

DPCA2-2_issue_v3

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Diabetes and bone health<br />
Secondary causes<br />
associated with diabetes<br />
l Coeliac disease<br />
l Graves thyrotoxicosis<br />
l Hypothyroidism<br />
l Hypogonadism<br />
l Vitamin D deficiency<br />
Anti-diabetes medication<br />
l TZDs<br />
l GLP-1 receptor agonists<br />
l DPP-4 inhibitors<br />
l SGLT2 inhibitors<br />
Falls risk<br />
l Diabetic retinopathy<br />
l Diabetic neuropathy<br />
l Obesity<br />
l Hypoglycaemia<br />
Decreased bone<br />
turnover<br />
CKD–MBD secondary to<br />
diabetic nephropathy<br />
Fracture risk<br />
Abnormal bone architecture<br />
Decreased bone mineral density<br />
via collagen cross links<br />
Decreased osteoblast differentiation<br />
Osteoblast dysfunction<br />
Increased osteoclast activity<br />
Increased adipogenesis<br />
Increased AGE<br />
Increased PPAR-gamma<br />
Decreased insulin/<br />
IGF-1 secretion<br />
Oxidative stress<br />
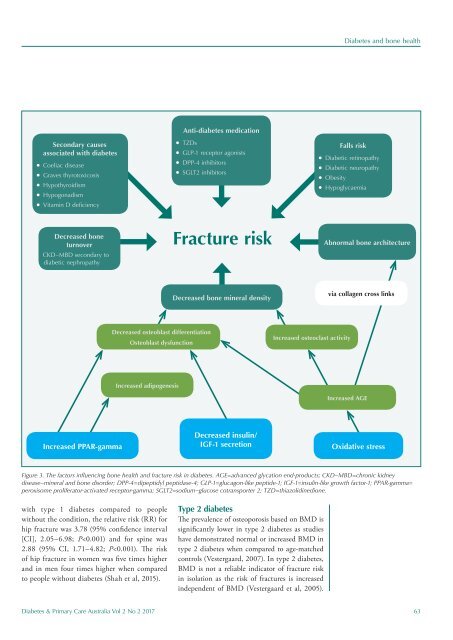
Figure 3. The factors influencing bone health and fracture risk in diabetes. AGE=advanced glycation end-products; CKD–MBD=chronic kidney<br />
disease–mineral and bone disorder; DPP-4=dipeptidyl peptidase-4; GLP-1=glucagon-like peptide-1; IGF-1=insulin-like growth factor-1; PPAR-gamma=<br />
peroxisome proliferator-activated receptor-gamma; SGLT2=sodium–glucose cotransporter 2; TZD=thiazolidinedione.<br />
with type 1 diabetes compared to people<br />
without the condition, the relative risk (RR) for<br />
hip fracture was 3.78 (95% confidence interval<br />
[CI], 2.05–6.98; P













