

Female Genital Mutilation - World Health Organization
Female Genital Mutilation - World Health Organization
Female Genital Mutilation - World Health Organization

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
78<br />
FEMALE GENITAL MUTILATION<br />
STUDENT MANUAL<br />
Infiltrate 2–3 mls of local anaesthetic into the area<br />
where the cut will be made, along the scar and in both<br />
sides of the scar (see figure 4.3).<br />
Figure 4.3: Infiltrating the scar area with local<br />
anaesthetic<br />
● With your finger or dilator inside the scar,<br />
introduce the scissors and cut the scar alongside<br />
the finger or fingers to avoid injury to the adjacent<br />
tissues (or to the baby, if the procedure is done<br />
during labour).<br />
● The cut should be made along the mid-line of the<br />
scar towards the pubis (see figure 4.4).<br />
● Take care that you do not cause injury to the<br />
structures along the scar. It is common with type<br />
III FGM to find the structures below the scar<br />
intact, e.g. clitoris and labia minora.<br />
● Incise the mid-line to expose the urethral opening.<br />
(see figure 4.5) Do not incise beyond the urethra.<br />
Extending the incision forward may cause<br />
haemorrhage, which is difficult to control. A cut of<br />
about 5-7 cm towards the urethra is usually<br />
appropriate. Generally speaking there is little<br />
bleeding for the relatively avascular scar tissue.<br />
Figure 4.4: Cutting open the scar<br />
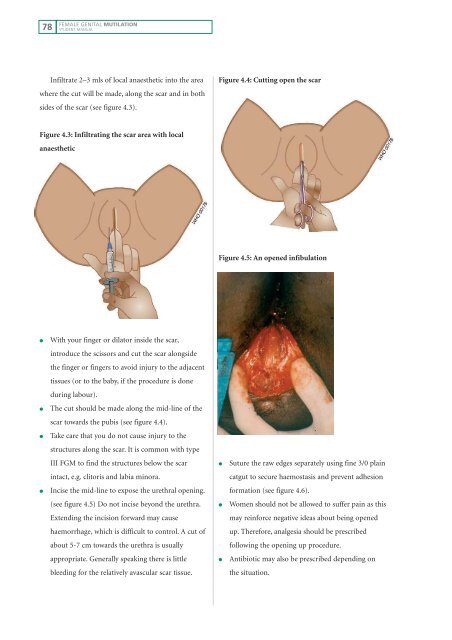
Figure 4.5: An opened infibulation<br />
● Suture the raw edges separately using fine 3/0 plain<br />
catgut to secure haemostasis and prevent adhesion<br />
formation (see figure 4.6).<br />
● Women should not be allowed to suffer pain as this<br />
may reinforce negative ideas about being opened<br />
up. Therefore, analgesia should be prescribed<br />
following the opening up procedure.<br />
● Antibiotic may also be prescribed depending on<br />
the situation.














