R. Gottschall, Die fiberoptische Intubation + Sicherung des Atemweges
R. Gottschall, Die fiberoptische Intubation + Sicherung des Atemweges
R. Gottschall, Die fiberoptische Intubation + Sicherung des Atemweges

Sie wollen auch ein ePaper? Erhöhen Sie die Reichweite Ihrer Titel.
YUMPU macht aus Druck-PDFs automatisch weboptimierte ePaper, die Google liebt.
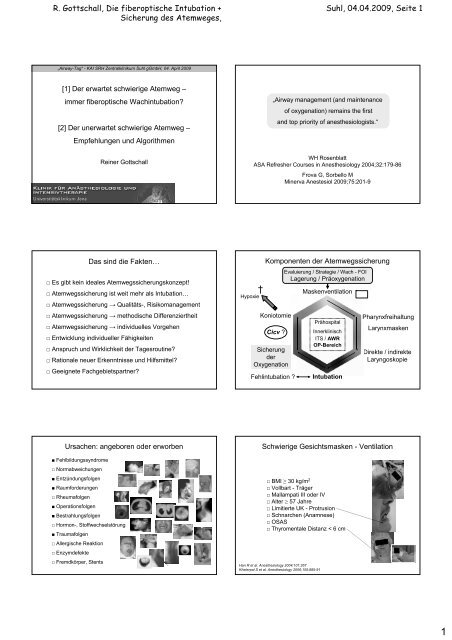
R. <strong>Gottschall</strong>, <strong>Die</strong> <strong>fiberoptische</strong> <strong>Intubation</strong> +<br />
<strong>Sicherung</strong> <strong>des</strong> <strong>Atemweges</strong>,<br />
„Airway-Tag“ - KAI SRH Zentralklinikum Suhl gGmbH, 04. April 2009<br />
[1] Der erwartet schwierige Atemweg –<br />
immer <strong>fiberoptische</strong> Wachintubation?<br />
[2] Der unerwartet schwierige Atemweg –<br />
Empfehlungen und Algorithmen<br />
Reiner <strong>Gottschall</strong><br />
Das sind die Fakten…<br />
□ Es gibt kein ideales Atemwegssicherungskonzept!<br />
□ Atemwegssicherung ist weit mehr als <strong>Intubation</strong>…<br />
□ Atemwegssicherung → Qualitäts-, Risikomanagement<br />
□ Atemwegssicherung → methodische Differenziertheit<br />
□ Atemwegssicherung → individuelles Vorgehen<br />
□ Entwicklung individueller Fähigkeiten<br />
□ Anspruch und Wirklichkeit der Tagesroutine?<br />
□ Rationale neuer Erkenntnisse und Hilfsmittel?<br />
□ Geeignete Fachgebietspartner?<br />
Ursachen: angeboren oder erworben<br />
■ Fehlbildungssyndrome<br />
□ Normabweichungen<br />
■ Entzündungsfolgen<br />
■ Raumforderungen<br />
□ Rheumafolgen<br />
■ Operationsfolgen<br />
■ Bestrahlungsfolgen<br />
□ Hormon-, Stoffwechselstörung<br />
■ Traumafolgen<br />
□ Allergische Reaktion<br />
□ Enzymdefekte<br />
□ Fremdkörper, Stents<br />
Suhl, 04.04.2009, Seite 1<br />
„Airway management (and maintenance<br />
of oxygenation) remains the first<br />
and top priority of anesthesiologists.“<br />
WH Rosenblatt<br />
ASA Refresher Courses in Anesthesiology 2004;32:179-86<br />
Frova G, Sorbello M<br />
Minerva Anestesiol 2009;75:201-9<br />
†<br />
Hypoxie<br />
Komponenten der Atemwegssicherung<br />
Koniotomie<br />
Cicv ?<br />
<strong>Sicherung</strong><br />
der<br />
Oxygenation<br />
Fehlintubation ?<br />
Evaluierung / Strategie / Wach - FOI<br />
Lagerung / Präoxygenation<br />
Maskenventilation<br />
Prähospital<br />
Innerklinisch<br />
ITS / AWR<br />
OP-Bereich<br />
<strong>Intubation</strong><br />
Pharynxfreihaltung<br />
Larynxmasken<br />
Direkte / indirekte<br />
Laryngoskopie<br />
Schwierige Gesichtsmasken - Ventilation<br />
□ BMI ≥ 30 kg/m 2<br />
□ Vollbart - Träger<br />
□ Mallampati III oder IV<br />
□ Alter ≥ 57 Jahre<br />
□ Limitierte UK - Protrusion<br />
□ Schnarchen (Anamnese)<br />
□ OSAS<br />
□ Thyromentale Distanz < 6 cm<br />
Han R et al. Anesthesiology 2004;101:267<br />
Kheterpal S et al. Anesthesiology 2006;105:885-91<br />
1
R. <strong>Gottschall</strong>, <strong>Die</strong> <strong>fiberoptische</strong> <strong>Intubation</strong> +<br />
<strong>Sicherung</strong> <strong>des</strong> <strong>Atemweges</strong>,<br />
Evaluierung <strong>des</strong> schwierigen <strong>Atemweges</strong> (n. Benumof)<br />
