April_eMagazine Volume 40

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>April</strong> 2022 <strong>Volume</strong> <strong>40</strong><br />
NUVANCE HEALTH<br />
Global Health Program<br />
LARNER COLLEGE OF MEDICINE<br />
NUVANCE HEALTH AND THE UNIVERSITY OF VERMONT LARNER COLLEGE OF MEDICINE<br />
Global Health <strong>eMagazine</strong><br />
I many times thought Peace had come<br />
When Peace was far away—<br />
As Wrecked Men—deem they sight the Land—<br />
At Centre of the Sea—<br />
And struggle slacker—but to prove<br />
As hopelessly as I—<br />
How many the fictitious Shores—<br />
Before the Harbor be—<br />
-Emily Dickinson<br />
Editor; Majid Sadigh, MD<br />
Contributing Editor; Mitra Sadigh<br />
Creative Director; Amanda Wallace
OUR PEOPLE,<br />
OUR MISSION<br />
Global Health<br />
<strong>eMagazine</strong><br />
<strong>April</strong> 2022<br />
Watch this video!!<br />
Bani Adam by Saadi Shirazi<br />
HIGHLIGHTS<br />
Nuvance Health/UVMLCOM at CUGH 2022<br />
at a Glance<br />
Written by Wendi Cuscina, BS, CPM, PACT<br />
Manager of the Nuvance Health Global Health Program<br />
Nuvance Health and UVMLCOM were well-represented at this<br />
year’s Consortium of Universities for Global Health (CUGH).<br />
Members of our global health family, both domestically<br />
and internationally, headlined six poster presentations,<br />
one of which won the Best Poster Presentation award; two<br />
Highlights<br />
Perspectives<br />
Behind the Scenes<br />
Announcements<br />
Spotlight<br />
Reflections<br />
Nursing Division<br />
SARS COV-2 Pandemic<br />
and Us<br />
Dr. Mariah McNamarah (top left), professor Noeline Nakasujja (top right), professor Chiratidzo Ndhlovu (bottom left), and<br />
Mitra Sadigh (bottom right).<br />
Clinical Case Report<br />
A New Column<br />
Global Health and the Arts<br />
Articles of the Month<br />
Videos of the Month<br />
Calendar<br />
Resources<br />
reflection essays by Jett Choquette & Mitra Sadigh; a full panel discussion titled Decolonizing<br />
Global Health: The Path from Overshadowing to Illuminating; and last but not least Dr. Sadigh,<br />
recipient of the Velji Faculty Leader in Global Health Innovation Award. The Velji Family Foundation<br />
annually celebrates global health education, research, and service by honoring individuals and<br />
projects that demonstrate creative approaches to serving underserved populations.<br />
More details are presented below:<br />
The Panel<br />
Title: Decolonizing Global Health: The Path from Overshadowing to Illuminating at the Nuvance<br />
Health Global Health Program.<br />
Panelists: Mariah McNamara, Rati Ndhlovu, Noeline Nakasujja, Mitra Sadigh<br />
Organizer: Mitra Sadigh<br />
Moderator: Mariah McNamara<br />
Decolonization is the trending buzzword that not only relates to global health, but ranges into<br />
art, philosophy, beauty, garden design and education. Advocacy for decolonization begins with<br />
re-evaluating the roots of its origin, removing the imperial mindset and becoming free from<br />
colonial status. Political power and money lends itself to shadow and taint truths and views.<br />
Colonialism has a direct effect on human rights and subsequently affects access to equitable<br />
health care across the globe. “The route to achieving equity will not be accomplished through<br />
treating everyone equally. It will be achieved by treating everyone justly according to their<br />
circumstances”. Of the numerous inequities in health care around the globe, education in and<br />
2<br />
Highlights continued on next page >>
OUR PEOPLE,<br />
OUR MISSION<br />
Global Health<br />
<strong>eMagazine</strong><br />
<strong>April</strong> 2022<br />
treatment of mental health is predominant. Funding for this arena has been delinquent, however<br />
due to recent collaboration with Rudy Ruggles, Makerere University is now able to provide tuition<br />
assistance to medical students focused on mental health practices. The Nuvance Health/<br />
UVMLCOM Global Health Program is founded in empowerment by providing key components such<br />
as decision-making, resource allocation, community engagement, and capacity building.<br />
“With the haste of hopeful optimism, we might also begin to imagine that a fully decolonized<br />
global health is when there is no global health industry at all – perhaps this could be the ‘moment’<br />
of departure.”<br />
Chaudhuri MM, Mkumba L, Raveendran Y, et alDecolonising global health: beyond ‘reformative’<br />
roadmaps and towards decolonial thoughtBMJ Global Health 2021;6:e006371.<br />
Watch this video!!<br />
Bani Adam by Saadi Shirazi<br />
Highlights<br />
Perspectives<br />
Behind the Scenes<br />
Announcements<br />
Spotlight<br />
Reflections<br />
Nursing Division<br />
SARS COV-2 Pandemic<br />
and Us<br />
Clinical Case Report<br />
A New Column<br />
Global Health and the Arts<br />
Articles of the Month<br />
Videos of the Month<br />
Calendar<br />
Resources<br />
At this panel presentation, Professor Noeline Nakasujja spoke about Rudy Ruggles Global Health Scholars as an example<br />
of a program that is moving in a positive direction towards decolonization of global health.<br />
Presented Posters:<br />
1. Dynamic Nature of Medical Students’ Challenges During Clinical Global Health Elective<br />
Based on Students’ Weekly Reflections<br />
Authors: Svanjita Berry, Salwa Sadiq-Ali, Dilyara Nurkhametova, Majid Sadigh<br />
The main objective was to analyze the evolving challenges faced by medical students during<br />
a six-week global health elective, often spent at international sites where they encounter<br />
language and communication barriers, social and cultural differences and strive to understand<br />
the nuances of various healthcare systems as well as differences in local laws and regulations.<br />
Understanding these challenges allows the program to improve students’ readiness and quality<br />
of the experience. Additionally, proper preparation and appropriate setting of expectations is<br />
vital in preventing harm to the students, patients and host institution.<br />
2. The Impact of COVID-19 on Vermont’s Black, Indigenous, and People of Color (BIPOC)<br />
Population<br />
Authors: Edom Girma and Katie Wells<br />
Vermont is the nation’s most rural state with a growing racial and ethnic population. Despite<br />
this growth of minority populations, there is little evidence of the state’s efforts to explore the<br />
impact of the pandemic in these communities. Since the onset of the pandemic, the disparities<br />
in COVID-19 positive rates and COVID related deaths among the Black, American Indian,<br />
Alaskan and Hispanic populations have been well-established. Information about COVID and<br />
vaccination were found to be delinquent or non-existent in these communities. Due to the<br />
rurality of VT, the limited number of testing and vaccination sites, and the lack of available<br />
data for this population, it is suspected that a spike in cases will be seen within the next year.<br />
Public health efforts should focus on improving communications to these at risk communities.<br />
3<br />
Highlights continued on next page >>
OUR PEOPLE,<br />
OUR MISSION<br />
Global Health<br />
<strong>eMagazine</strong><br />
<strong>April</strong> 2022<br />
Watch this video!!<br />
Bani Adam by Saadi Shirazi<br />
3. The History of Colonization and its Impact on Global Health Practice: An Educational Session<br />
Authors: Mitra Sadigh, Dilyara Nurkhametova, Majid Sadigh<br />
Through a virtual elective for medical students, Nuvance Health Global Health offered a<br />
90-minute session on the history of colonization and its impact on global health practices. Mitra<br />
outlined the impact of George Floyd and the Black Lives Matter movement on restructuring this<br />
session from its standard format. How colonization affects students’ current lives and families,<br />
as well as how to combat the mindset of imperialism in today’s daily life were major points<br />
of breakout room discussions. At the conclusion of the course, the students were asked to<br />
submit their reflections and assess the course curriculum. Overwhelmingly, the students felt<br />
the course content was impactful and provided relevant cultural sensitivity awareness. The<br />
ending general consensus was that this curriculum should be an integral standard component<br />
in medical and global health studies.<br />
4. Transformation of Global Health Electives for Medical Students Amid the COVID-19 Pandemic<br />
Authors: Dilyara Nurkhametova, Bulat A. Ziganshin, Majid Sadigh<br />
Highlights<br />
Perspectives<br />
Behind the Scenes<br />
Announcements<br />
Spotlight<br />
Reflections<br />
Nursing Division<br />
SARS COV-2 Pandemic<br />
and Us<br />
Clinical Case Report<br />
A New Column<br />
Global Health and the Arts<br />
Articles of the Month<br />
Videos of the Month<br />
Calendar<br />
Resources<br />
With travel completely halted, the international experience for medical students, which is an<br />
integral part of the program, needed to quickly transform. In this light, a completely virtual<br />
online curriculum was developed. Rather than providing this elective to only 48 medical<br />
students annually, this new global health model was attended by over 800 students, with 37<br />
courses offered from the onset of the pandemic through December 2021. There was an overall<br />
positive response from students on the efficacy of this revised program.<br />
5. Global Health Narrative Medicine Elective as a Tool for Improving Cultural Competency<br />
Authors: Irene Sue, Andrea Green, et al.<br />
Winner: The Lancet – CUGH Best Student Posters – Global Health Education division…<br />
In collaboration with Dr. Andrea Green, Irene Sue took the award home for Best Poster<br />
Presentation for “Narrative Medicine in Global Health Elective: A Tool for Improving Cultural<br />
Awareness”. Irene outlined the definition, purpose, and importance of narrative medicine –<br />
which is the reiterative practice of narrative competence – to acknowledge and embrace<br />
the stories and predicaments of others. Comprehending that knowing and understanding a<br />
patient’s story, history, and the experiences have shaped their lives can allow one to be a<br />
better doctor, provider, and caregiver.<br />
Developing narrative medicine practices improves the delivery of compassionate care through<br />
increased empathy and self-awareness. With an uptick in global health electives, narrative<br />
medicine is vital to cultivating cultural awareness and improving ACGME core competencies.<br />
6. The Use of Simulation in the Training of Participants in Short-Term Global Health Electives<br />
Authors: Mitra Sadigh, Audree Frey<br />
With an increased participation in global health electives, attention has been focused on<br />
the risk of inadequate preparation to the students, patients and institution. Simulation Lab<br />
utilization has helped prepare participants to better handle the dilemmas they may encounter<br />
when traveling, including but not limited to emotional, mental, ethical, clinical, and safety<br />
challenges. Simulations were developed to improve competency in patient interaction, ethical<br />
and cultural awareness, and clinical case presentations.<br />
Summary of Nuvance Health/UVMLCOM GHP Winners at CUGH<br />
The Lancet – CUGH Best Student Posters – Global Health Education division<br />
In collaboration with Dr. Andrea Green, Irene Sue took the award home for Best Poster Presentation<br />
for “Narrative Medicine in Global Health Elective: A Tool for Improving Cultural Awareness.”<br />
“Human Experience Shaping Medical Needs” by Jett Choquette was selected for an honorable<br />
mention in the global health student category.<br />
“A Radical Act” by Mitra Sadigh was selected as a winner in the global health practitioner category.<br />
Dr. Sadigh was the recipient of the Velji Faculty Leader in Global Health Innovation Award. The<br />
Velji Family Foundation annually celebrates global health education, research, and service by<br />
honoring individuals and projects that demonstrate creative approaches to serving underserved<br />
populations.<br />
4
OUR PEOPLE,<br />
OUR MISSION<br />
Global Health<br />
<strong>eMagazine</strong><br />
<strong>April</strong> 2022<br />
Watch this video!!<br />
Bani Adam by Saadi Shirazi<br />
PERSPECTIVES<br />
Decolonizing Global Health: The Past, Present and<br />
the Future-Staff Exchanges<br />
From a panel presentation at CUGH<br />
Written by<br />
Prof Chiratidzo E Ndhlovu, M Med Sci( Clin Epi), FRCP<br />
University of Zimbabwe Faculty of Medicine and Health<br />
Sciences<br />
Decolonizing Global Health: The Past, Present and the Future-<br />
Staff Exchanges<br />
If decolonizing global health is about achieving equity and<br />
justice, how do we get there, especially when it comes to our<br />
academic global health partnerships?<br />
Highlights<br />
Perspectives<br />
Behind the Scenes<br />
Announcements<br />
Spotlight<br />
Reflections<br />
Nursing Division<br />
SARS COV-2 Pandemic<br />
and Us<br />
Clinical Case Report<br />
A New Column<br />
Global Health and the Arts<br />
Articles of the Month<br />
Videos of the Month<br />
Calendar<br />
Resources<br />
