Editorial_lay:Layout 1 - BDIZ EDI
Editorial_lay:Layout 1 - BDIZ EDI
Editorial_lay:Layout 1 - BDIZ EDI

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
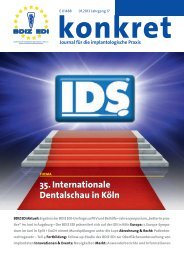
Figs. 1 to 4<br />
The clinical<br />
examination<br />
showed the<br />
precarious<br />
condition of the<br />
patients’ restorations<br />
and pronounced<br />
vertical<br />
and horizontal<br />
atrophy in both<br />
mandibular<br />
segments.<br />
1 2<br />
3 4<br />
tion consisted of complete implant-supported dentures<br />
for the maxilla and the mandible, using a computer-assisted<br />
approach to treatment planning and<br />
atraumatic surgery. The plan called for the placement<br />
of six implants each in the maxillary and mandibular<br />
arches, to be loaded immediately on placement with<br />
fixed denture prefabricated on the basis of data<br />
obtained from the SurgiGuide [12-17]. To be able to<br />
perform an atraumatic flapless procedure, it is necessary<br />
to transition through a phase with a conventional<br />
removable denture immediately after the extraction<br />
of the residual teeth, to remain in place during<br />
the entire time required for the soft tissue to heal.<br />
<strong>EDI</strong> 45<br />
Case Studies<br />
Fig. 5<br />
Baseline<br />
orthopantomograph.<br />
The patient embraced this project with enthusiasm<br />
and signed an informed consent form, and the<br />
treatment was begun immediately.<br />
The first step was a preparatory periodontal treatment<br />
to reduce the activity of periodontal disease<br />
and to improve the prognosis of the subsequent<br />
treatment steps.<br />
After four weeks and antibiotic preparation (amoxicillin<br />
3 g one hour before the procedure), we proceeded<br />
to extracting the residual maxillary teeth. The<br />
extractions were performed with the utmost caution,<br />
using the appropriate bone levers and syndesmotomes<br />
[18].