1. Schneidezahn - Relation passiv (kein Überstand oben)<br />
2. Schneidezahn - Relation aktiv (UK-Mobilität vorhanden)<br />
3. Schneidezahn - Distanz (> 3 cm)<br />
4. Oropharyngeale Relation (Mallampati ≤ II)<br />
5. Gaumenenge, -form (weit, flach)<br />
6. Länge Submandibularraum (n. Patil ≥ 5 cm)<br />
7. Obere Schneidezähne (kurz, fest)<br />
8. Compliance Submandibularraum (weich, dehnbar)<br />
9. Länge / Dicke <strong>des</strong> Halses (?)<br />
10. Mobilität von Kopf / Hals („Schnüffelposition“)<br />
11. Subglottischer Raum (?)<br />
Anamnese - Schnarchen / OSAS - Dysphagie - Dysarthrie -<br />
Stridor - Mundatmer - Zungenmobilität - Lückengebiss -<br />
Notfallpatient - Nichtkooperative - Kanülen-, Stentträger -<br />
Bildgebung / Endoskopie - Radiatio - Atemfunktion - Vollbart -<br />
Apnoeintoleranz -…<br />
„Unter den Blinden ist<br />
der Einäugige König“<br />
Erasmus von Rotterdam 1469-1536<br />
Vorteile (Wachintubation)<br />
□ Spontanatmung = Sicherheit<br />
□ Schutzreflexe<br />
□ Inspektion vor / nach <strong>Intubation</strong><br />
□ Zugangswege<br />
□ Erfolgsrate↑<br />
□ Traumapotenzial↓<br />
□ Vegetative Stimulation↓<br />
□ Nutzungsdistanz, -vielfalt<br />
1<br />
2<br />
3<br />
Suhl, 04.04.2009, Seite 2<br />
Evaluierung Multifaktor-Risiko-Index<br />
<strong>des</strong> schwierigen Atemwegs<br />
Arnè J et al. Br J Anaesth 1998;80:140-6<br />
(Multifaktor-Risiko-Index)<br />
≥ 11<br />
Indikationen (Wachintubation)<br />
Copyright: Dr. S. Simon, KAI FSU Jena<br />
□ Erwartet schwieriger Atemweg (strukturell, funktionell)<br />
□ Unerwartet schwieriger Atemweg (Aufwachen, Verschieben)<br />
□ Erhalt der Spontanatmung (MMS - Prävention)<br />
□ Aspirationsrisiko<br />
□ Neurologische Beurteilung<br />
□ Prävention von <strong>Intubation</strong>sschäden<br />
□ Extreme Patientenposition<br />
□ Ausbildung, Training<br />
Rosenblatt WH J Clin Anesth 2004;16:312-16<br />
Langeron O et al. Critical Care 2008;10:243-7<br />
Nachteile (Wachintubation)<br />
□ Patientenkooperation erforderlich<br />
□ Diskomfort möglich !<br />
□ Laryngeale Tubuspassage „blind“<br />
□ Zeitaufwand (<strong>Intubation</strong>, Aufbereitung)<br />
□ Komplexität, Handhabung (Lernkurve, Assistenz)<br />
□ Methodische Grenzen (u.a. massives Gesichts-Hals-Trauma)<br />
4<br />
5<br />
6<br />
7<br />
2
R. <strong>Gottschall</strong>, <strong>Die</strong> <strong>fiberoptische</strong> <strong>Intubation</strong> +<br />
<strong>Sicherung</strong> <strong>des</strong> <strong>Atemweges</strong>,<br />
Zugangswege (Wachintubation) Vorbereitung (Checkliste)<br />
Schleimhautanästhetika<br />
(n. Dr. F. Stanzel, Hemer*)<br />
□ Nasal<br />
□ Oral<br />
□ Luftbrücke<br />
□ Stomal<br />
□ Andere<br />
□ Lidocain 2 - 4% 3 - 4 mg / kg (Erwachsene)<br />
1 - 2% 4,5 mg / kg (Kinder)<br />
□ Lidocain 3% + Phenylephrin 0.25% (Erwachsene, max. 1 ml nasal)<br />
□ Alternative - Tetracain (Ester) *<br />
z.B. Acoin ® - Pumpspray vs. Lösung (COMBUSTIN)<br />
~ 0,8 mg / kg (?) Evaluierung nicht abgeschlossen<br />
Schleimhautanästhesie mittels FFO laryngotracheal<br />
LA<br />
O 2<br />
(max. 5 L/min)<br />
BF-P40 / LF-2<br />
(OLYMPUS)<br />