How do we decolonize global health when those delivering healthcare in the Global South are<br />
trained in “western medicine”(Kulesa J, Brantuo NA, BMJ Global Health 2021) and will have their<br />
health outcomes judged using the Global North perspective? How do we decolonize global health<br />
if Global South countries/academic institutions do not fund the activities that constitute global<br />
health?<br />
We in the Global South are part of this globalized world. But should we be judged the same way<br />
as our colleagues/ clinicians in the Global North or “developed world”? We all acknowledge that<br />
the playing field is not yet level, but how do we level it? If we are able to, there will be no need for<br />
global health as currently practiced. The Global South is viewed as needing help. Hence we have<br />
the current global health collaborations framework or format. Why should those with resources<br />
level out the playing field, as it will take away their jobs!<br />
Decolonization in academic institutions is challenging as it is supposed to be between “foreign<br />
global health practitioners and indigenous clinicians trained in western medicine” (Kulesa J, Brantuo<br />
NA, BMJ Global Health 2021). How can local clinicians look at health in their setting without the<br />
foreigners’ lens if they were trained to deliver healthcare using their “western medicine” training?<br />
Global Health Collaborations at Academic Institutions<br />
In academia, we are also on the receiving end of what our partners need for their training programs,<br />
be it at faculty or student level. The aim of course is to build bidirectional relationships. How can we<br />
build relationships that demonstrate equity and social justice?<br />
Our partners need exposure to a different culture/healthcare setting as part of their growth and<br />
training. What do we get in turn? We also get exposure to a different culture and healthcare setting,<br />
however our Global North partners can “touch” our patients while we can only be observers! We<br />
are given the opportunity to visit their institutions as observers and marvel at the technologies<br />
being used to deliver healthcare such as the wide use of computers and robots—technologies that<br />
we will not be able to use in our settings in the foreseeable future.<br />
When we return to our institutions after fulfilling our side of the global health partnerships, we<br />
become disillusioned with our work settings. If we are lucky, we are likely offered work out there<br />
in the Global North, and may even actively seek research such opportunities. We run the risk of<br />
abandoning our country as the grass looks greener elsewhere i.e getting poached or “braindrained”!<br />
For senior clinicians, our Global North partners can easily get jobs in the Global South while<br />
we cannot easily obtain clinical jobs or even faculty positions in the Global North! Are we selfstigmatizing<br />
ourselves, or is that just the way global health has operated? Will it continue to<br />
operate in this fashion, or is there really hope for change?<br />
5<br />
Perspectives continued on next page >>
OUR PEOPLE,<br />
OUR MISSION<br />
If we do get out to the Global North, does that mean our global health partnerships have been<br />
successful or is this is how brain drain starts, especially regarding our young faculty members? After<br />
all, they have families to fend for. If we do manage to keep them in the country, they are likely to get<br />
swept away by international NGOs/partners and will then advocate for other people’s agenda!<br />
That will continue to perpetuate our colonization.<br />
Global Health<br />
<strong>eMagazine</strong><br />
<strong>April</strong> 2022<br />
Watch this video!!<br />
Bani Adam by Saadi Shirazi<br />
Global Health Visits by Faculty Members - GH Partnerships<br />
Do these GH visits encourage colonization? How can they contribute to decolonizing global health?<br />
Our partners (faculty or students) from the Global North can be more than “observers.” They are<br />
allowed to practice in our settings even if they come in “culturally incompetent.” But how about<br />
those of us coming from the South to the North?<br />
We are unlikely to be allowed to practice as we will not be licensed to “touch” patients. What<br />
will it take to allow us, even our most senior or most clinically competent practitioners to work<br />
clinically in the Global North? How long will it take to allow us to be more than just “observers” of<br />
the healthcare delivery process?<br />
Though UVMLCOM faculty members “following up” their students relieves locals from being<br />
responsible for visiting students, does it perpetuate the colonial mindset by continuing to give the<br />
impression that local practitioners are not qualified to teach visiting students?<br />
Highlights<br />
Perspectives<br />
Behind the Scenes<br />
Announcements<br />
Can we expect Global South faculty to “follow up” their students? i.e. just the same way UVM<br />
faculty were expected to supervise, albeit for a very short period, their students visiting our sites?<br />
The Global North now has clinical skills laboratories with high-fidelity mannequins that will cry if you<br />
hurt them, so we can perhaps be trusted to handle those mannequins but not real human beings!<br />
We also do not want to be sued for not delivering appropriate medical practice. We cannot afford<br />
to have litigation against us. We cannot even afford to subscribe to the most prestigious journals<br />
let alone be well-insured to “touch” patients.<br />
Spotlight<br />
Reflections<br />
Nursing Division<br />
SARS COV-2 Pandemic<br />
and Us<br />
Clinical Case Report<br />
A New Column<br />
Global Health and the Arts<br />
Articles of the Month<br />
Videos of the Month<br />
Calendar<br />
Resources<br />
How long will it take for equity to be achieved in global health partnerships between teaching<br />
institutions? Is it even possible? It is probably unlikely in the foreseeable future as the world<br />
continues to be so divided class-wise – “developed” versus “developing” countries.<br />
Most times we undertake programs because someone has offered or is prepared to fund those<br />
programs.Those problems that have no obvious funds dangled in front of us are not prioritized.<br />
Are we in this predicament because we have not taken responsibility for our healthcare delivery<br />
as countries in the Global South?<br />
If we do not put adequate money into our Ministries of Health we will be at the mercy of those<br />
who think they know what we need and then provide it, be it faculty visits, student visits, or<br />
research funding to make up for the gaps in our skills as we deliver health care. When will those of<br />
us in the Global South or “developing world” be the agenda setters? What will equity and justice<br />
in global health look like in the short-term or even mid-term?<br />
6
OUR PEOPLE,<br />
OUR MISSION<br />
Global Health<br />
<strong>eMagazine</strong><br />
<strong>April</strong> 2022<br />
Watch this video!!<br />
Bani Adam by Saadi Shirazi<br />
In Conclusion, What Does “Decolonizing Global Health” Mean?<br />
Do we need to agree that this is the way it is and it is unlikely to change for the foreseeable future?<br />
Perhaps “decolonizing global health” will remain an academic debate with few tangible changes.<br />
The best we can do for now is accept that the world has created a colonized global health but<br />
continue to discuss the uncomfortable truths just as the Black Lives Matter and Me-too movements<br />
have done. We could look at this problem as a puzzle to be solved bit by bit.<br />
I feel we have a long way to go to equalizing the playing field. These discussions should help us all<br />
be aware of the elephant in the room. I have no solutions to offer besides agreeing that discussing<br />
these issues has been a great start over the past decade or so.<br />
Besides, he who pays the piper calls the tune!<br />
Decolonizing Global Health: The Past, Present and the Future-Staff Exchanges<br />
Highlights<br />
Perspectives<br />
Behind the Scenes<br />
Announcements<br />
Spotlight<br />
Reflections<br />
Nursing Division<br />
SARS COV-2 Pandemic<br />
and Us<br />
Clinical Case Report<br />
A New Column<br />
Global Health and the Arts<br />
Articles of the Month<br />
Videos of the Month<br />
Calendar<br />
Resources<br />
Saida agliullina (Kazan)<br />
7<br />
Perspectives continued on next page >>
OUR PEOPLE,<br />
OUR MISSION<br />
Global Health<br />
<strong>eMagazine</strong><br />
<strong>April</strong> 2022<br />
Watch this video!!<br />
Bani Adam by Saadi Shirazi<br />
“Decolonizing Global Health: The Path from Overshadowing to Illuminating”<br />
Mitra Sadigh<br />
Watch the video here >><br />
Highlights<br />
Perspectives<br />
Behind the Scenes<br />
Announcements<br />
Decolonization of Global Health<br />
The Winning Essay at CUGH<br />
“A Radical Act”<br />
Written by Mitra Sadigh<br />
Spotlight<br />
Reflections<br />
Nursing Division<br />
SARS COV-2 Pandemic<br />
and Us<br />
Clinical Case Report<br />
A New Column<br />
Global Health and the Arts<br />
Articles of the Month<br />
Videos of the Month<br />
Calendar<br />
Resources<br />
It was June 2020. Six months into a global pandemic. Just<br />
weeks following the murder of George Floyd. The height of the<br />
Black Lives Matter protests. Our Global Health Program was<br />
finding a new home in the virtual sphere. I had claimed two<br />
sessions of our two-week elective to discuss cultural relativity<br />
and humility. The course was carefully crafted in an attempt to<br />
recreate the global health environment; that moment when a<br />
person, through interacting with a different culture and way of<br />
life, excavates their own privileges and beliefs and perhaps for<br />
the first time, questions them.<br />
Our nation was tearing at seams that have always existed but have never appropriately been<br />
acknowledged. That Friday morning, a student opened our class discussion with a few questions I<br />
could not have prepared myself for.<br />
Did Christopher Columbus arrive in the New World in peace, but couldn’t communicate his intentions<br />
because of the language barrier?<br />
Were slaves in the United States unable to own land because they weren’t educated in how to<br />
own land?<br />
Did slaves not know they were being oppressed because they weren’t educated?<br />
The virtual room fell silent. I had never heard anyone ask these kinds of questions. I was not aware<br />
that anyone had these kinds of questions.<br />
I responded the best I could in the moment.<br />
No, the issue with Christopher Columbus was not the language barrier. Peace is offered through<br />
actions, not words.<br />
Slaves couldn’t own land because they were oppressed.<br />
8<br />
Perspectives continued on next page >>
OUR PEOPLE,<br />
OUR MISSION<br />
Global Health<br />
<strong>eMagazine</strong><br />
<strong>April</strong> 2022<br />
Watch this video!!<br />
Bani Adam by Saadi Shirazi<br />
No, a person does not require an education to know that they are being oppressed.<br />
Every human being knows when they are subjected to injustice.<br />
A few students chimed in—to help me, to help this questioning student, to help their own sense of<br />
helplessness. To help our colleagues of color in the virtual room.<br />
The session left me reeling. At first I blamed myself for being unprepared—I should have known<br />
that our national reckoning would seep through the screen. Later, I blamed our education system<br />
for allowing a student to make it so far without a basic understanding of history. I then blamed our<br />
medical education system for allowing a student to enter clinical care without understanding this<br />
continuing history that impacts countless peers, colleagues, and patients. The thought evolved<br />
over the weeks to follow. I harnessed the only thing in this cascade that I could control: ensuring<br />
students completed our global health elective having been exposed to this understanding. The<br />
next cycle, I taught a new course: Colonization and Global Health—a delving into the ways colonization<br />
has and continues to create inequity, and the pervasiveness of the colonial mindset in<br />
today’s global health sphere.<br />
As it turns out, this is not an easy thing to teach. One student’s takeaway was that colonization<br />
was not as successful elsewhere as it was in the United States. Despite grave human rights violations,<br />
it was worth it because the nation is one of the world’s greatest superpowers today. Other<br />
students have begun the course perplexed by the connection between colonization and global<br />
health, and completed it with the two concepts only slightly more reciprocal.<br />
Highlights<br />
Perspectives<br />
Behind the Scenes<br />
Announcements<br />
Spotlight<br />
Reflections<br />
Nursing Division<br />
SARS COV-2 Pandemic<br />
and Us<br />
Clinical Case Report<br />
A New Column<br />
Global Health and the Arts<br />
Articles of the Month<br />
Videos of the Month<br />
Calendar<br />
But the overall response has moved me. Many students feel catharsis in sharing their personal<br />
