

Download PDF - Medical Tourism Magazine
Download PDF - Medical Tourism Magazine
Download PDF - Medical Tourism Magazine

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
satisfaction, clinical treatment, and investment in information<br />
technology.<br />
Some substantial payments are being made. In addition, on August<br />
24 Blue Cross of California, a subsidiary of WellPoint, announced<br />
that is was rewarding 126 physician groups a total of $69 million in<br />
bonuses for performance in 2006. About a week earlier, Blue Shield<br />
of California announced that it distributed $31 million in bonus<br />
money.<br />
What do Physician Groups Fear about P4P?<br />
� Getting used in a “shell game” manipulated by the payors<br />
� To date there is no long term commitment to P4P by payors<br />
� Measures are not geographically or socio-economically fair<br />
or reliable<br />
� P4P compliance is too burdensome and expensive<br />
� Public reporting can increase liability<br />
� Cost controls will masquerade as quality and initiatives<br />
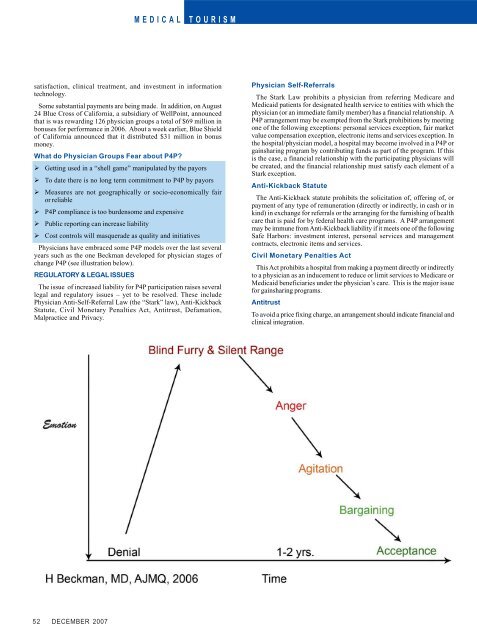
Physicians have embraced some P4P models over the last several<br />
years such as the one Beckman developed for physician stages of<br />
change P4P (see illustration below).<br />
REGULATORY & LEGAL ISSUES<br />
The issue of increased liability for P4P participation raises several<br />
legal and regulatory issues – yet to be resolved. These include<br />
Physician Anti-Self-Referral Law (the “Stark” law), Anti-Kickback<br />
Statute, Civil Monetary Penalties Act, Antitrust, Defamation,<br />
Malpractice and Privacy.<br />
52 DECEMBER 2007<br />
MEDICAL TOURISM<br />
Physician Self-Referrals<br />
The Stark Law prohibits a physician from referring Medicare and<br />
Medicaid patients for designated health service to entities with which the<br />
physician (or an immediate family member) has a financial relationship. A<br />
P4P arrangement may be exempted from the Stark prohibitions by meeting<br />
one of the following exceptions: personal services exception, fair market<br />
value compensation exception, electronic items and services exception. In<br />
the hospital/physician model, a hospital may become involved in a P4P or<br />
gainsharing program by contributing funds as part of the program. If this<br />
is the case, a financial relationship with the participating physicians will<br />
be created, and the financial relationship must satisfy each element of a<br />
Stark exception.<br />
Anti-Kickback Statute<br />
The Anti-Kickback statute prohibits the solicitation of, offering of, or<br />
payment of any type of remuneration (directly or indirectly, in cash or in<br />
kind) in exchange for referrals or the arranging for the furnishing of health<br />
care that is paid for by federal health care programs. A P4P arrangement<br />
may be immune from Anti-Kickback liability if it meets one of the following<br />
Safe Harbors: investment interest, personal services and management<br />
contracts, electronic items and services.<br />
Civil Monetary Penalties Act<br />
This Act prohibits a hospital from making a payment directly or indirectly<br />
to a physician as an inducement to reduce or limit services to Medicare or<br />
Medicaid beneficiaries under the physician’s care. This is the major issue<br />
for gainsharing programs.<br />
Antitrust<br />
To avoid a price fixing charge, an arrangement should indicate financial and<br />
clinical integration.