□ Oxygenation<br />
□ LA - Menge↓<br />
□ Sicht↑<br />
Suhl, 04.04.2009, Seite 3<br />
□ Aufklärung und individuelle Prämedikation<br />
□ Geeignete Fiberoptik, Lichtquelle und div. Hilfsmittel<br />
□ Patientenmonitoring (EKG, NIBD, SaO2, ggf. EtCO2) □ Sauerstoffgabe<br />
□ Intravenöser Zugang, Absaugvorrichtung<br />
□ Topische Anästhesie<br />
□ Analgosedierung<br />
□ Geeigneter Tubus, Beissring<br />
□ Antibeschlag-, Gleitmittel<br />
Schleimhautanästhesie naso-, oropharyngeal<br />
Mucosal Atomization Device (oral / nasal)<br />
Option: krikothyroidal<br />
Supportive Pharmaka<br />
„conscious sedation“<br />
www.wolfetory.com<br />
www.LMA-Deutschland.de<br />
□↑Patientenkomfort<br />
□ Optimierte Applikation<br />
□ LA - Einsparung<br />
□ Anticholinergikum (Atropin s.c.; Glycopyrrolat i.v.)<br />
□ Midazolam niedrigdosiert p.o. / titriert i.v.<br />
□ Remifentanil - Perfusor* (0,05 - 0,175 µg / kg / min) n. Wirkung !<br />
Bild: Mit Einverständnis <strong>des</strong> Patienten<br />
→ Klinische Zeichen: - subjektives Wärmegefühl<br />
- Spontanatmung (Af ↓ EtCO 2↑)<br />
- Miosis / Augenlidschwere<br />
- BD / Hf ↓<br />
- Hustenreflexdämpfung<br />
Reusche & Egan J Clin Anesth 1999;11:64-8<br />
Puchner W et al. Acta Anaesthesiol Scand 2002;46:350-4<br />
Machata AM et al. Anesth Analg 2003;97:904-8<br />
Beers & Camporesi CNS Drugs 2004;18:1085-104*<br />
Mingo OH et al. Anaesthesia 2008;63:1065-9<br />
3
R. <strong>Gottschall</strong>, <strong>Die</strong> <strong>fiberoptische</strong> <strong>Intubation</strong> +<br />
<strong>Sicherung</strong> <strong>des</strong> <strong>Atemweges</strong>,<br />
Notfallmäßige <strong>fiberoptische</strong> <strong>Intubation</strong> ?<br />
[Postoperatives ventrales Hals-Hämatom; tiefe Halsinfektion]<br />
Tumor-Chirurgie<br />
wach naso-, orotracheal<br />
HWS-Chirurgie<br />
Carotis-Chirurgie<br />
Mediastinitis<br />
Struma-Chirurgie<br />
Methodische Grenzen (Wachintubation)<br />
Submandibularis-<br />
Chirurgie<br />
→ AA, cicv<br />
B 1 ) LMA<br />
C 1 ) FFO / Aintree ®<br />
C 2 ) ETT<br />
□ Anwender, Assistenz, Patient<br />
□ Technik, Hilfsmittel, Aufbereitung<br />
□ Topische Anästhesie, Sedierung<br />
□ Kritische Oxygenation, Zeitdruck<br />
□ Keine Glottisvisualisierung (Distorsion)<br />
□ Rigide Hindernisse, Stenosen, etc<br />
□ Sichtverlust, Absaugkapazität<br />
→ Alternative zwingend: „Plan B“<br />
Wulf H et al. Acta Anaesthesiol Scand 1997;41:1080-2<br />
Hershey MD, Hannenberg AA Anesthesiology 1998;85:479-0<br />
Ho AMH et al. Can J Anaesth 2004;51:838-41<br />
Ho CM et al. Br J Anaesth 2005;94:856-8<br />
Kaneko Y et al. J Clin Anesth 2006;18:135-7<br />
Fiberoptische <strong>Intubation</strong> (Allgemeinanästhesie)<br />
□ <strong>Sicherung</strong> der Oxygenation / Ventilation<br />
□ Erleichterter Atemwegszugang<br />
□ Sekundäre <strong>Intubation</strong> unter Sicht<br />
Suhl, 04.04.2009, Seite 4<br />
Instabile / dysfunktionelle HWS (Trauma)<br />
□ Manuelle in - line Stabilisierung AA / Rel.→ DL*<br />
□ Alternative Laryngoskope / Optiken<br />
□ Fiberoptische Wachintubation<br />
□ Larynxmaske (Fastrach, Classic, ProSeal)<br />
□ Elektive Tracheotomie (LA)<br />
