other<strong>hospitals</strong> identified seriously ill <strong>children</strong> us<strong>in</strong>g a range <strong>of</strong> systems from a nurse go<strong>in</strong>g roundlook<strong>in</strong>g <strong>for</strong> seriously ill <strong>children</strong> to announcements through a public address system call<strong>in</strong>g<strong>for</strong> mothers with seriously ill <strong>children</strong> to report at the nurses’ station. In the absence <strong>of</strong>proper triag<strong>in</strong>g, seriously ill and emergency patients were missed and had to wait <strong>in</strong> thequeue to be seen. The exception was those with obvious emergencies, like seizures.Qualified health pr<strong>of</strong>essionals were always available but most <strong>of</strong> them have not been tra<strong>in</strong>ed<strong>in</strong> ETAT and there<strong>for</strong>e do not have adequate skills to manage emergencies. Protocols, or jobaids to guide the management <strong>of</strong> emergencies, were not available <strong>in</strong> most <strong>of</strong> the facilities.The few that were displayed need to be updated and also conta<strong>in</strong>ed very scanty <strong>in</strong><strong>for</strong>mation.Commonly displayed on walls were memos and notices that were very old, hav<strong>in</strong>g outlivedtheir usefulness and no longer relevant to the <strong>care</strong> <strong>of</strong> sick <strong>children</strong>. Three facilities had somestaff tra<strong>in</strong>ed <strong>in</strong> ETAT, as well as charts and protocols displayed on the walls <strong>in</strong> the <strong>children</strong>’sward.Page 7