experiences with colonization. Relief in connecting with others in shared perspectives. Elucidation<br />
in naming the traumas that affect them every day more clearly than before. Awe as they start to<br />
observe their world through a new lens. Shock, even indignation for the false narratives they had<br />
been taught previously—from the media, from teachers, from textbooks, from culture. Guilt and<br />
shame in the reality they didn’t see before. One student applauded my efforts in “sharing truths<br />
that were direct and arguably radical.” I am still sitting with the question of why speaking the truth<br />
is a radical act.<br />
Do people in low-to-middle income countries (LMICs) not know they are getting the short end of<br />
the economic, resource, and life expectancy stick because they are not educated?<br />
Do people in LMIC have lesser access to resources because they’re “not educated” in how to use<br />
those resources?<br />
Do people from high-income countries (HICs) come to LMICs with well-intentioned solutions, but<br />
are misunderstood as having a colonially-rooted savior complex?<br />
Global health experiences on-the-ground are capable of overturning these same fallacies, but<br />
with greater harm to host communities. It is the learning of a student from a HIC at the expense of<br />
a person in a LMIC, much like the students of color that day who were teaching the white student<br />
about the awareness that intrinsically arises within the oppressed.<br />
We cannot provide the breadth and depth of a global health experience in the virtual sphere<br />
any more than we can craft the nuanced, personalized lessons that a student on a global health<br />
elective would be faced with. But we can provide them with a platform on which to question how<br />
inequality came to be before they rush in to help fight it. We can encourage them to investigate<br />
the ways harmful legacies continue to propagate through our subconscious and the systems<br />
from which many of us benefit. We can awaken them to the abuse and mistrust from which global<br />
health emerged and currently inhabits so that they may someday truly connect with the populations<br />
they feel compelled to serve.<br />
“A Radical Act” Mitra Sadigh<br />
Resources<br />
9<br />
Perspectives continued on next page >>
OUR PEOPLE,<br />
OUR MISSION<br />
Global Health<br />
<strong>eMagazine</strong><br />
<strong>April</strong> 2022<br />
Watch this video!!<br />
Bani Adam by Saadi Shirazi<br />
Highlights<br />
Perspectives<br />
Behind the Scenes<br />
Announcements<br />
Spotlight<br />
Reflections<br />
Nursing Division<br />
SARS COV-2 Pandemic<br />
and Us<br />
Clinical Case Report<br />
A New Column<br />
Global Health and the Arts<br />
Articles of the Month<br />
Videos of the Month<br />
Calendar<br />
Resources<br />
2021 Report from the Desert: “Borderlands<br />
Infectious Disease Prevention Program”<br />
Written by Jonathan Melk MD FAAP<br />
CEO, Chiricahua Community Health Centers, Inc,<br />
Douglas, Arizona<br />
Since 1996, Chiricahua Community Health Centers, Inc. (CCHCI)<br />
has provided primary care to the diverse communities and<br />
special populations of Cochise County as the region’s only<br />
Federally Qualified Health Center (FQHC). Cochise County is<br />
an area the size of Connecticut and Rhode Island combined<br />
(including one hundred miles of the U.S./Mexico border), and<br />
both geographic isolation and prevalence of poverty makes<br />
preventive and primary health care inherently complex and<br />
challenging. All of Cochise County is designated as a Health<br />
Professional Shortage Area. CCHCI is uniquely positioned to respond to these challenges via a<br />
team of <strong>40</strong>0 highly trained employees and an extensive network of both fixed site and mobile<br />
clinics that currently cares for over 30,000 patients. As a FQHC, CCHCI provides culturally<br />
competent care and does not turn any patient away based on ability to pay or insurance status.<br />
In 2016, a case of dog tick-born Rocky Mountain Spotted Fever (RMSF) was missed by an astute<br />
Chiricahua pediatrician in our pediatric clinic (located just blocks from the US/Mexico border)<br />
in Douglas. RMSF is an unusual diagnosis for our region and was not on this pediatrician’s<br />
differential. RMSF can be fatal to children, particularly when there is a delay in diagnosis and<br />
treatment. Although this child survived and is now well, he required an extensive stay in a Tucson<br />
intensive care unit. Shortly after learning about this case, a CDC field officer traveled to Cochise<br />
County to provide education to CCHCI medical providers to better recognize and promptly treat<br />
this ‘rare’ and ‘unexpected’ diagnosis. However, ironically, a coincidental conversation between<br />
a CCHCI staff member and a Mexican doctor soon revealed just how little American and Mexican<br />
health colleagues communicate and how dangerous this shortcoming is for border communities.<br />
At the time of the RMSF case that was presented to our clinic, Agua Prieta (the sister city on<br />
the other side of the Douglas border wall) had dozens of cases of RMSF, with multiple pediatric<br />
deaths. This unfolding and deadly epidemic was entirely unknown to CCHCI, to the county health<br />
department and apparently to the CDC. Had CCHCI been alerted, it would have been less likely<br />
for this child to suffer from an illness that is otherwise curable with a common antibiotic when<br />
promptly treated.<br />
Following this revelation and close call, CCHCI proactively worked with the Mexican Consulate<br />
to set up tours and meetings between CCHCI and Mexican medical leadership and colleagues.<br />
We hosted them and they hosted us. A Whatsapp group resulted and continues in use to this<br />
day. With this minimal leadership effort, multiple patient collaborations have since developed<br />
to better manage individual patients who were deported to Mexico, who now live in the United<br />
States, or who utilize medical services on both sides of the border. However, despite our creative<br />
and practical approach, this effort is limited in its application and results, as exhibited by the<br />
disparities in the current Covid-19 illness and death on both sides of the border as compared to<br />
Arizona as a whole. It also doesn’t address the reality that no matter what laws are passed by<br />
either nation, ticks, mosquitos, vermin and other vectors don’t stop for Customs checkpoints or a<br />
border wall. Epidemiologically, border communities are one single community, and the reality is<br />
that Cochise County, Arizona and Sonora, Mexico are separated only by a metal barrier and two<br />
different political systems.<br />
To address this challenge, CCHCI wrote for and received a grant from the global nonprofit<br />
Direct Relief through funding from the Pfizer Foundation. The goal of the grant is to establish a<br />
“Borderlands Infectious Disease Prevention Program”. Over the two-year grant period, CCHCI<br />
is working to build a robust and sustainable infectious disease surveillance, prevention and<br />
treatment program guided by both external and internal data that will incorporate all of CCHCI<br />
delivery sites and staff. The program will incorporate collaboration with both Mexican and United<br />
States public health entities. This data-based program will establish consultation and oversight<br />
by CCHCI clinicians as well as regional infectious disease and public health experts from both<br />
sides of the border. Finally, CCHCI will seek to document, publish, and present our approach and<br />
outcomes for other border communities (on the US/Mexico border or elsewhere) to learn from<br />
and to replicate.<br />
10
OUR PEOPLE,<br />
OUR MISSION<br />
Global Health<br />
<strong>eMagazine</strong><br />
<strong>April</strong> 2022<br />
Watch this video!!<br />
Bani Adam by Saadi Shirazi<br />
BEHIND THE SCENES<br />
Written by<br />
Marty Scholand in recognition of Sally Yelland<br />
and Dr. Stephen Scholand<br />
As we learned with Covid, there was no quick way to end<br />
its scourge. It took many months to learn how to best deal<br />
with the many proposed solutions that we were offered<br />
and determine which were truly effective. Sometimes both<br />
medicine and politics are not exact sciences.<br />
With the following comments, I would like to express my<br />
sympathy for a great loss to me and the Global Health<br />
Program and share what sometimes happens behind-thescenes.<br />
Highlights<br />
Perspectives<br />
Behind the Scenes<br />
Announcements<br />
Spotlight<br />
Reflections<br />
Nursing Division<br />
SARS COV-2 Pandemic<br />
and Us<br />
Clinical Case Report<br />
A New Column<br />
Global Health and the Arts<br />
Articles of the Month<br />
Videos of the Month<br />
Calendar<br />
Resources<br />
Most of you have never heard of a wonderful lady named Sally Yelland from Hanover, PA as she<br />
never sought notoriety. She was a simple yet complex woman who had a close circle of friends of<br />
whom I was proud to be one of. If you saw her at work or the grocery store, you would never know<br />
she was well-off. But if you ever ate a “Snyder’s of Hanover” pretzel or a “Lance Cracker,” you were<br />
connected to her.<br />
A few years ago, before Covid, my nephew Dr. Stephen Scholand of the Global Health Program<br />
asked if I would help raise money for a project he was working on in a hospital in Zimbabwe.<br />
While I was retired and a bad golfer, not a fund raiser, I attempted to raise some money through<br />
my small 100-year-old rural Country Club. How can you say no to the family doctor? I arranged<br />
for an upscale banquet and invited people I thought might donate more than I was paying<br />
for the dinner. My goal was to raise $8,000 to $10,000. I had about fifty friends agree to come<br />
knowing it was going to cost them. Dr. Scholand delivered a thirty-minute presentation which<br />
induced many of them to open their checkbooks. I was pleased that we raised almost $12,000<br />
by the end of dinner. In my mind, it was a remarkable success.<br />
When I got home that evening, I received a call from Sally asking if it was okay for her to send me<br />
an additional check as she was inspired by Steve’s presentation and felt she wanted to do more.<br />
People often want to do more but I did not know what “more” might mean. She must have driven<br />
to the post office that night as on Monday morning I found a check in the mailbox for around<br />
$20,000 to add to my total for the Global Health Program. It brought tears to my eyes as I went into<br />
the house and showed my wife Connie who worked through the exhausting project with me. We<br />
significantly exceeded our goal.<br />
I was honored at a Global Health Program dinner for raising funds, but a scant few knew where the<br />
over-the-top success of the program came from. It was Sally Yelland. She was well-known in local<br />
circles as a supporter of hospital and historical causes. But a hospital on another continent—who<br />
knew? In February 2022, I was saddened to learn that Sally suddenly passed away in just two days.<br />
A loss to the community and to me.<br />
For that reason, I wanted<br />
to direct my sympathy to<br />
her family and express<br />
my gratitude for being<br />
able to know and<br />
collaborate with her.<br />
Dr. Stephen Scholand<br />
visited again to thank her<br />
personally. To the right is<br />
a picture from the dinner<br />
we shared with Sally and<br />
her Husband Sidney.<br />
God bless her! The world<br />
could use more people<br />
like her.<br />
11
OUR PEOPLE,<br />
OUR MISSION<br />
Global Health<br />
<strong>eMagazine</strong><br />
<strong>April</strong> 2022<br />
Watch this video!!<br />
Bani Adam by Saadi Shirazi<br />
ANNOUNCEMENTS<br />
The following panel has been accepted for a 120-minute virtual presentation at the United<br />
Nation General Assembly (UNGA), Science Summit September 2022<br />
Creating an Empowerment Model in Global Health: An Evolving Practice to<br />
Build Capacity, Research Methodologies, Educational Modalities, and Health<br />
Equity<br />
Organizer and Moderator<br />
Majid Sadigh, MD<br />
Director of the Nuvance Health (NH) / University of Vermont Larner College of Medicine<br />
(UVMLCOM) Global Health Program, Christopher J. Trefz Family Endowed Chair in Global<br />
Health at NH.<br />
Panelists<br />
Robert Kalyesubula, MD, PhD<br />
Highlights<br />
Perspectives<br />
Behind the Scenes<br />
Announcements<br />
Spotlight<br />
Reflections<br />
Nursing Division<br />
SARS COV-2 Pandemic<br />
and Us<br />
Clinical Case Report<br />
A New Column<br />
Global Health and the Arts<br />
Articles of the Month<br />
Videos of the Month<br />
Calendar<br />
Resources<br />
Assistant professor MakCHS, Founder of the African Community Center for Social Sustainability<br />
(ACCESS), Uganda<br />
Chiratidzo E Ndhlovu, M Med Sci( Clin Epi), FRCP<br />
Deputy Dean of the University of Zimbabwe College of Health Science, Associate Professor<br />
in the Department of Medicine<br />
Marcos Núñez, MD, FICS, M.Ed<br />
Dean of Health Sciences at Universidad Iberoamericana, Dominican Republic<br />
Syed Zahiruddin Quazi, MD, PhD<br />