HWS Immobilisierung wesentlicher als <strong>Intubation</strong>stechnik.<br />
Keine Einzeltechnik ist überlegen bzw. unproblematisch<br />
Ghafoor AU et al. J Clin Anesth 2005;17:640-49<br />
Manninen PJ et al. J Neurosurg Anesthesiol 2007;19:190-4<br />
Langford & Leslie J Clin Neuroscience 2009;16:366-72<br />
* Santoni BG et al. Anesthesiology 2008;109:24-31<br />
Alternativen zur <strong>fiberoptische</strong>n Wachintubation<br />
□ Fiberoptische <strong>Intubation</strong> in Narkose / Spontanatmung<br />
Bonnin M et al. Comparison of propofol target-controlled infusion and inhalational sevoflurane for fibreoptic<br />
intubation under spontaneous ventilation. Acta Anaesthesiol Scand 2007;51:54-9<br />
□ Fiberoptische <strong>Intubation</strong> in Narkose nach Katheterkoniotomie<br />
Gerig HJ et al. Prophylactic percutaneous transtracheal catheterisation in the management of patients with<br />
anticipated difficult airways: a case series. Anaesthesia 2005;60:801-5<br />
□ Fiberoptische <strong>Intubation</strong> über Larynxmasken<br />
Koerner IP, Brambrink AM Fiberoptic techniques. Best Pract Res Clin Anaesthesiol 2005;19:611-21<br />
Zura A et al. Use of the Aintree intubation catheter in a patient with an unexpected difficult airway.<br />
Can J Anaesth 2005;52:646-9<br />
Alternativen zur <strong>fiberoptische</strong>n Wachintubation<br />
□ LA / Regionalanästhesie (Plan B erforderlich!)<br />
Soens MA et al. Obstetric anaesthesia for the obese and morbidly obese patient: an ounce of prevention is<br />
worth more than a pound of treatment. Acta Anaesthesiol Scand 2008;52:6-19<br />
□ Selektive chirurgische Koniotomie / Tracheotomie in LA<br />
Schuss U u. Mitarb. <strong>Die</strong> selektive Koniotomie (unveröffentlicht)<br />
Altman KW et al. Urgent surgical airway interventions:…Laryngoscope 2005;115:2101-4<br />
□ Wachintubation mit alternativen Instrumenten<br />
Abramson SI et al. Awake insertion of the Bonfils retromolar intubation fiberscope in five<br />
patients with anticipated difficult airways. Anesth Analg 2008;106:1215-7<br />
□ <strong>Intubation</strong> in Narkose / ± Spontanatmung<br />
Cros AM et al. Anesthesia induction with sevoflurane in adult patients with pedictive signs of difficult intubation.<br />
Ann Fr Anesth Reanim 2002;21:249-55<br />
Caponas G Intubating laryngeal mask airway. Anaesth Intensive Care 2002;30:551-69<br />
4
R. <strong>Gottschall</strong>, <strong>Die</strong> <strong>fiberoptische</strong> <strong>Intubation</strong> +<br />
<strong>Sicherung</strong> <strong>des</strong> <strong>Atemweges</strong>,<br />
Extubation (nach schwieriger <strong>Intubation</strong>)<br />
□ Geplant - Erfüllung funktioneller / anderer Kriterien?<br />
- Präoxygenation / Absaugung / Cuff entblocken<br />
- Tubuswechsler / Aintree - Katheter (FFO)<br />
- LMA<br />
- GM / CPAP (NIV)<br />
- Katheter - Koniotomie / Tracheotomie (temporär)<br />
□ Ungeplant - Algorithmus für schwierigen Atemweg!<br />
Kempen P J Clin Anesth 1999;11:441-4<br />
Hagberg & Regan In: Handbook of Difficult Airway Management. Ed. Hagberg CA, Churchill<br />
Livingstone 2000, p 373-87<br />
