Escaping the Scalpel
In-depth evidence to change clinical practice for patients with a degenerative meniscal tear. By Julia C.A. Noorduyn
In-depth evidence to change clinical practice for patients with a degenerative meniscal tear.
By Julia C.A. Noorduyn

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
12<br />
CHAPTER I<br />
ment effectiveness. [31, 32] Therefore, <strong>the</strong> old guideline does not make any statement on <strong>the</strong><br />
treatment for degenerative meniscal tears.[32] Whereas, <strong>the</strong> current Dutch, but also international<br />
guidelines, recommend against surgical treatment for middle aged and older patients<br />
with a degenerative meniscus tear and nonsurgical management should last for at least 3<br />
months.[1, 29, 31]<br />
Despite that <strong>the</strong> guidelines recommend nonsurgical treatment, meniscus surgery is still frequently<br />
performed in middle aged and older patients with a meniscus tear.[4, 28] It seems<br />
that with 25.992 (75%) of <strong>the</strong> arthroscopic partial meniscectomies performed in patients<br />
over 40 years old in 2005, and still 20.833 (70%) in 2014, clinicians are not convinced by <strong>the</strong><br />
evidence and uncertain about <strong>the</strong> quality of <strong>the</strong> current evidence.[3, 5] A non-inferiority design<br />
can fill this knowledge gap and provide high quality evidence that is need to empower<br />
clinicians in <strong>the</strong>ir evidence-based treatment decisions.[26]<br />
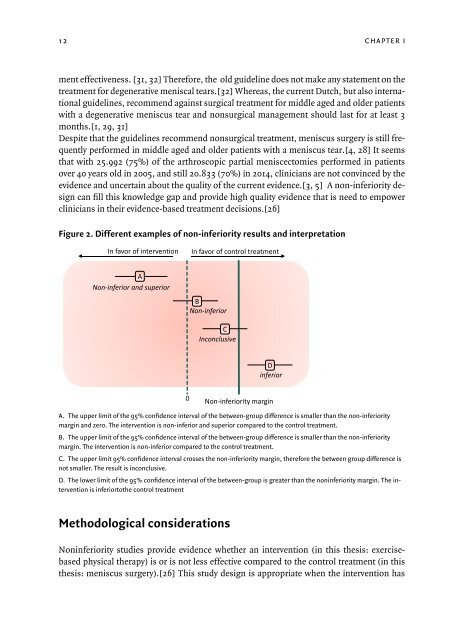
Figure 2. Different examples of non-inferiority results and interpretation<br />
In favor of intervention<br />
In favor of control treatment<br />
A<br />
Non-inferior and superior<br />
B<br />
Non-inferior<br />
C<br />
Inconclusive<br />
D<br />
inferior<br />
0<br />
Non-inferiority margin<br />
A. The upper limit of <strong>the</strong> 95% confidence interval of <strong>the</strong> between-group difference is smaller than <strong>the</strong> non-inferiority<br />
margin and zero. The intervention is non-inferior and superior compared to <strong>the</strong> control treatment.<br />
B. The upper limit of <strong>the</strong> 95% confidence interval of <strong>the</strong> between-group difference is smaller than <strong>the</strong> non-inferiority<br />
margin. The intervention is non-inferior compared to <strong>the</strong> control treatment.<br />
C. The upper limit 95% confidence interval crosses <strong>the</strong> non-inferiority margin, <strong>the</strong>refore <strong>the</strong> between group difference is<br />
not smaller. The result is inconclusive.<br />
D. The lower limit of <strong>the</strong> 95% confidence interval of <strong>the</strong> between-group is greater than <strong>the</strong> noninferiority margin. The intervention<br />
is inferiorto<strong>the</strong> control treatment<br />
Methodological considerations<br />
Noninferiority studies provide evidence whe<strong>the</strong>r an intervention (in this <strong>the</strong>sis: exercisebased<br />
physical <strong>the</strong>rapy) is or is not less effective compared to <strong>the</strong> control treatment (in this<br />
<strong>the</strong>sis: meniscus surgery).[26] This study design is appropriate when <strong>the</strong> intervention has