Director, Directorate of Research & Development, Professor of Community Medicine at DMIMS,<br />
India.<br />
Mitra Sadigh<br />
Writer, Editor, and Researcher at the Nuvance Health/University of Vermont Larner College<br />
of Medicine and MD candidate at the Stony Brook University Renaissance School of Medicine<br />
Vincent Setlhare<br />
Head of the Department of Family Medicine and Public Health, University of Botswana,<br />
Botswana<br />
The colonizer mindset is alive and continuing to ripple through academia, educational institutions,<br />
healthcare centers, and communities. Rooted in an empowerment rather than dependency model,<br />
the Nuvance Health / University of Vermont Larner College of Medicine Global Health Program<br />
with active participation from domestic and international partners has gradually implemented<br />
unique features from decision-making to resource allocation, participant education to community<br />
engagement, capacity building to brain gain. We aim to shed a truthful light on a tragic past and<br />
present while evaluating our program’s components that combat and contribute to the savior<br />
complex model.<br />
During this session, a group of global health experts share their insights by citing examples of<br />
successes, failures, and challenges in their partnerships with the Global North. Learning objectives<br />
include an understanding of the colonial mindset in global health; the ways it weaves into global<br />
health programs administratively, pedagogically, and in clinical practice; its impact on the wellbeing<br />
of host institutions, patients, and communities; the steps our program has taken toward<br />
decolonization, including creation of a Global South-led taskforce and a Global South-Global<br />
South empowerment model; and ways the program hopes to grow. Examples of reverse learning<br />
and reverse innovations will be discussed.<br />
12<br />
Announcements continued on next page >>
OUR PEOPLE,<br />
OUR MISSION<br />
Global Health<br />
<strong>eMagazine</strong><br />
<strong>April</strong> 2022<br />
Watch this video!!<br />
Bani Adam by Saadi Shirazi<br />
In reflection of today’s social and cultural atmosphere, the field of global health is calling for<br />
a reckoning of its colonial past. The topic of “decolonizing” global health is a highly relevant<br />
investigation. Histories of slavery, redlining, environmental racism and the predatory nature<br />
of capitalism underpin the design of global and public health systems, resulting in structural,<br />
racial and ethnic inequities within Black, Indigenous and People of Color (BIPOC) communities<br />
globally. There are many who call for a shift in the paradigm of global health and label this as a<br />
“decolonization,” where a critical eye is cast on the history of global health and shift its structure<br />
and administration, removing any repressive motives of colonial control.<br />
By a critical account of where the Nuvance Global Health Program stands in this respect, we believe<br />
it can make its mark in global health by providing a potential blueprint for mutually dependent<br />
programs. More importantly, giving the podium to partners from LMIC to discuss their perspective<br />
may open new dialogues toward more equitable, justified, and transparent partnerships. We<br />
review the changes of our program over the past decade in hope of delivering a better global<br />
health partnership between domestic institutions and institutions in LMIC.<br />
There is no question that we have a long way to go to equalize global health. However, transparent,<br />
respectful discussions among colleagues such as those in this panel is a critical step forward<br />
toward equity and justice.<br />
Highlights<br />
Perspectives<br />
Behind the Scenes<br />
Announcements<br />
Spotlight<br />
Reflections<br />
Nursing Division<br />
SARS COV-2 Pandemic<br />
and Us<br />
Clinical Case Report<br />
A New Column<br />
Global Health and the Arts<br />
Articles of the Month<br />
Videos of the Month<br />
Calendar<br />
Resources<br />
13
OUR PEOPLE,<br />
OUR MISSION<br />
SPOTLIGHT<br />
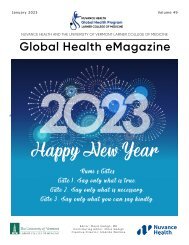
“Global Health on the Farm”: Another Potential Domestic Site<br />
Global Health<br />
<strong>eMagazine</strong><br />
Written by Stephen Scholand, MD<br />
Associate Director of Nuvance Global Health Program<br />
<strong>April</strong> 2022<br />
Watch this video!!<br />
Bani Adam by Saadi Shirazi<br />
Highlights<br />
Perspectives<br />
Behind the Scenes<br />
Announcements<br />
Spotlight<br />
Reflections<br />
Nursing Division<br />
SARS COV-2 Pandemic<br />
and Us<br />
Clinical Case Report<br />
Norm Beatty, MD<br />
UF Health, Florida<br />
On March 11, 2022, Dr. Stephen Scholand<br />
met with Dr. Norm Beatty at the University<br />
of Florida in Gainesville to explore the<br />
potential for a new partnership in global<br />
health education. A suggested collaborative<br />
program called Global Health on the Farm<br />
was discussed. Currently, it is estimated that<br />
about 200,000 immigrant farm workers from<br />
Mexico and elsewhere in Central America are<br />
relied upon to harvest fruits and vegetables<br />
from the vast farm areas of Florida.<br />
Strawberries, cucumbers, tomatoes, and of<br />
course citrus crops rely upon this workforce.<br />
Communities of these immigrant workers are<br />
housed locally and transported en masse<br />
every day to perform the backbreaking work<br />
of harvesting.<br />
Until recently, there hasn’t been much<br />
attention focused on the health of these<br />
workers. Dr. Beatty and his team have begun<br />
a series of volunteer-based efforts focused<br />
on health screening, health education,<br />
immunizations, and establishment of care<br />
with local health resources and charities.<br />
The partnership offers the chance for an<br />
authentic global health experience, as the<br />
workers come from various areas within<br />
Central America with their own languages<br />
and customs. Of course the health needs<br />
are great, as often is found in this field. This<br />
new initiative promises to be a rich learning<br />
experience for medical students and a<br />
significant benefit to the workers. We look<br />
forward to growing this partnership in the<br />
coming months.<br />
A New Column<br />
Global Health and the Arts<br />
Articles of the Month<br />
Videos of the Month<br />
Calendar<br />
Resources<br />
Dr. Norm Beatty (left) and Dr. Stephen Scholand (right)<br />
14<br />
Spotlight continued on next page >>
OUR PEOPLE,<br />
OUR MISSION<br />
Global Health<br />
<strong>eMagazine</strong><br />
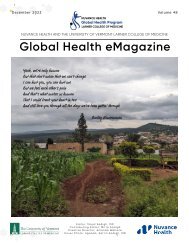
Rudy Ruggles Scholars in Global Mental Health<br />
On March 13th during a Zoom meeting with Professor Noeline Nakasujja, Head of MakCHS<br />
Psychiatry Department; Dr. Dickens Akena, MakCHS Psychiatry Department; Dr. Judith Lewis,<br />
Director of the UVMLCOM Resident Training Program; Majid Sadigh, Director Nuvance Health/<br />
UVMLCOM GHP; and Ms. Susan Byekwaso, Coordinator of international Programs at MakCHS,<br />
the MakCHS psychiatry residents Dr. Agaba Denis, Dr. Wamala Denis, and Dr. Penelope-Emma<br />
Tukasingura Kiremire were awarded Rudy Ruggles Global Mental Health Scholarships.<br />
<strong>April</strong> 2022<br />
Watch this video!!<br />
Bani Adam by Saadi Shirazi<br />
Highlights<br />
Perspectives<br />
Dr. Penelope-Emma Tukasingura<br />
Kiremire<br />
Dr. Wamala Denis (left), Dr. Agaba Denis (right)<br />
Behind the Scenes<br />
Announcements<br />
Spotlight<br />
Reflections<br />
Nursing Division<br />
SARS COV-2 Pandemic<br />
and Us<br />
Clinical Case Report<br />
A New Column<br />
Global Health and the Arts<br />
Articles of the Month<br />
Videos of the Month<br />
Calendar<br />
Resources<br />
Saida agliullina (Kazan)<br />
15<br />
Spotlight continued on next page >>
OUR PEOPLE,<br />
OUR MISSION<br />
Global Health<br />
<strong>eMagazine</strong><br />
<strong>April</strong> 2022<br />
Watch this video!!<br />
Bani Adam by Saadi Shirazi<br />
Highlights<br />
Perspectives<br />
Behind the Scenes<br />
Announcements<br />
Spotlight<br />
Letter from Dr. Jonathan Melk<br />
CEO, Chiricahua Community Health Centers, Inc,<br />
Douglas, Arizona<br />
Following the binational infectious disease meeting today, I had<br />
the opportunity to meet with Dr. Brianda Gonzalez Gutierrez, the<br />
epidemiologist for the General Hospital of Agua Prieta (GHAP). Dr.<br />
Gonzalez has been in her post for 14 years and thus has been a<br />
stable, enthusiastic and knowledgeable presence and partner for<br />
CCHCI.<br />
For years until 2008, the University of Arizona sent students to<br />
GHAP for experiential learning. Activities included shadowing<br />
the work of inpatient, outpatient and community work, including<br />
shadowing with community health workers. She believes that<br />
the GHAP would be open and interested in collaborating with<br />
Chiricahua and UVMLCOM students. In brainstorming with her, I<br />
tossed out the idea of eight students per year—the number we<br />
thought we could handle). As each has about a one-month rotation, I thought perhaps they could<br />
spend ten days in Mexico: around 50% in the hospital and 50% in the community. She liked that<br />
idea, but is definitely open for discussion.<br />
To ensure that there is some sort of tangible benefit for the Mexican team, we spoke about the<br />
needs of the hospital and its services. In short, likely the best way that UVMLCOM could assist<br />
would be in funding equipment and material needs, as any transfer of cash would likely need to<br />
go to the state and GHAP wouldn’t likely see the benefits of that despite doing all of the work. For<br />
instance, the hospital doesn’t currently have a working x-ray machine. They also don’t have enough<br />
anesthesia setups, and those that they do have are rented. I would like to see if the UVMLCOM/<br />
Nuvance relationship could bring not only opportunities for their students as well as CCHCI, but<br />
also opportunities for our Mexican colleagues and their patients.<br />
In summary, it appears very promising that CCHCI could set up an exceptional global health<br />
rotation that would be a win/win/win for UVMLCOM students, CCHCI, and our Mexican partners.<br />
Attached is a recent article regarding our budding binational work to address infectious disease<br />
(just to start).<br />
Reflections<br />
Nursing Division<br />
SARS COV-2 Pandemic<br />
and Us<br />
Clinical Case Report<br />
A New Column<br />
Global Health and the Arts<br />
Articles of the Month<br />
Videos of the Month<br />
Calendar<br />
Resources<br />
https://www.elpasotimes.com/story/news/2022/03/24/covid-arizona-sonora-mexico-borderdoctors-chiricahua-clinic-infectious-disease/6943332001/<br />
16<br />
Spotlight continued on next page >>
OUR PEOPLE,<br />
OUR MISSION<br />
Global Health<br />
<strong>eMagazine</strong><br />
<strong>April</strong> 2022<br />
Watch this video!!<br />
Bani Adam by Saadi Shirazi<br />
Mulago Hill, Uganda: Flight to the Moon<br />
Written by Hossein Akbarialiabad, MDMSc, Iran<br />
In Mulago Hospital’s accidents and emergency ward, the<br />
evolutionary survival of the fittest reigns. Due to the scarcity of<br />
resources, one can only hope that they will be able to extend<br />
a patient’s life until the next bottle of normal saline, the next<br />
dose of antibiotics, the next shot of insulin appears. On arrival,<br />
patients are examined by an intern or medical officer who then<br />
triages them into outpatient and red zone cases.<br />
The ongoing strike by medical professionals in Uganda against<br />
the poor pay and unfair working conditions they endure has left<br />
hospitals even more understaffed than usual. The high costs of<br />
medical care in private hospitals drive the majority who cannot<br />
afford a government-funded hospital. The promise of free<br />
services, however, is unfulfilled as the cost of tests and treatments<br />
are out-of-reach for many patients and families.<br />
Highlights<br />
Perspectives<br />
Behind the Scenes<br />
Announcements<br />
Spotlight<br />
Reflections<br />
Nursing Division<br />
SARS COV-2 Pandemic<br />
and Us<br />
Clinical Case Report<br />
The prevailing circumstances dictate that we practice medicine with extremely depleted resources<br />
and a ceaseless stream of patients, some of whom are abandoned at the entrance by their relatives<br />
out of hopeless desperation. When pushed between a rock and a hard place, you have to make<br />
decisions that only you can understand. Disease spares no one, and considers neither resource<br />
nor accessibility. The 30% mortality rate in Mulago for those in admission remains just as high after<br />
discharge, meaning the mortality risk is cumulatively 60% on arrival, regardless of cause.<br />
On this tropical November morning, in the middle of the crowded, dimly-lit emergency hall of<br />
Mulago National Referral Hospital, it was busy as usual with multiple lengthy and tasking rounds.<br />
As we completed the teaching round, a few nurses carried a pale, cold girl into the room. This was<br />
a diurnal occurrence; patients are brought into an already suffocating ward with meager resources<br />