Kienzle F In: Airway-Management. Hrsg. Krier & Georgi, Thieme 2001, S. 272-8<br />
de la Linde Valverde CM Rev Esp Anestesiol Reanim 2005;52:557-70<br />
Tubuswechselkatheter - Memo<br />
□ Geeignete Größe / Länge vorhalten (ETT / DLT)<br />
□ Niemals gegen Widerstand / zu tief platzieren<br />
□ Barotraumarisiko (bei manuell-getriggerter JV!)<br />
□ Aspirationsrisiko<br />
□ Nicht für Tracheostoma - Management<br />
□ Training am Phantom<br />
Benumof JL Anesthesiology 1999;91:342-344<br />
<strong>Gottschall</strong> & Müller Anästh Intensivmed 2003;44:214-6<br />
[1] Der erwartet schwierige Atemweg –<br />
immer <strong>fiberoptische</strong> Wachintubation?<br />
[2] Der unerwartet schwierige Atemweg –<br />
Empfehlungen und Algorithmen<br />
Suhl, 04.04.2009, Seite 5<br />
Tubuswechselkatheter - Optionen<br />
□ Temp. Trachealer Platzhalter<br />
□ Reintubation<br />
□ Umintubation *<br />
□Temporäre Oxygenation /<br />
(Ventilation) *<br />
* unter laryngoskopischer /<br />
manueller Zungengrundstützung !<br />
Nates & Berner. The Internet J of Anesthesiology 2001;5/1<br />
Mort TC. The Internet J of Anesthesiology 2001;5/4<br />
Mort TC. Anesth Analg 2007;105:1357-62<br />
[1] Der erwartet schwierige Atemweg –<br />
immer <strong>fiberoptische</strong> Wachintubation?<br />
Wenn indiziert / machbar → ja!<br />
Ansonsten nein, nein weil es Alternativen gibt!<br />
Menschliche und andere Fehlerquellen<br />
+ CPAP<br />
/ NIV<br />
Fehler:<br />
Bis 70% Fehler durch „menschliche Faktoren“…<br />
„Ich tat etwas Falsches“<br />
Verstoß: „Ich wußte es, aber ich wollte es nicht tun“<br />
□ Organisationsstrukturen und Verfahren<br />
□ Training in der Routine und von Notfallsituationen<br />
□ Organisiertes Lernen<br />
□ Formen der Zwischenfallsanalyse<br />
Rall M, <strong>Die</strong>ckmann P Safety culture and crisis resource management in airway management: General<br />
principles to enhance patient safety in critical airway situations.<br />
Best Pract & Res Clin Anaesthesiol 2005;19:539-57<br />
Manser T (Hrsg.) Komplexes Handeln in der Anästhesie, Pabst Science Publishers, Lengerich 2003<br />
5
R. <strong>Gottschall</strong>, <strong>Die</strong> <strong>fiberoptische</strong> <strong>Intubation</strong> +<br />
<strong>Sicherung</strong> <strong>des</strong> <strong>Atemweges</strong>,<br />
Atemwegssicherung: Hintergrund<br />
< 1% bis > 8.5% Häufigkeit <strong>des</strong> schwierigen <strong>Atemweges</strong>,<br />
bei Kopf - Hals - Tumoren bis 11% !<br />
Bis ~ 30% Anästhesie - bedingter Morbidität / Mortalität<br />
Bis ~ 30% nicht sicher bestimmbar<br />
→ Erfordernis institutioneller Konzepte<br />
(Ausbildungseinrichtung vs. Versorgungskrankenhaus)<br />
Präoxygenation (Erwachsene)<br />
□ Obligater Bestandteil <strong>des</strong> AWM, Dokumentation?<br />
□ Ziel: Auffüllen <strong>des</strong> verfügbaren (!) pulmonalen O2-Speichers (=FRC; ~ 35 ml/kg KM; O2-Verbrauch ~ 3ml/kg/min)<br />
□ Monitoring = FetO2 (≥ 80% anstreben…)<br />
□ Maske dicht (Kapnogramm?); ≥ 8l/min O2; Oberkörper 25-30°↑;<br />
CPAP (ca 6 cm WS) sinnvoll…<br />
□ „Verlängerung“ durch ass. / kontrollierte Maskenventilation, ggf.<br />
Larynxmaske (außer RSI), apnoische Oxygenation oder<br />
