GBS DLL booklet 2016_Flip

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
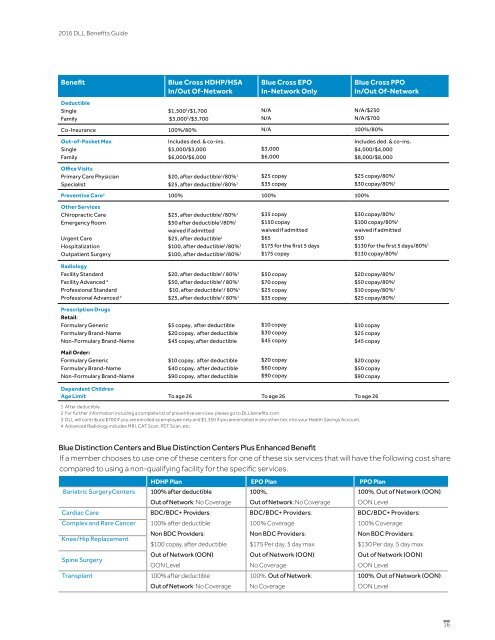
<strong>2016</strong> <strong>DLL</strong> Benefits Guide<br />
Benefit<br />
Deductible<br />
Single<br />
Family<br />
Blue Cross HDHP/HSA<br />
In/Out Of-Network<br />
$1,500 3 /$1,700<br />
$3,000 3 /$3,700<br />
Blue Cross EPO<br />
In-Network Only<br />
N/A<br />
N/A<br />
Blue Cross PPO<br />
In/Out Of-Network<br />
N/A/$230<br />
N/A/$700<br />
Co-Insurance 100%/80% N/A 100%/80%<br />
Out-of-Pocket Max<br />
Single<br />
Family<br />
Includes ded. & co-ins.<br />
$3,000/$3,000<br />
$6,000/$6,000<br />
$3,000<br />
$6,000<br />
Includes ded. & co-ins.<br />
$4,000/$4,000<br />
$8,000/$8,000<br />
Office Visits<br />
Primary Care Physician<br />
Specialist<br />
$20, after deductible 1 /80% 1<br />
$25 copay<br />
$25, after deductible 1 /80% 1 $35 copay<br />
Preventive Care 2 100% 100% 100%<br />
$25 copay/80% 1<br />
$30 copay/80% 1<br />
Other Services<br />
Chiropractic Care<br />
Emergency Room<br />
Urgent Care<br />
Hospitalization<br />
Outpatient Surgery<br />
$25, after deductible 1 /80% 1<br />
$35 copay<br />
$50 after deductible 1 /80% 1<br />
$150 copay<br />
waived if admitted<br />
waived if admitted<br />
$25, after deductible 1<br />
$65<br />
$100, after deductible 1 /80% 1 $175 for the first 5 days<br />
$100, after deductible 1 /80% 1 $175 copay<br />
$30 copay/80% 1<br />
$100 copay/80% 1<br />
waived if admitted<br />
$50<br />
$130 for the first 5 days/80% 1<br />
$130 copay/80% 1<br />
Radiology<br />
Facility Standard<br />
Facility Advanced 4<br />
Professional Standard<br />
Professional Advanced 4 $20, after deductible 1 / 80% 1<br />
$50, after deductible 1 / 80% 1<br />
$10, after deductible 1 / 80% 1<br />
$25, after deductible 1 / 80% 1 $50 copay<br />
$70 copay<br />
$25 copay<br />
$35 copay<br />
$20 copay/80% 1<br />
$50 copay/80% 1<br />
$10 copay/80% 1<br />
$25 copay/80% 1<br />
Prescription Drugs<br />
Retail:<br />
Formulary Generic<br />
Formulary Brand-Name<br />
Non-Formulary Brand-Name<br />
$5 copay, after deductible<br />
$20 copay, after deductible<br />
$45 copay, after deductible<br />
$10 copay<br />
$30 copay<br />
$45 copay<br />
$10 copay<br />
$25 copay<br />
$45 copay<br />
Mail Order:<br />
Formulary Generic<br />
Formulary Brand-Name<br />
Non-Formulary Brand-Name<br />
$10 copay, after deductible<br />
$40 copay, after deductible<br />
$90 copay, after deductible<br />
$20 copay<br />
$60 copay<br />
$90 copay<br />
$20 copay<br />
$50 copay<br />
$90 copay<br />
Dependent Children<br />
Age Limit To age 26 To age 26 To age 26<br />
1 After deductible.<br />
2 For further information including a complete list of preventive services, please go to <strong>DLL</strong>benefits.com<br />
3 <strong>DLL</strong> will contribute $700 if you are enrolled as employee only and $1,350 if you are enrolled in any other tier, into your Health Savings Account.<br />
4 Advanced Radiology includes MRI, CAT Scan, PET Scan, etc.<br />
Blue Distinction Centers and Blue Distinction Centers Plus Enhanced Benefit<br />
If a member chooses to use one of these centers for one of these six services that will have the following cost share<br />
compared to using a non-qualifying facility for the specific services.<br />
Bariatric SurgeryCenters<br />
Cardiac Care<br />
Complex and Rare Cancer<br />
Knee/Hip Replacement<br />
Spine Surgery<br />
Transplant<br />
HDHP Plan EPO Plan PPO Plan<br />
100% after deductible<br />
100%,<br />
100%, Out of Network (OON):<br />
Out of Network: No Coverage Out of Network: No Coverage<br />
OON Level<br />
BDC/BDC+ Providers:<br />
BDC/BDC+ Providers:<br />
BDC/BDC+ Providers:<br />
100% after deductible<br />
100% Coverage<br />
100% Coverage<br />
Non BDC Providers:<br />
Non BDC Providers:<br />
Non BDC Providers:<br />
$100 copay, after deductible $175 Per day, 5 day max<br />
$130 Per day, 5 day max<br />
Out of Network (OON):<br />
Out of Network (OON):<br />
Out of Network (OON):<br />
OON Level<br />
No Coverage<br />
OON Level<br />
100% after deductible<br />
100%, Out of Network:<br />
100%, Out of Network (OON):<br />
Out of Network: No Coverage No Coverage<br />
OON Level<br />
16


![GBS DLL booklet 2016_V5_EDITS[2]](https://img.yumpu.com/54825056/1/190x245/gbs-dll-booklet-2016-v5-edits2.jpg?quality=85)