where they continue the fight for life while medical personnel wrestle to give them the chance.<br />
At the time the little girl was brought in, we had only one patient left to end the round and were<br />
tired to the core. She was dropped off at the adjoining verandah and carried by the nurses into<br />
the emergency room. Her radial pulse was absent, with no detectable blood pressure. The only<br />
signs of life were carotid vibrations in addition to an abnormal breathing pattern. The sweet smell<br />
emanating from her mouth, coupled with the distressed breathing, are pathognomonic of diabetes<br />
mellitus.<br />
The examination revealed a Glasgow Coma Scale (GCS) level of 3/15. We immediately planned<br />
to start intravenous fluids with two liters of normal saline, which was a setback because we could<br />
A New Column<br />
Global Health and the Arts<br />
Articles of the Month<br />
Videos of the Month<br />
Calendar<br />
Resources<br />
17<br />
Spotlight continued on next page >>
OUR PEOPLE,<br />
OUR MISSION<br />
Global Health<br />
<strong>eMagazine</strong><br />
<strong>April</strong> 2022<br />
Watch this video!!<br />
Bani Adam by Saadi Shirazi<br />
hardly find veins to insert the cannula. Other options such as placing a central line were out of<br />
the question because of their unavailability. We finally managed to place two peripheral lines.<br />
Her blood glucose level was about 200, while her blood pressure remained undetectable even<br />
after running normal saline. During the process of inserting a foley catheter, we noticed bruises<br />
and potential signs of rape. We put her on vasopressors. Because there was no norepinephrine<br />
available, we started epinephrine until the mean arterial pressure rose to about 60 mmHg. A few<br />
hours later, the first lab tests revealed a sodium level of 175. I checked all possible evidence-based<br />
resources I could, including Up-To-Date, to decide which direction we should take to save her life.<br />
The next day during the night shift, the sodium level rose to 183. I borrowed a thermometer which<br />
showed a mild fever (37.9 °C). She was fighting this battle alone with no family or supporters to get<br />
her medication, beddings, or food. With the hospital’s public laboratory and pharmacy locked<br />
overnight, I paid a local broker to purchase ampicillin-sulbactam and potassium chloride. I also<br />
contacted my professor at Saint Louis, Missouri who gave us guidelines on how to conduct the<br />
fluid replacement considering the condition of the patient, who was undergoing renal failure (BUN:<br />
80, Creatinine: 4.1) and acute hepatic injury, as indicated by raised liver enzymes. Two days later,<br />
she gained consciousness and spoke a name once before losing it again. One may wonder whose<br />
name it was or why she uttered it as she walked the thin line between being awake and asleep.<br />
We tried to get her an intensive care unit bed in the following days, but that proved too big a<br />
dream. A few days later, I was involved in a major wound debridement of a young man with severe<br />
electricity burns, who had a myriad of complications from intestinal necrosis to tendon disruptions.<br />
In the midst of that six-hour surgical debridement in the operation room, with everybody’s hands<br />
full with all workloads in the emergency room hall and dire conditions prevailing, the march of<br />
death was played, and she left us and flew to the moon.<br />
Highlights<br />
Perspectives<br />
Behind the Scenes<br />
I wonder if in an alternate, well-equipped Mulago, she would have survived this cruel life that<br />
makes us all fight to have it. I draw comfort knowing we did our best with what we had while she<br />
was with us. I regret not being able to hold her hand as she passed away. She left this world in<br />
silence with no one crying for her, with no one present who knew who she was. Maybe someone out<br />
there is still looking for her.<br />
Announcements<br />
Spotlight<br />
Reflections<br />
Nursing Division<br />
SARS COV-2 Pandemic<br />
and Us<br />
Clinical Case Report<br />
A New Column<br />
Global Health and the Arts<br />
Articles of the Month<br />
Videos of the Month<br />
Calendar<br />
Resources<br />
Saida agliullina (Kazan)<br />
18
OUR PEOPLE,<br />
OUR MISSION<br />
Global Health<br />
<strong>eMagazine</strong><br />
<strong>April</strong> 2022<br />
Watch this video!!<br />
Bani Adam by Saadi Shirazi<br />
REFLECTIONS<br />
COVID-19: Reflections from a Russian Resident<br />
Physician<br />
Part 2/2<br />
Written by Aliya S. Zakirova, MD<br />
PGY-1, Primary Care, Kazan State Medical University, Kazan,<br />
Republic of Tatarstan, Russian Federation<br />
I acquired a mild COVID-19 infection that did not require<br />
hospitalization. The only thing that scared me was the risk of<br />
infecting others and the long COVID effects. Meanwhile, a new<br />
infectious diseases hospital opened, calling for new staff. Due<br />
to an uptick in the number of infections, there was an acute<br />
shortage of nurses in the red zones. I decided to work in the<br />
infectious diseases department and worked with teams that<br />
exclusively catered to COVID-19 patients.<br />
Highlights<br />
Perspectives<br />
Behind the Scenes<br />
Announcements<br />
Spotlight<br />
Reflections<br />
Nursing Division<br />
SARS COV-2 Pandemic<br />
and Us<br />
Clinical Case Report<br />
A New Column<br />
Global Health and the Arts<br />
Articles of the Month<br />
For me, working in an infectious diseases hospital was a great experience with new staff, new<br />
conditions, new triage and treatment zones. We had to work with the personal protective equipment<br />
on all the time. It was funny at first just donning a PPE, but when attending patients, you start<br />
realizing that there is a great responsibility on your shoulders.Though some patients were afraid of<br />
our PPE, some started to recognize us by simply watching our eyes. We worked in the red zone in<br />
six-hour shifts, following which we were shifted to clean zones to process the documents, dispense<br />
medicines, and organize other processes. Soon we became one family with our colleagues in these<br />
difficult conditions, supporting each other physically as well as emotionally. This helped me realize<br />
the importance of teamwork.<br />
Another positive of COVID-19 was adapting to working from home. The epidemic and self-isolation<br />
also influenced our habits. We began to wash our hands and face more often. We learned to come<br />
home from the street without touching our faces. These can be termed as a good side effect,<br />
as doctors around the world reported reduction in the numbers of intestinal infections. People<br />
began to listen carefully for any physical symptoms, fearing that some of them would reveal a<br />
“manifestation” of the virus. Health awareness suddenly became a priority for the average citizen<br />
of our country, which was previously approached casually.<br />
I graduated in 2021 and am now working as a resident physician in primary care. These days we are<br />
witnessing a new wave of coronavirus infections with symptoms mimicking the flu. As I see it, one<br />
way or another, everybody has come across the COVID-19 infection. Someone is ill now, someone<br />
has been ill; someone’s relatives or friends are or have been sick. Our world with patients is divided<br />
into before and after COVID-19. We have become more health conscious. The level of earnings,<br />
standards of living, frequency of offshore vacations, form and type of employment have changed<br />
due to COVID-19. Many people have revised their attitude to managing and planning their lives.<br />
It is more difficult to estimate non-measurable parameters that also affect identity. What has<br />
changed in our psychology? What new parameters and relationships have appeared? My world<br />
has been different «before and after» due to the new SARS-CoV-2 coronavirus infection. There’s so<br />
much unclarity! But I am hopeful and certain that this too shall pass.<br />
Videos of the Month<br />
Calendar<br />
Resources<br />
Click here to visit the Nuvance Health<br />
Global Health Program COVID-19<br />
Resource Center<br />
19<br />
Reflections continued on next page >>
OUR PEOPLE,<br />
OUR MISSION<br />
Global Health<br />
<strong>eMagazine</strong><br />
<strong>April</strong> 2022<br />
Watch this video!!<br />
Bani Adam by Saadi Shirazi<br />
A Ugandan Student’s Education in the Foil of the<br />
COVID-19 Pandemic<br />
Part 2/2<br />
Written by Abraham Ddungu Matovu<br />
Medical Student, MakCHS<br />
All seemed to be returning to normal until June 2021 in my third<br />
year of medical school when Uganda experienced the second<br />
wave of COVID-19, forcing the president to issue yet another<br />
nationwide lockdown similar to the one we had stomached the<br />
previous year. I was still filled with the excitement of getting an<br />
elective placement abroad at Cambridge University, UK but this<br />
meant I had to pause and wait on the return of normalcy.<br />
This lockdown further slowed academic progress, pushing completion of my medical school<br />
education to a later date than initially planned. In the second lockdown I volunteered to help<br />
health workers in Kampala District by encouraging people to come for COVID-19 vaccination. The<br />
Ugandan government had acquired AstraZeneca, Pfizer, Johnson & Johnson, Sinovac and Moderna<br />
vaccines. We also experienced a massive usage of herbal drugs by Ugandans in the plight of the<br />
looming pandemic. This particular lockdown was shorter than the first one and by August 2021 we<br />
were allowed to return to university to continue with our studies.<br />
Highlights<br />
Perspectives<br />
Behind the Scenes<br />
Announcements<br />
Spotlight<br />
Reflections<br />
Nursing Division<br />
SARS COV-2 Pandemic<br />
and Us<br />
As the saying goes that tough times don’t last but tough people do, I was able to successfully wade<br />
my way through the third year of medical school amidst a blended learning experience of physical<br />
and online studies. In December 2021, I was placed in Kiryandongo District, Uganda with eight other<br />
medical students for Community Based Education and Research Studies (COBERS) placement, an<br />
initiative designed by Makerere University College of Health Sciences (MakCHS) to bridge to the<br />
gap between urban and rural communities in accessing healthcare services. This is because more<br />
than 80% of the population in Uganda lives in rural areas yet 80% of the nation’s doctors live in the<br />
capital city of Kampala. As part of the curriculum, medical students in small grounds are expected to<br />
train and live in a rural community where they diagnose health challenges and work with the people<br />
to design a solution. The COBERS site, located all over Uganda, is pre-determined at MakCHS.<br />
During the COBERS placement in Kisorosoro village, Kiryadongo District located Northwest of<br />
Kampala, western Uganda, we conducted a community diagnosis where we were able to assess<br />
the impact of the pandemic on the local community while helping recommend potential solutions<br />
to overcome these challenges. In conclusion, the COVID-19 pandemic has led to many deaths, loss<br />
of jobs resulting in inability to afford school tuition, and an increase in school dropouts especially<br />
among teenage girls in Uganda. However, I am still positive about the recovery of our economy and<br />
improvement in disease surveillance all over the world to prevent such pandemics from happening<br />
again.<br />
Clinical Case Report<br />
A New Column<br />
Global Health and the Arts<br />
Articles of the Month<br />
Videos of the Month<br />
Calendar<br />
Resources<br />
20<br />
Reflections continued on next page >>
OUR PEOPLE,<br />
OUR MISSION<br />
Global Health<br />
<strong>eMagazine</strong><br />
<strong>April</strong> 2022<br />
Watch this video!!<br />
Bani Adam by Saadi Shirazi<br />
Highlights<br />
Perspectives<br />
Behind the Scenes<br />
Announcements<br />
Spotlight<br />
Reflections<br />
Nursing Division<br />
SARS COV-2 Pandemic<br />
and Us<br />
Clinical Case Report<br />
A New Column<br />
Global Health and the Arts<br />
Articles of the Month<br />
Videos of the Month<br />
I Am Still Trying to Catch up With My Academic<br />
Journey<br />
Part 2/3<br />
Written by Natukunda Ferguson<br />
Medical Student, MakCHS<br />
At some point the English premier league, which had been<br />
closed in March 2020, resumed and occupied part of my<br />
time. I am a staunch supporter of Manchester United and the<br />
games lit up my world once again. This was however shortlived<br />
and did not satisfy my mental health.<br />
With time, COVID-19 cases began declining with more<br />
patients recovering. Having reached seven months without<br />
studying, I had lost hope and moved on. My poultry and<br />
plants were doing well and I did not care about when I could<br />
return to school. Then, the Ministry of Education announced<br />
that students enrolled in health sciences-related programs in their final year of study were allowed<br />
to resume in-person classes. This was done because the health sector was overwhelmed and<br />
