Streptococcus bovis - Gundersen Lutheran Health System
Streptococcus bovis - Gundersen Lutheran Health System
Streptococcus bovis - Gundersen Lutheran Health System

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
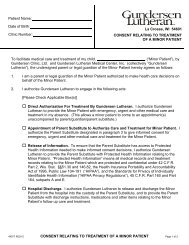
figure 1. Axial reformatted computed tomographic scan of the<br />
abdomen and pelvis performed on the day of presentation. The<br />
appendix appears normal, and no other pathology is present to<br />
explain the patient’s pain.<br />
from the appendiceal orifice (Figure 2). This was aspirated and sent<br />
to the laboratory, where analysis detected a large number of white<br />
blood cells, gram-negative rods, and gram-positive cocci. Results of<br />
the biopsy of the mucosa at the base of the appendix demonstrated<br />
mild nonspecific chronic and focal acute inflammation.<br />
The general surgeon on call was notified and observed the<br />
appendiceal findings at colonoscopy. The patient’s generally<br />
benign condition and the duration of the symptoms were<br />
taken into consideration, as was the interesting finding of freely<br />
flowing pus from the appendiceal orifice. The surgeon elected to<br />
observe the patient over the weekend and repeat a CT scan if his<br />
symptoms persisted.<br />
The patient remained symptomatic and underwent a repeat CT<br />
scan. The radiologist noted that this scan was similar in appearance<br />
to the patient’s previous studies and that the appendix was fluidfilled,<br />
although the walls were not thickened and there were no<br />
inflammatory changes. The remainder of the abdomen and pelvis<br />
appeared normal.<br />
The following day, the patient underwent laparoscopic<br />
appendectomy. Intraoperative findings included an enlarged,<br />
inflamed appendix and mild mesenteric scarring around the<br />
CoLonoSCopiC diAGnoSiS of AppendiCitiS<br />
terminal ileum. No signs of active Crohn disease or ulcerative colitis<br />
were identified. No signs of a Meckel diverticulum were present.<br />
Routine pathologic evaluation of the appendix later confirmed the<br />
diagnosis of acute suppurative appendicitis with benign lymphoid<br />
hyperplasia. The patient was discharged home after a brief and<br />
benign recovery.<br />
Just over a month later, the patient was seen in the emergency<br />
department for recurrent abdominal pain, which quickly resolved<br />
without intervention. His postoperative course had been benign<br />
until that point, with the exception of a knee joint effusion, possibly<br />
related to trauma from playing basketball. Since that episode 24<br />
months ago, the patient has reported no abdominal pain.<br />
To our knowledge, this is the first report of colonoscopic<br />
diagnosis of appendicitis in a patient with known ulcerative colitis<br />
and possible Crohn disease, which significantly confounded the<br />
evaluation.<br />
diSCuSSion<br />
In 1994, Said et al reported a case of atypical appendicitis that<br />
was diagnosed by colonoscopy. The patient had experienced<br />
abdominal pain and fever for 2 weeks and was hospitalized and<br />
treated nonoperatively. The results of laboratory studies were<br />
consistent with inflammation. Workup included ultrasonography<br />
and upper endoscopy. On the third day after admission,<br />
colonoscopy was performed, pus was aspirated from the<br />
appendiceal orifice, and the patient’s symptoms resolved within<br />
a day. Interval appendectomy was performed 5 months later and<br />
confirmed a previous diagnosis of appendicitis. 14<br />
figure 2. Colonoscopy demonstrates pus from the appendiceal os,<br />
slight inflammation near the base of the appendix.<br />
<strong>Gundersen</strong> <strong>Lutheran</strong> Medical Journal • Volume 6, Number 1, June 2009 15