Streptococcus bovis - Gundersen Lutheran Health System
Streptococcus bovis - Gundersen Lutheran Health System
Streptococcus bovis - Gundersen Lutheran Health System

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
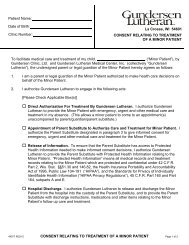
figure 2. Computed tomographic scan with contrast illustrating<br />
complex tubo-ovarian abscess (white arrow).<br />
While our patient had left-sided OVT, a right-sided<br />
predominance has been reported, probably attributable to the<br />
immediate postpartum retrograde flow of venous blood down<br />
the left ovarian vein, through the pelvis, and up the right ovarian<br />
vein. 6,7 With thrombosis, the clotted vein can be imaged along the<br />
psoas muscle to the vena cava on the right or left renal vein, as in<br />
our case. The clot may extend into the vena cava, and pulmonary<br />
embolus may ensue. Imaging studies reveal sensitivities of 100%,<br />
92%, and 50% for CT scans, magnetic resonance imaging scans,<br />
and ultrasonograms, respectively. 8<br />
Blood cultures usually remain negative for pathogens, with<br />
positive cultures seen in only about 3% of patients.1 The bacteria<br />
most commonly associated with OVT reflect the vaginal origin of<br />
these infections: enteric gram-negative rods, including Escherichia<br />
coli, Enterobacter and Klebsiella species, along with microaerophilic<br />
streptococci, and anaerobic bacteria such as Peptostreptococcus,<br />
Bacteroides, and Prevotella species. 1,3 Antimicrobial treatment of<br />
OVT should be directed against these gastrointestinal/genitourinary<br />
facultative and anaerobic flora.<br />
A genetic hypercoaguable state in has been found in 50%<br />
of women with OVT. 9 Our patient had no family history of<br />
thromboembolic disease, thus genetic causes for a hypercoagulable<br />
state were not evaluated. Literature approximately 40 years ago<br />
indicated that anticoagulation had replaced the surgical ligation of<br />
the vena cava or ovarian veins to prevent pulmonary emboli. 3<br />
More recent literature has shown that resolution of fever and<br />
length of hospitalization were not significantly different in women<br />
treated with antibiotics alone versus those treated with antibiotics<br />
and anticoagulation, probably due to a spectrum bias of earlier<br />
detection and, therefore, milder cases. 10<br />
poSt–CeSAreAn deLiVery SeptiC oVAriAn Vein throMboSiS<br />
Despite these recent reports, a short course of anticoagulation<br />
is often given due to concerns of vena cava thrombosis or<br />
pulmonary emboli seen in approximately 13% of OVT, 6 although<br />
the type and duration of anticoagulation for OVT remains<br />
controversial. 7,11,12 Until better evidence is available, the authors<br />
believe anticoagulation should be considered until the patient is<br />
ambulating and asymptomatic, and for 3 to 6 months in cases<br />
complicated by pulmonary emboli. If warfarin is given to a woman<br />
who breast feeds, Vitamin K supplement and coagulation testing<br />
of her infant is considered prudent.<br />
referenCeS<br />
1. Brown TK, Munsick RA. Puerperal ovarian vein thrombophlebitis: a syndrome.<br />
Am J Obstet Gynecol. 1971;109(2):263-273.<br />
2. Dunnihoo DR, Gallaspy JW, Wise RB, Otterson WN. Postpartum ovarian vein<br />
thrombophlebitis: a review. Obstet Gynecol Surv. 1991;46(7):415-427.<br />
3. Josey WE, Staggers SR,Jr. Heparin therapy in septic pelvic thrombophlebitis: a<br />
study of 46 cases. Am J Obstet Gynecol. 1974;120(2):228-233.<br />
4. Garcia J, Aboujaoude R, Apuzzio J, Alvarez JR. Septic pelvic thrombophlebitis:<br />
diagnosis and management. Infect Dis Obstet Gynecol. doi:10.1155/<br />
IDOG/2006/15614.<br />
5. Witlin AG, Mercer BM, Sibai BM. Septic pelvic thrombophlebitis or refractory<br />
postpartum fever of undetermined etiology. J Matern Fetal Med. 1996;5(6):<br />
355-358.<br />
6. Munsick RA, Gillanders LA. A review of the syndrome of puerperal ovarian vein<br />
thrombophlebitis. Obstet Gynecol Surv. 1981;36(2):57-66.<br />
7. Kominiarek MA, Hibbard JU. Postpartum ovarian vein thrombosis: an update.<br />
Obstet Gynecol Surv. 2006;61(5):337-342.<br />
8. Twickler DM, Setiawan AT, Evans RS, et al. Imaging of puerperal septic<br />
thrombophlebitis: prospective comparison of MR imaging, CT, and sonography.<br />
AJR Am J Roentgenol. 1997;169(4):1039-1043.<br />
9. Salomon O, Apter S, Shaham D, et al. Risk factors associated with postpartum<br />
ovarian vein thrombosis. Thromb Haemost. 1999;82(3):1015-1019.<br />
10. Brown CE, Stettler RW, Twickler D, Cunningham FG. Puerperal septic pelvic<br />
thrombophlebitis: incidence and response to heparin therapy. Am J Obstet<br />
Gynecol. 1999;181(1):143-148.<br />
11. Beigi RH, Wiensenfeld HC. Enoxaparin for postpartum ovarian vein thrombosis.<br />
A case report. J Reprod Med. 2004;49(1):55-57.<br />
12. Ortin X, Ugarriza A, Espax RM, et al. Postpartum ovarian vein thrombosis.<br />
Thromb Haemost. 2005;93(5):1004-1005.<br />
<strong>Gundersen</strong> <strong>Lutheran</strong> Medical Journal • Volume 6, Number 1, June 2009 25