needed more labor force. I was not a finalist, so I had to sit, relax, and wait for my time which was<br />
unknown. However, my hope was rekindled. “If the finalists were allowed to get back and do the<br />
exams, we too shall go back soon,” I thought to myself.<br />
One month later, I resumed school with virtual lectures via the Zoom video conferencing platform. I<br />
faced multiple challenges with this new online mode of learning. I was residing in a remote village<br />
in Western Uganda for the entire lockdown with a very poor communication network that could not<br />
sustain the online lectures. The environment at home was not good for concentrating and studying<br />
as I could be interrupted. These coupled together made studying at home a hustle.<br />
I told a good friend and classmate about the challenges I was facing only to find I was not alone.<br />
We worked out a plan that involved traveling back to Kampala. Not yet being allowed to report<br />
physically to school, we rented a hostel near the university in search of a good network to create a<br />
conducive learning environment. By the time I settled in, my fellow classmates had covered lots of<br />
material and I had to work harder to catch up. No longer facing challenges with the Zoom platform,<br />
I could attend lectures in the comfort of my room. End-of-semester exams were given on an online<br />
platform called Makerere University Electronic Learning Environment (MUELE), which had loopholes<br />
like slowing down when doing real-time exams.<br />
Though these exams were not favorable, I persevered and completed the semester that I had left<br />
uncompleted at the onset of the lockdown. A five-week recess term to end second year proceeded,<br />
as opposed to the usual ten weeks. Having finished the recess, I was set for the next academic<br />
year which I was looking forward to as it is the start of clinical rotations. I was curious to see how<br />
my experience as a junior clerk would affect my attitude and choices between the medical and<br />
surgical specialties.<br />
Third year began with a blended form of learning whereby we had some lectures and presentations<br />
online and also went to the wards for physical learning. My first clinical rotation was in the<br />
department of surgery. I was excited to start practicing on the wards, clerking patients, presenting<br />
to senior doctors, and scrubbing into surgeries. However, there were new rules like wearing masks<br />
and reducing interaction with patients, fellow students, and doctors. With patients being said to<br />
be the best textbooks, the restrictions and fear of contracting the virus limited my clinical exposure.<br />
I later had my rotation in internal medicine which I was passionate about. I interacted with senior<br />
doctors who taught me a lot and inspired me to work harder.<br />
Calendar<br />
Resources<br />
21<br />
Reflections continued on next page >>
OUR PEOPLE,<br />
OUR MISSION<br />
Global Health<br />
<strong>eMagazine</strong><br />
<strong>April</strong> 2022<br />
Watch this video!!<br />
Bani Adam by Saadi Shirazi<br />
Highlights<br />
Perspectives<br />
Behind the Scenes<br />
Announcements<br />
Spotlight<br />
Reflections<br />
Nursing Division<br />
SARS COV-2 Pandemic<br />
and Us<br />
Clinical Case Report<br />
A New Column<br />
Global Health and the Arts<br />
Articles of the Month<br />
Videos of the Month<br />
Calendar<br />
Resources<br />
NURSING DIVISION<br />
Editor:<br />
Catherine Winkler, PhD, Nurse Practitioner - BC<br />
Written by<br />
Mary Kincart, MS, RN<br />
Corporate Director Quality and Patient Safety New York<br />
Presbyterian<br />
Palliative Care<br />
As nurses, we may have been drawn to the profession<br />
because we wanted to help others and alleviate suffering.<br />
The heart of nursing is a call to palliate: to relieve human<br />
suffering, both physical and mental. It is what we are called<br />
to do. Mark Lazenby, PhD, APRN, FAAN, reminds us in his book<br />
Caring Matters Most that “caring about and for others is a<br />
specific kind of calling.” He quotes the philosopher-nurse Patricia Benner’s saying that the calling<br />
of nursing demands that we care “for the disenfranchised, the vulnerable and the suffering.” (M.<br />
Lazenby Caring Matters Most p.6)<br />
The World Health Organization (WHO) describes palliative care as an approach that improves<br />
the quality of life of patients by managing pain, relieving symptoms, and providing physical and<br />
emotional comfort. We provide palliative care in many different ways. Palliative care is influenced<br />
by many factors including the culture, beliefs, and socioeconomic factors of the patients we care<br />
for. The WHO calls us to understand that ‘‘relieving serious health-related suffering, be it physical,<br />
psychological, social, or spiritual, is a global ethical responsibility.” (WHO Health topics / Palliative<br />
care)<br />
“In 2014, the first ever global resolution on palliative care, World Health Assembly resolution WHA67.19,<br />
called upon WHO and Member States to improve access to palliative care as a core component<br />
of health systems, with an emphasis on primary health care and community/home-based care.<br />
WHO’s work to strengthen palliative care focuses on the following areas:<br />
• integrating palliative care into all relevant global disease control and health system plans;<br />
• developing guidelines and tools on integrated palliative care across disease groups and<br />
levels of care, addressing ethical issues related to the provision of comprehensive palliative<br />
care;<br />
• supporting Member States in improving access to palliative care medicines through improved<br />
national regulations and delivery systems;<br />
• a special focus on palliative care for people living with HIV, including development of<br />
guidelines;<br />
• promoting increased access to palliative care for children (in collaboration with UNICEF);<br />
• monitoring global palliative care access and evaluating progress made in palliative care<br />
programmes;<br />
• developing indicators for evaluating palliative care services;<br />
• encouraging adequate resources for palliative care programmes and research, especially<br />
in resource-limited countries; and building evidence of models of palliative care that are<br />
effective in low- and middle-income settings.” (WHO Health topics / Palliative care)<br />
Palliative care is influenced by many factors including our culture, ethnic background, and religious<br />
beliefs. As nurses, we value and integrate all these things in the care we render to our patients. I<br />
invite all to share your knowledge and experience from your own culture to enhance a greater and<br />
more global understanding of our efforts to provide palliative care and the challenges we face in<br />
supporting this human right.<br />
22<br />
Nursing continued on next page >>
OUR PEOPLE,<br />
OUR MISSION<br />
Women’s Health Education<br />
Postpartum Depression<br />
Written by Sarah Cordisco<br />
Global Health<br />
<strong>eMagazine</strong><br />
<strong>April</strong> 2022<br />
Watch this video!!<br />
Bani Adam by Saadi Shirazi<br />
Senior Nursing Student at the University of Vermont<br />
Postpartum depression is a major health concern in all countries<br />
and is the most common mental health problem in the postnatal<br />
period. Generally, postpartum depression (PPD) occurs four<br />
to six weeks after childbirth, with symptoms similar to major<br />
depressive disorder. These symptoms include “depressed mood,<br />
loss of interest or pleasure in activities, sleep disturbance,<br />
appetite disturbance, loss of energy, feelings of worthlessness or<br />
guilt, diminished concentration, irritability, anxiety, and thoughts of suicide” (Slomian et al., 2019).<br />
Many women may experience a phenomenon called “baby blues,” a transient, self-limiting mood<br />
disorder that begins two to three days after birth and resolves within two weeks. Both postpartum<br />
depression and baby blues occur from the sudden drop and change in estrogen and progesterone<br />
after having a baby. In addition to hormonal changes, the role and life changes that occur after<br />
add additional stress that can affect mental health.<br />
Highlights<br />
Perspectives<br />
Behind the Scenes<br />
Announcements<br />
Spotlight<br />
On average, PPD affects about one in five women, although this statistic varies from country to<br />
country. In higher-income countries, the prevalence of PPD varies from 10-15% in the first year after<br />
birth while in lower and lower middle-income countries the prevalence is around 18.6% (Wang et al.,<br />
2021), although some studies have shown these numbers to be up to 60% of the population. Southern<br />
Africa has been seen to have the highest prevalence rate at 39.96%, followed by Southern Asia with<br />
22.32%, South American at 21.71%, Western Asia at 19.83% and Northern Africa at 18.75% (Wang et al.,<br />
2021). These numbers are likely significantly higher, as not everyone reports their symptoms. Some<br />
mothers may not report due to the fear of being judged for their symptoms or for not bonding<br />
with their baby as easily. Others may be unaware that this condition exists and fail to mention<br />
their feelings to their healthcare providers. The rate of this mental health disorder is also affected<br />
by other factors such as “marital status, education level, social support, spouse care, violence,<br />
gestational age, breastfeeding, child mortality, pregnancy plan, financial difficulties, partnership,<br />
life stress, smoking, alcohol intake, and living conditions” (Wang et al., 2021).<br />
Reflections<br />
Nursing Division<br />
SARS COV-2 Pandemic<br />
and Us<br />
Clinical Case Report<br />
A New Column<br />
Global Health and the Arts<br />
Articles of the Month<br />
Videos of the Month<br />
When dealing with PPD, women need a lot of support and must develop coping strategies. Coping<br />
is the cognitive and behavior process that a person uses to deal with stressful circumstances that<br />
are demanding, challenging, threatening, or have a potential for harm or loss. Coping styles are<br />
broken into three categories: problem-focused, emotion-focused, and dysfunction or avoidance<br />
coping. Problem-focused coping involves the person dealing with the source of the stress, whereas<br />
emotion-focused coping is when the person attempts to handle the thoughts and feelings<br />
associated with the stressor. Dysfunctional or avoidant coping is a strategy in which a person<br />
avoids dealing with both the stressor and the emotions associated (Azale et al., 2018). While coping<br />
strategies vary from culture to culture, it is important that postpartum women develop coping<br />
mechanisms that will be healthy and beneficial to their mental health. They must have a support<br />
system which may consist of family, friends, or community. Many women may also find spirituality or<br />
religion to be very beneficial when dealing with postpartum depression. It is important that women<br />
identify their own support systems and where they can turn to when experiencing these feelings.<br />
They must be encouraged to talk about their feelings and emotions after having a baby without<br />
shame or judgment from others.<br />
In the next article I would like to talk about women’s rights and the differences we see across the<br />
globe, as well as different women’s activist groups. If anyone has anything to share or questions to<br />
ask about any topic I write about, please feel free to email me at: sarah.cordisco@gmail.com<br />
Calendar<br />
Resources<br />
References<br />
Azale, T., Fekadu, A., Medhin, G., & Hanlon, C. (2018). Coping strategies of women with postpartum depression symptoms in<br />
rural Ethiopia: A cross-sectional community study. BMC Psychiatry, 18(1), 41. https://doi.org/10.1186/s12888-018-1624-z<br />
Slomian, J., Honvo, G., Emonts, P., Reginster, J.-Y., & Bruyère, O. (2019). Consequences of maternal postpartum<br />
depression: A systematic review of maternal and infant outcomes. Women’s Health, 15, 174550651984<strong>40</strong>44. https://doi.<br />
org/10.1177/174550651984<strong>40</strong>44<br />
Wang, Z., Liu, J., Shuai, H., Cai, Z., Fu, X., Liu, Y., Xiao, X., Zhang, W., Krabbendam, E., Liu, S., Liu, Z., Li, Z., & Yang, B. X. (2021).<br />
Mapping global prevalence of depression among postpartum women. Translational Psychiatry, 11(1), 1–13. https://doi.<br />
org/10.1038/s41398-021-01663-6<br />
Nursing continued on next page >><br />
23
OUR PEOPLE,<br />
OUR MISSION<br />
A New Series:<br />
SARS-COV2 PANDEMIC AND US<br />
Global Health<br />
<strong>eMagazine</strong><br />
<strong>April</strong> 2022<br />
Watch this video!!<br />
Bani Adam by Saadi Shirazi<br />
Highlights<br />
Perspectives<br />
Behind the Scenes<br />
Announcements<br />
Spotlight<br />
Reflections<br />
Nursing Division<br />
SARS COV-2 Pandemic<br />
and Us<br />
Clinical Case Report<br />
A New Column<br />
Global Health and the Arts<br />
Articles of the Month<br />
Videos of the Month<br />
Calendar<br />
Resources<br />
A Nursing Professor’s Perspective in Teaching<br />
During a Pandemic<br />
