A04_Christine Meier Khan
A04_Christine Meier Khan
A04_Christine Meier Khan

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Impact of 3 different treatment approaches<br />
on arm and hand function in stroke patients<br />
- a randomized controlled trial<br />
<strong>Christine</strong> <strong>Meier</strong> <strong>Khan</strong>*, Peter Oesch*, Urs Gamper*,<br />
Jan Kool°, Serafin Beer*<br />
*Klinik Valens; °Fachhochschule Winterthur
Background<br />
Conventional neurological therapy (CNT)<br />
• Bobath/PNF, functional task-oriented training<br />
• widely used � (Kollen & Lennon 2009)<br />
Constraint induced movement therapy (CIT)<br />
• evaluated in different studies<br />
(Taub 1993, Miltner 1999, Page 2005, Wolf 2006)<br />
• high time demands<br />
mitt on the less-affected UE 14 h/d<br />
repetitive task-oriented training 6h/d<br />
� low compliance (Page 2002)<br />
Therapeutic climbing (TC)<br />
• bilateral arm training (Luft 2004, McCombe 2008)<br />
• promising results: case study<br />
• no controlled data available
Objectives & Methods<br />
• Objective: To compare the impact of<br />
� CNT<br />
� CIT<br />
� TC<br />
on arm and hand function in stroke patients.<br />
• Design: RCT with 6 months follow-up<br />
• Setting: Inpatient rehabilitation<br />
• Participants: Stroke patients with<br />
- at least minimal upper extremity function<br />
- no shoulder-pain<br />
- at least able to walk 20m<br />
• Blinded assessor at baseline, discharge, follow-up
Interventions<br />
CNT<br />
Conventional physical and occupational therapy, group<br />
therapies<br />
�Intensity: 3-4h/d<br />
CIT<br />
Constraint training in physical and occupational therapy<br />
and group therapies<br />
�Intensity: 3-4h/d, additionally 1h/d constraint self- training<br />
TC<br />
Therapeutic climbing and occupational therapy, group<br />
therapies<br />
�Intensity: 3-4h/d
Outcome measures<br />
Primary outcomes: UE-function and ADL-related use<br />
• Wolf Motor Function Test (WMFT):<br />
15 movements/ADL-tasks graded for time + quality-scale 0-5<br />
2 strength-items<br />
• Motor Activity Log (MAL): semistructured interview for<br />
- amount of use of UE: 0-5<br />
- satisfaction about use of UE: 0-5<br />
Secondary outcomes:<br />
• Shoulder-pain: subscale of Chedoke McMaster Stroke Assessm.<br />
• ROM: active shoulder flexion<br />
• Isometric strength: shoulder flex/ext, elbow flex/ext
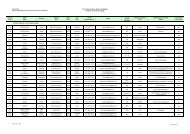
Study flowchart<br />
Not fulfilling inclusion<br />
criteria n = 237<br />
No informed consent<br />
n = 2<br />
CNT<br />
n = 15<br />
Drop out<br />
n = 1<br />
Discharge<br />
n= 14<br />
6 months follow-up<br />
n = 14<br />
All hemiplegic stroke patients<br />
n = 283<br />
Considered<br />
for randomization n = 46<br />
Randomized n = 44<br />
CIT<br />
n = 14<br />
Drop out<br />
n = 1<br />
Discharge<br />
n = 13<br />
6 months follow-up<br />
n = 13<br />
TC<br />
n = 15<br />
Discharge<br />
n = 15<br />
Drop out<br />
n = 3<br />
6 months follow-up<br />
n = 12
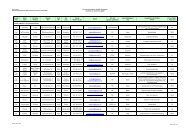
Results<br />
No significant differences between groups at baseline<br />
Significant improvement in all groups from baseline (BL) to discharge (DC)<br />
WMFTtime 58.7 ±<br />
38.6<br />
CNT n = 14 CIT n = 13 TC n = 15<br />
at BL at DC at BL at DC at BL at DC<br />
at 6 ms FU at 6 ms FU at 6 ms FU<br />
30.2 ± 37.0<br />
29.1 ± 36.3*<br />
MAL as 0.6 ± 0.7 2.2 ± 1.4<br />
2.5 ± 1.4<br />
CMSA<br />
shoulder pain<br />
6.2 ± 0.8 6.4 ± 0.8<br />
6.1 ± 1.3<br />
64.5 ± 38.4 33.0 ± 34.7#<br />
27.9 ± 29.1#<br />
1.0 ± 1.2 2.7 ± 1.6<br />
2.5 ± 1.9<br />
6.0 ± 0.8 6.4 ± 0.1 #<br />
6.9 ±0.4#∆∆∆∆<br />
51.2 ± 45.7 39.2 ±47.9<br />
37.5 ±51.4<br />
0.9 ± 1.1 2.0 ± 1.7<br />
2.5 ± 1.9<br />
6.3 ± 0.7 6.1 ± 0.9<br />
5.6 ± 1.2<br />
* Significant difference of CNT compared with TC p
Conclusions<br />
• CIT and CNT equivalent in restoring UE-function after stroke,<br />
consistent with the results of 2 reviews (Langhorne 2009, French, 2008)<br />
� 50% reduction of WMTFtime from BL to DC clinically relevant<br />
• TC with lower grade of improvement<br />
� constraint and task-oriented approach better<br />
• CIT with lower risk of shoulder pain<br />
� CIT preventing misuse? improved stabilization of shoulder?<br />
• No significant differences in strength and ROM<br />
� not determining for functional improvement<br />
• Limitations: highly selected patient group<br />
� no general conclusions for other stroke subgroups<br />
� small patient groups
This study showed, that the goal is reached best with<br />
constraint and task-oriented training.<br />
Group therapy and self-training are feasible means to<br />
provide high intensity with the available resources.<br />
Engraziel,<br />
Grazie,<br />
Merci, Danke