A/V Services Order Form - Consumer Healthcare Products Association
A/V Services Order Form - Consumer Healthcare Products Association
A/V Services Order Form - Consumer Healthcare Products Association

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
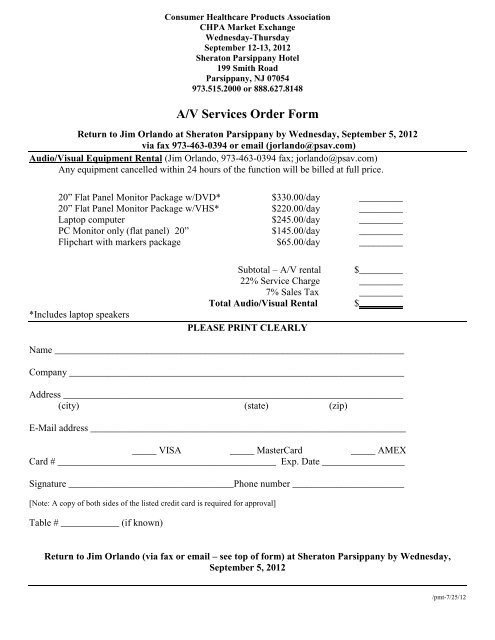
<strong>Consumer</strong> <strong>Healthcare</strong> <strong>Products</strong> <strong>Association</strong><br />
CHPA Market Exchange<br />
Wednesday-Thursday<br />
September 12-13, 2012<br />
Sheraton Parsippany Hotel<br />
199 Smith Road<br />
Parsippany, NJ 07054<br />
973.515.2000 or 888.627.8148<br />
A/V <strong>Services</strong> <strong>Order</strong> <strong>Form</strong><br />
Return to Jim Orlando at Sheraton Parsippany by Wednesday, September 5, 2012<br />
via fax 973-463-0394 or email (jorlando@psav.com)<br />
Audio/Visual Equipment Rental (Jim Orlando, 973-463-0394 fax; jorlando@psav.com)<br />
Any equipment cancelled within 24 hours of the function will be billed at full price.<br />
20” Flat Panel Monitor Package w/DVD* $330.00/day _________<br />
20” Flat Panel Monitor Package w/VHS* $220.00/day _________<br />
Laptop computer $245.00/day _________<br />
PC Monitor only (flat panel) 20” $145.00/day _________<br />
Flipchart with markers package $65.00/day _________<br />
*Includes laptop speakers<br />
Subtotal – A/V rental $_________<br />
22% Service Charge _________<br />
7% Sales Tax _________<br />
Total Audio/Visual Rental $_________<br />
PLEASE PRINT CLEARLY<br />
Name ________________________________________________________________________<br />
Company _____________________________________________________________________<br />
Address ______________________________________________________________________<br />
(city) (state) (zip)<br />
E-Mail address _________________________________________________________________<br />
_____ VISA _____ MasterCard _____ AMEX<br />
Card # _____________________________________________ Exp. Date _________________<br />
Signature __________________________________Phone number _______________________<br />
[Note: A copy of both sides of the listed credit card is required for approval]<br />
Table # ____________ (if known)<br />
Return to Jim Orlando (via fax or email – see top of form) at Sheraton Parsippany by Wednesday,<br />
September 5, 2012<br />
/pmt-7/25/12