Part 2/3<br />
Written by Monica Sousa Ed.D, ACNS-BC, APRN<br />
Professor of Nursing at Western Connecticut State University<br />
One of the big challenges was to decide how to proctor an exam<br />
online in a secure way that minimizes the possibility of academic<br />
dishonesty. In the past, we had wanted to administer exams<br />
electronically but did not have the software to ensure they<br />
would be secure. Examples of challenges we had seen occur<br />
included students opening another browser or tab and looking<br />
up answers; printing the exam to students in another part of the<br />
building; and instant messaging each other regarding answers.<br />
We had no way to prevent cheating, so this was a huge concern<br />
for faculty when we went virtual.<br />
Luckily, the university purchased an online proctoring software that would prevent students from<br />
doing anything else but take the exam. It also video-recorded students while they took the test.<br />
Students had to do a room scan to show their table surface and around the room to ensure they<br />
were taking the exam independently without assistance or other materials. Faculty had access<br />
to these recordings and the software would flag areas where the student was spending too<br />
much time looking away from the screen or there was extra noise in the room, etc. Importantly,<br />
another idea we had to help minimize cheating was student review and signature of the academic<br />
honesty statement prior to beginning each exam. Failure to comply with the policy would result in<br />
a zero grade on the exam and possible failure of the course and the nursing program. There was a<br />
learning curve for all faculty to learn how to set up their exams on Blackboard using the proctoring<br />
software. A few faculty unofficially became super-users who assisted other faculty in setting up and<br />
administering the exams. Our department was also fortunate to have an instructional designer to<br />
help troubleshoot Blackboard issues and establish online courses. Setting up students for success by<br />
minimizing the chances of academic dishonesty was important to maintaining academic integrity<br />
and fairness.<br />
Another positive occurrence and one I will always remember is the way in which the faculty helped<br />
each other during this turbulent time. Some became unofficial superusers of technological aspects<br />
and resource points for others if needed. We would all meet weekly to discuss challenges with<br />
technology, student concerns, and next steps would to meet the ongoing changes related to<br />
COVID-19. We created a team to help us get through any challenge before us. When the summer<br />
of 2020 arrived, we were told that classes would be all online asynchronous. During the fall 2020<br />
semester I was to teach a medical-surgical nursing class to juniors along with three other faculty. We<br />
spent hundreds of hours planning and creating a student-centered interactive learning environment.<br />
One faculty member suggested a flipped classroom approach to deliver the information in a virtual<br />
environment. This was new to the rest of us, but under the circumstances we thought it was a clever<br />
idea to try it out.<br />
We recorded voiceover PowerPoint lectures and assigned case studies and other interactive learning<br />
assignments to provide opportunities for students to apply the information they read in chapters<br />
and reviewed in lecture. We each had designated times that we would be on video conferencing<br />
to review assignment answers and review the concepts of the week. Unfortunately, many students<br />
did attend these video conferences as they were not mandatory. The active learning assignments<br />
we developed and assigned were to engage students to apply the information to a scenario or<br />
situation. When they take our course exams or the state board exam, the questions are designed<br />
to apply the information with applying critical thinking and clinical judgment. We wanted to foster<br />
this way of thinking and processing. Students initially struggled with the coursework and felt that<br />
the assignments were just busywork. However, after reviewing the first exam with students and<br />
demonstrating how the concepts and critical thinking were used to answer the questions, they<br />
began to see the value in the assignments.<br />
24
OUR PEOPLE,<br />
OUR MISSION<br />
CLINICAL CASE<br />
OF THE MONTH<br />
Global Health<br />
<strong>eMagazine</strong><br />
<strong>April</strong> 2022<br />
Watch this video!!<br />
Bani Adam by Saadi Shirazi<br />
Editor:<br />
Majid Sadigh, MD<br />
Boda-bodas: A Bittersweet Transport Mode and a Silent Killer<br />
Written by Joshua Matsiko, medical student at MakCHS<br />
Highlights<br />
Perspectives<br />
Behind the Scenes<br />
Announcements<br />
Spotlight<br />
Reflections<br />
Nursing Division<br />
SARS COV-2 Pandemic<br />
and Us<br />
Clinical Case Report<br />
A New Column<br />
Global Health and the Arts<br />
Articles of the Month<br />
Videos of the Month<br />
Calendar<br />
Resources<br />
It is 8:36 PM when a 17-year-old male is rushed in a semi-conscious state with signs of multiple<br />
trauma after being involved in a boda-boda accident 18 hours ago. Primary and secondary surveys<br />
are immediately performed and the patient receives initial care to save his life. After a few minutes,<br />
the doctors realize he is sliding into hemorrhagic shock, and immediately a Focused Assessment<br />
with Sonography (FAST) reveal the patient has a ruptured spleen with massive intra-abdominal<br />
hemorrhage. The patient quickly goes in for an exploratory laparotomy with splenectomy and two<br />
liters of blood are drained from the abdomen as he is fighting for his dear life. One thing he has in<br />
common with dozens of trauma patients who flock the casualty ward daily is that a boda-boda<br />
accident was involved in their cause for trauma. For those who wonder what boda-boda is, it is the<br />
motorcycle form of taxi used throughout Uganda and particularly at a higher rate in Kampala since<br />
it provides a faster way to move through the ever-slow or static traffic around the city.<br />
Every minute of the day, at the causality ward (emergency room) of Mulago National Referral<br />
Hospital, numerous ambulances and police patrols flock in with trauma patients of every kind from<br />
accidents, beatings, and stab wounds from thugs and fights. The casualty ward is full to the brim<br />
as usual with the number of patients exceeding the number of beds available. Some will have to<br />
painfully wait on the floor or outside the ward. As a medical student, something continued to strike<br />
my mind every time I reviewed a fresh patient about the cause of trauma: it was amazing to notice<br />
that this one word was common among a great deal of patients. I decided to carry out a study<br />
research and the results will amaze you.<br />
During the one-month period between January and February 2022, 622 trauma patients were<br />
studied. Of these, 336 (54%) were from road traffic crashes (RTCs) of which 252 directly involved a<br />
boda-boda, accounting for 75% of all the 336 RTCs and approximately 41% of all trauma cases.<br />
One should take note that this only caters for direct accidents but there are also patients coming<br />
in with indirect boda-boda involvements, for example boda-boda riders who are badly beaten<br />
25<br />
Clinical Case continued on next page >>
OUR PEOPLE,<br />
OUR MISSION<br />
Global Health<br />
<strong>eMagazine</strong><br />
<strong>April</strong> 2022<br />
Watch this video!!<br />
Bani Adam by Saadi Shirazi<br />
Highlights<br />
Perspectives<br />
Behind the Scenes<br />
Announcements<br />
by passengers they carried and their motorcycles robbed or passengers who were assaulted by<br />
riders and their belongings stolen. In some it was an RTC where a car driver intended to drift past<br />
a boda-boda cyclist and ended up crashing into another car or pedestrians, etc.<br />
Therefore, when we included indirect boda-boda involvements, we discovered that boda-bodas<br />
were involved in more than 50% of all casualty admissions meaning these causes alone bring in<br />
more cases than all other emergency causes combined. This data also doesn’t include those that<br />
pass away on impact or at the site of the accident. On further study, I discovered that on average,<br />
boda-boda accidents kill at least 10 people daily in Kampala alone and this costs the government<br />
4.4 trillion Uganda shillings, approximately 1.3 US billion dollars annually. These accidents cause<br />
more deaths than HIV, diarrheal diseases, and tuberculosis and I believe this calls for some action<br />
to remedy the situation.<br />
With further study, I found five cardinal reasons for this high rate of boda-boda accidents:<br />
negligence of road safety rules, competition for passengers with fellow riders and other public<br />
transport operators, inadequate helmet usage, drug use, and reckless, speedy driving. To a larger<br />
percentage, these are behavioral causes. Since boda-bodas serve such a great purpose, we can’t<br />
do away with them but we can increase safety for both passengers and riders through means such<br />
as digitalization of drivers, driver sensitization of road safety, and provision of protective gear to<br />
riders and passengers alike.<br />
We conducted a study that discovered only 4% of boda-boda accidents involve digitized riders.<br />
Boda-boda accidents can be lowered to negligible levels towards saving lives while lowering the<br />
healthcare burden. I have a detailed scheme on how boda-boda accidents can be lowered by<br />
approximately 80% in three years with partnership from interested individuals. It hurts to see the<br />
constant rise of disabilities and death along with the associated rise in orphans and widows, many<br />
of whom remain helpless due to deaths or permanent disability of their bread-winners. Anyone who<br />
may wish to come to Uganda, look out for this silent killer.<br />
For more information, please contact me at matsikojoshua091@gmail.com or WhatsApp<br />
+256703630454.<br />
Watch the case presentation here >><br />
Spotlight<br />
Reflections<br />
Nursing Division<br />
SARS COV-2 Pandemic<br />
and Us<br />
Clinical Case Report<br />
A New Column<br />
Global Health and the Arts<br />
Articles of the Month<br />
Videos of the Month<br />
Calendar<br />
Resources<br />
Parvin Sadigh (Iran)<br />
26
OUR PEOPLE,<br />
OUR MISSION<br />
Global Health<br />
<strong>eMagazine</strong><br />
<strong>April</strong> 2022<br />
Watch this video!!<br />
Bani Adam by Saadi Shirazi<br />
Highlights<br />
Perspectives<br />
Behind the Scenes<br />
Announcements<br />
Spotlight<br />
Reflections<br />
Nursing Division<br />
SARS COV-2 Pandemic<br />
and Us<br />
A NEW COLUMN<br />
Editor: Joshua Matsiko<br />
Medical student at MakCHS<br />
I am an undergraduate student at Makerere<br />
university offering a bachelors of medicine and<br />
a bachelors of surgery in my third year with an<br />
emphasis in global health and research. I am an<br />
open-minded learner who is very passionate and<br />
committed to achieving the best in every activity<br />
I set my mind on and am always eager to learn<br />
more. I have a particular interest in global health<br />
and speaking out for the largely marginalized<br />
population to see that their health is improved<br />
where possible. I am an active member of society<br />
empowering organizations and a proprietor of<br />
better health Uganda. I am happy to be part of<br />
this group and hope to learn a lot from everyone<br />
here.<br />
The purpose of this new section is to discuss the health sector in Uganda and Africa at large. In<br />
doing so, we hope to collectively better the health of Ugandans and the world at large and add a<br />
stone to the global health community.<br />
Objectives<br />
• To provide information about different health issues and fields of particularly high interest<br />
and those that are of importance in global health medicine and affecting the greater part<br />
of the population. This may be in the form of articles, particular case stories, etc.<br />
• To evaluate the role of cultural, social, religious, economic, and psychological systems in<br />
Uganda and their net effect on the health of the population.<br />
• To voice the greatest and/or neglected health issues and see how we can better the health<br />
of marginalized, less privileged populations in Uganda.<br />
• To maintain a high degree of professionalism throughout our endeavors.<br />
• To discuss the effect of alternative medicine on the general patient’s health.<br />
Clinical Case Report<br />
A New Column<br />
Global Health and the Arts<br />
Articles of the Month<br />
Click here to visit the Nuvance Health Global Health Program<br />
COVID-19 Resource Center<br />
Videos of the Month<br />
Calendar<br />
Resources<br />
27
OUR PEOPLE,<br />
OUR MISSION<br />
ART TO REMIND US<br />
OF WHO WE CAN BE<br />
Global Health<br />
<strong>eMagazine</strong><br />
<strong>April</strong> 2022<br />
Watch this video!!<br />
Bani Adam by Saadi Shirazi<br />
Peace<br />
BEST POEMS ABOUT PEACE<br />
Peace in thy hands,<br />
