

Safeguarding
Safeguarding patients - BiP Solutions Ltd.
Safeguarding patients - BiP Solutions Ltd.
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Safeguarding</strong> Patients 89<br />
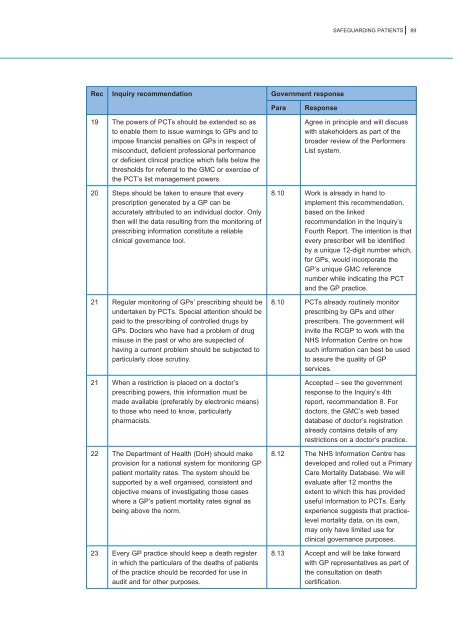
Rec Inquiry recommendation Government response<br />
Para<br />
Response<br />
19 The powers of PCTs should be extended so as<br />
to enable them to issue warnings to GPs and to<br />
impose financial penalties on GPs in respect of<br />
misconduct, deficient professional performance<br />
or deficient clinical practice which falls below the<br />
thresholds for referral to the GMC or exercise of<br />
the PCT’s list management powers.<br />
20 Steps should be taken to ensure that every<br />
prescription generated by a GP can be<br />
accurately attributed to an individual doctor. Only<br />
then will the data resulting from the monitoring of<br />
prescribing information constitute a reliable<br />
clinical governance tool.<br />
21 Regular monitoring of GPs’ prescribing should be<br />
undertaken by PCTs. Special attention should be<br />
paid to the prescribing of controlled drugs by<br />
GPs. Doctors who have had a problem of drug<br />
misuse in the past or who are suspected of<br />
having a current problem should be subjected to<br />
particularly close scrutiny.<br />
21 When a restriction is placed on a doctor’s<br />
prescribing powers, this information must be<br />
made available (preferably by electronic means)<br />
to those who need to know, particularly<br />
pharmacists.<br />
22 The Department of Health (DoH) should make<br />
provision for a national system for monitoring GP<br />
patient mortality rates. The system should be<br />
supported by a well organised, consistent and<br />
objective means of investigating those cases<br />
where a GP’s patient mortality rates signal as<br />
being above the norm.<br />
23 Every GP practice should keep a death register<br />
in which the particulars of the deaths of patients<br />
of the practice should be recorded for use in<br />
audit and for other purposes.<br />
Agree in principle and will discuss<br />
with stakeholders as part of the<br />
broader review of the Performers<br />
List system.<br />
8.10 Work is already in hand to<br />
implement this recommendation,<br />
based on the linked<br />
recommendation in the Inquiry’s<br />
Fourth Report. The intention is that<br />
every prescriber will be identified<br />
by a unique 12-digit number which,<br />
for GPs, would incorporate the<br />
GP’s unique GMC reference<br />
number while indicating the PCT<br />
and the GP practice.<br />
8.10 PCTs already routinely monitor<br />
prescribing by GPs and other<br />
prescribers. The government will<br />
invite the RCGP to work with the<br />
NHS Information Centre on how<br />
such information can best be used<br />
to assure the quality of GP<br />
services.<br />
Accepted – see the government<br />
response to the Inquiry’s 4th<br />
report, recommendation 8. For<br />
doctors, the GMC’s web based<br />
database of doctor’s registration<br />
already contains details of any<br />
restrictions on a doctor’s practice.<br />
8.12 The NHS Information Centre has<br />
developed and rolled out a Primary<br />
Care Mortality Database. We will<br />
evaluate after 12 months the<br />
extent to which this has provided<br />
useful information to PCTs. Early<br />
experience suggests that practicelevel<br />
mortality data, on its own,<br />
may only have limited use for<br />
clinical governance purposes.<br />
8.13 Accept and will be take forward<br />
with GP representatives as part of<br />
the consultation on death<br />
certification.