Peace in thine eyes,<br />
Peace on thy brow;<br />
Flower of a moment in the eternal hour,<br />
Peace with me now.<br />
Highlights<br />
Perspectives<br />
Behind the Scenes<br />
Announcements<br />
Spotlight<br />
Reflections<br />
Nursing Division<br />
SARS COV-2 Pandemic<br />
and Us<br />
Clinical Case Report<br />
A New Column<br />
Editor: Majid Sadigh<br />
Contributing Editor: Mitra<br />
Sadigh<br />
During times of confusion, tribulation,<br />
grief, uncertainty, and despair, the<br />
arts enliven us by reintegrating the<br />
disjointed pieces of ourselves and<br />
replenishing them with clarity and hope.<br />
The arts remind us of our individual and<br />
collective potential to grow, evolve, and<br />
transform. They remind us of what and<br />
who we can be and what we can create.<br />
In this new section, we bring you works<br />
of art that have moved and inspired us.<br />
We encourage you to also share works<br />
that have inspired you.<br />
Not a wave breaks,<br />
Not a bird calls,<br />
My heart, like a sea,<br />
Silent after a storm that hath died,<br />
Sleeps within me.<br />
All the night’s dews,<br />
All the world’s leaves,<br />
All winter’s snow<br />
Seem with their quiet to have stilled in life’s dream<br />
All sorrowing now.<br />
-Walter de la Mare<br />
Best Poems About Peace<br />
Global Health and the Arts<br />
Articles of the Month<br />
Videos of the Month<br />
Calendar<br />
Resources<br />
https://youtu.be/HpxX4ZE4KWE<br />
28
OUR PEOPLE,<br />
OUR MISSION<br />
ARTICLE OF THE MONTH<br />
Global Health<br />
<strong>eMagazine</strong><br />
<strong>April</strong> 2022<br />
Meeting the health challenges of displaced populations from Ukraine<br />
Yulia Ioffe, Ibrahim Abubakar, Rita Issa, Paul Spiegel, Bernadette N Kumar<br />
Lancet March 26, 2022<br />
Watch this video!!<br />
Bani Adam by Saadi Shirazi<br />
Highlights<br />
Perspectives<br />
Behind the Scenes<br />
Announcements<br />
Spotlight<br />
Reflections<br />
Nursing Division<br />
SARS COV-2 Pandemic<br />
and Us<br />
Clinical Case Report<br />
A New Column<br />
Global Health and the Arts<br />
Articles of the Month<br />
Videos of the Month<br />
The worsening humanitarian catastrophe and conflict in Ukraine has led to the largest refugee crisis in Europe<br />
since World War 2. Millions of people are expected to flee Ukraine, with more than a million individuals having<br />
fled the country in the first week of the conflict alone.1 The consequences of war, trauma, and devastation<br />
must be tackled swiftly. The resultant mid-term and long-term needs must propel all sectors, including health,<br />
into rapid action. The UCL–Lancet Commission on Migration and Health report highlighted evidence-based<br />
approaches to address the health needs of forcibly displaced individuals.2 Although the initial response of<br />
the EU agreeing to a uniform policy of settlement, work, and welfare rights for those forcibly displaced is<br />
welcomed,3 implementation of these policies, without restrictions, red tape, or xenophobia and racism is by<br />
no means assured.2,4 The COVID-19 pandemic illuminated the need to strengthen health systems and reduce<br />
disparities in access to and quality of care for migrant groups.5 As the crisis in Ukraine becomes protracted,<br />
access to health care could be at further risk because nations have varying levels of preparedness and<br />
reception, and variable health systems, particularly in neighbouring countries such as Poland, Slovakia,<br />
Bulgaria, and the Czech Republic (Czechia), which will be strained by the large numbers of people arriving from<br />
Ukraine. These countries will need increased support, including financial support, from other countries. The<br />
Ukrainian crisis will test political solidarity, health system planning and capacity, and the global community’s<br />
ability to keep the commitment to universal health coverage.<br />
Read the article: Meeting the health challenges of displaced populations from Ukraine<br />
Calendar<br />
Resources<br />
29
OUR PEOPLE,<br />
OUR MISSION<br />
VIDEO OF THE MONTH<br />
https://youtu.be/RN81h85V6D4<br />
Global Health<br />
<strong>eMagazine</strong><br />
<strong>April</strong> 2022<br />
Watch this video!!<br />
Bani Adam by Saadi Shirazi<br />
Highlights<br />
Perspectives<br />
Behind the Scenes<br />
Announcements<br />
Spotlight<br />
Reflections<br />
Nursing Division<br />
SARS COV-2 Pandemic<br />
and Us<br />
Clinical Case Report<br />
A New Column<br />
Global Health and the Arts<br />
Articles of the Month<br />
Videos of the Month<br />
Calendar<br />
Resources<br />
Rose Schwartz<br />
30
OUR PEOPLE,<br />
OUR MISSION<br />
GLOBAL HEALTH FAMILY<br />
Global Health<br />
<strong>eMagazine</strong><br />
<strong>April</strong> 2022<br />
Watch this video!!<br />
Bani Adam by Saadi Shirazi<br />
Highlights<br />
Perspectives<br />
Eseniy Ziganshina<br />
Henry Scholand<br />
Behind the Scenes<br />
Announcements<br />
Spotlight<br />
Reflections<br />
Nursing Division<br />
SARS COV-2 Pandemic<br />
and Us<br />
Clinical Case Report<br />
A New Column<br />
Global Health and the Arts<br />
Articles of the Month<br />
Riley Wallace with Poppy<br />
Willow and Poppy<br />
Videos of the Month<br />
Calendar<br />
Resources<br />
Click here to visit the Nuvance<br />
Health Global Health Program<br />
COVID-19 Resource Center<br />
31
OUR PEOPLE,<br />
OUR MISSION<br />
CALENDAR OF EVENTS<br />
Global Health<br />
<strong>eMagazine</strong><br />
<strong>April</strong> 2022<br />
Watch this video!!<br />
Bani Adam by Saadi Shirazi<br />
Nuvance Health<br />
March 2: Zoom meeting with Dilyara Nurkhametova, Director of the AUC/RUSM Global<br />
Health Collaboration to discuss the virtual GH elective and potential reopening of<br />
international global health sites in the future.<br />
March 2: Meeting with Dr. Rastegar to discuss the decolonizing global health panel at CUGH.<br />
March 2: Meeting with Dr. Swapnil Parve to discuss selection of international sites for resuming the<br />
global health clinical rotations.<br />
March 2: Meeting with Dr. Stephen Scholand to discuss content and format of GH Bridge at<br />
Danbury Hospital and potential opening of Chiricahua Health Center in Douglass, Arizona for<br />
medical students in summer 2022.<br />
March 3: Weekly meeting with Wendi Cuscina, Manager of the GHP.<br />
March 3: Meeting with Dr. Stephen Scholand to follow up on GH Bridge at Danbury Hospital.<br />
Highlights<br />
Perspectives<br />
Behind the Scenes<br />
Announcements<br />
Spotlight<br />
Reflections<br />
Nursing Division<br />
SARS COV-2 Pandemic<br />
and Us<br />
Clinical Case Report<br />
A New Column<br />
Global Health and the Arts<br />
Articles of the Month<br />
Videos of the Month<br />
Calendar<br />
Resources<br />
March 7: First meeting with the Director of the Scientific Committee of the United Nations General<br />
Assembly which will be held in September 2022 to discuss putting together a panel for this<br />
conference.<br />
March 8: Weekly phone meeting with Audree Frey, Coordinator of the GHP at UVMLCOM.<br />
March 9: Meeting with members of the Compliance Office.<br />
March 9: Meeting with Swapnil Parve to discuss the reopening of the DMIMS, India for medical<br />
students.<br />
March 9: Meeting with a RUSM student to discuss a potential research project.<br />
March 12: Meeting with CUGH 2022 Decolonizing Global Health panelists as well as Dr. Rastegar<br />
and Dr. Sewankambo.<br />
March 13: Meeting with Dr. Stephen Scholand to review his new role as course director of GH Bridge<br />
at Danbury Hospital.<br />
March 15: Meeting with Drs. Dilyara Nurkhametova, Elina, and Swapnil Parve to discuss reopening<br />
of a few international sites for AUC and RUSM students this summer.<br />
March 15: Meeting with Dr. Judith Lewis, Director of Global Mental Health at UVMLCOM and Dr.<br />
Noeline Nakasujja to interview new Rudy Ruggles Scholars in Global Health.<br />
March 15: Meeting with Dr. Bulat Ziganshin to explore the potential date of his employment with<br />
Nuvance Health.<br />
March 29: Meeting with Drs. Dilyara Nurkhametova, Elina, and Swapnil Parve to follow up on<br />
resumption of international travel for AUC and RUSM students.<br />
March 30: Meeting with four CT Institute primary care residents and one resident from Danbury<br />
Hospital’s internal medicine residency program who are interested in participating in the six-week<br />
GH elective in Uganda in spring 2023.<br />
UVMLCOM<br />
March 14: Global Health Leadership Team meeting<br />
March 18: Match Day – our alumni had impressive matches! See list here.<br />
Week of March 28: CUGH – multiple contributions from LCOM faculty and students Irene Sue won<br />
the Lancet Global Health-CUGH Best Student Poster for the track: Global Health Education<br />
32<br />
Calendar continued on next page >>
OUR PEOPLE,<br />
OUR MISSION<br />
Global Health<br />
<strong>eMagazine</strong><br />
March 28: Global Health Leadership Team meeting<br />
<strong>April</strong> 1: Mariah/Audree strategic planning meeting<br />
<strong>April</strong> 11: Global Health Leadership Team meeting<br />
Mid-<strong>April</strong> (date TBD): Global Health Informational Meeting for Class of 2025 to discuss travel<br />
opportunities for summer 2022!<br />
<strong>April</strong> 25: Global Health Leadership Team meeting<br />
<strong>April</strong> 2022<br />
Watch this video!!<br />
Bani Adam by Saadi Shirazi<br />
AUC/RUSM<br />
Online GH course:<br />
March 21 - <strong>April</strong> 1: course 5, 16 students (1 AUC and 15 RUSM)<br />
Two online courses are planned for <strong>April</strong>:<br />
<strong>April</strong> 4 - <strong>April</strong> 15<br />
<strong>April</strong> 18 - <strong>April</strong> 29<br />
Highlights<br />
Perspectives<br />
Behind the Scenes<br />
March 20: Touch-base meeting with Dr Elina Mukhametshina<br />
March 28: Poster presentations at CUGH conference<br />
Announcements<br />
Spotlight<br />
Reflections<br />
Nursing Division<br />
SARS COV-2 Pandemic<br />
and Us<br />
Clinical Case Report<br />
A New Column<br />
Global Health and the Arts<br />
Articles of the Month<br />
Videos of the Month<br />
Calendar<br />
Resources<br />
Tucson (Stephen Scholand)<br />
33
OUR PEOPLE,<br />
OUR MISSION<br />
RESOURCES<br />
Global Health<br />
<strong>eMagazine</strong><br />
<strong>April</strong> 2022<br />
Watch this video!!<br />
Bani Adam by Saadi Shirazi<br />
Highlights<br />
Perspectives<br />
Behind the Scenes<br />
Announcements<br />
Spotlight<br />
Reflections<br />
Nursing Division<br />
SARS COV-2 Pandemic<br />
and Us<br />
Photos and Reflections 2021<br />
Global Health & the Arts<br />
Nuvance Health and UVMLCOM Global Health<br />
Website<br />
COVID-19 Resource Center<br />
Nuvance Health and UVMLCOM Annual Report 2020<br />
AUC/RUSM Annual Report 2018<br />
Cases and Reflections from Mulago<br />
Climb for a Cause 2018<br />
Climb for a Cause 2019<br />
Ebola: Sequences on Light and Dark<br />
Ebola: Two Doctors Respond to the 2014 Ebola<br />
Epidemic in Liberia: A Personal Account<br />
Global Health Annual Reports<br />
Global Health Conference 2019 Photos<br />
Global Health Conference 2019 Videos<br />
Global Health Conference 2019 Book<br />
Global Health Diaries and Newsletters 2015-2016<br />
Global Health Diaries and Newsletters 2016-2017<br />
Global Health Diaries and Newsletters 2017-2018<br />
Global Health Diaries and <strong>eMagazine</strong>s 2018-2019<br />
Global Health <strong>eMagazine</strong>s 2020-2021<br />
Global Health Diaries 2020-2021<br />
Global Health Reflections and Photos 2017 and 2018<br />
Global Health Reflections and Photos 2019<br />
Ethical Dilemmas book<br />
Global Health Program Website<br />
Global Health at WCHN Facebook<br />
Ho Chi Minh City and Cho Ray Hospital<br />
The Homestay Model of Global Health Program video<br />
Kasensero Uganda<br />
Katanga video<br />
Nuvance/MakCHS Global Health Information Center<br />
Booklet<br />
Paraiso and the PAP Hospital<br />
Photographs from Uganda, by photojournalist Tyler<br />
Sizemore<br />
Presentations By Global Health Scholars<br />
Previous issues of the Global Health <strong>eMagazine</strong><br />
Program Partners<br />
Publications<br />
Site Specific Information<br />
Tropical Medicine Booklets (101, and 202)<br />
Tropical Medicine Spanish 101<br />
Tropical Medicine Modules<br />
Tropical Medicine Courses<br />
The World of Global Health book<br />
The World of Global Health Video<br />
Words of Encouragement<br />
UVM Larner College of Medicine Blog<br />
Participant Guide in Global Health, Thailand<br />
Cho Ray International Student Handbook<br />
DRC Facing a New Normal<br />
Photos and Reflections 2019<br />
Coronavirus 2019 Important clinical considerations for<br />
Patients & Health care Providers<br />
Clinical Case Report<br />
A New Column<br />
Global Health and the Arts<br />
Articles of the Month<br />
Interviews<br />
A Connecticut Doctor in Africa, by journalist Mackenzie<br />
Riggs<br />
Majid Sadigh, MD Interview Regarding Ebola in Liberia<br />
(Video)<br />
My Heart Burns: Three Words Form a Memoir (Video)<br />
Two UVM Docs Combat Ebola in Liberia (Article)<br />
Videos of the Month<br />
Calendar<br />
Resources<br />
34