transtracheale Oxygenation<br />
Herriger A et al. Anaesthesia 2004;59.243-7<br />
Dixon BJ et al. Anesthesiology 2005;102:1110-5<br />
Gerlach K u. Mitarb. Anaesthesist 2006;41:93-118<br />
Äußere Kehlkopfmanöver<br />
n. Knill (BURP) bzw. Benumof (OELM)<br />
□ Häufiger Fehler = Verwechslung / Gleichsetzung mit Krikoiddruck !<br />
□ <strong>Die</strong>se Manöver dienen der Optimierung von direkter Laryngoskopie /<br />
Tubuspassage im Rahmen der endotrachealen <strong>Intubation</strong>, meist durch<br />
Manipulation am Schildknorpel (selten am Zungenbein oder Ringknorpel)<br />
Backward, Upward, Rightside & Pressure<br />
Optimal External Laryngeal Manipulation<br />
Suhl, 04.04.2009, Seite 6<br />
Kopf-Hals-Position und Atemwegsmanagement<br />
[Maskenventilation, Laryngoskopie, <strong>Intubation</strong>, supraglottische Luftbrücken]<br />
Schulter- „Rampe“<br />
„Schnüffelposition“ oder<br />
verbesserte JACKSON-Position<br />
HWS - Flexion<br />
+ HWS - Extension<br />
Optimierung der konventionellen <strong>Intubation</strong><br />
□ Lagerung („Schnüffelposition“)<br />
□ Präoxygenation<br />
□ Muskeltonus ↓; Antisalivation<br />
□ Maskenventilation; pharyngeale Schienung<br />
□ Lichtverhältnisse; Absaugung<br />
□ Externe Larynxmanöver (BURP, OELM)<br />
□ Krikoiddruck bei Indikation<br />
□ Tubus - Einführhilfen<br />
□ Typ- / Größenwechsel Spatel / Tubus<br />
□ Zweit - Intubateur (FA)<br />
modif. n. Benumof JL ASA Annual Meeting Refresher Course 2000<br />
Mandrins / Einführhilfen für ETT<br />
6
R. <strong>Gottschall</strong>, <strong>Die</strong> <strong>fiberoptische</strong> <strong>Intubation</strong> +<br />
<strong>Sicherung</strong> <strong>des</strong> <strong>Atemweges</strong>,<br />
www.smith-medical.com<br />
www.vbm-medical.de<br />
www.cookmedical.com<br />
Einführhilfen n. Muallem und Frova<br />
Portex („gum elastic bougie“, Eschmann - Stab)<br />
Muallem MK et al Middle East J Anesthesiol 2005;18:385-9<br />
Detave M et al. Ann Fr Anesth Reanim 2008;27:154-7<br />
Indikation: C & L III<br />
15 F<br />
12 / 14 F<br />
14 F<br />
Gerader Laryngoskopspatel n. Henderson<br />
Henderson JJ The use of paraglossal straight blade laryngoscopy in difficult tracheal intubation.<br />
Anaesthesia 1997;52:552-60<br />
„Keiner ist blinder als der,<br />
der nicht sehen will“<br />
Johnathan Swift 1667-1745<br />
Suhl, 04.04.2009, Seite 7<br />
Portex - Einführung für Trachealtuben<br />
(„gum elastic bougie“, Eschmann-Stab)<br />
www.AnaesthesiaUK.com<br />
Gerader Laryngoskopspatel n. Henderson<br />
□ Sichtverbesserung<br />
□ Relativ atraumatisch<br />
□ Optionen: variabler oraler Zugang<br />
± Einführhilfen<br />
□ 1. Alternative zur Macintosh - Technik<br />
Henderson JJ, Frerk CM Remember the straight laryngoscope.<br />
Br J Anaesth 2002;88:151-2<br />
Macht „um die Ecke schauen“ Sinn?<br />
□ Anpassung an die Anatomie (…macht immer Sinn)<br />
□ Anpassung an veränderte Anatomie ist schon schwieriger<br />
□ „Blinde“ Verfahren sollten der Vergangenheit angehören<br />
□ Optische Hilfsmittel sind medizinischer Standard<br />
□ Handhabung der flexiblen Fiberoptik ist komplex<br />
□ Der vergleichende Nutzen neuer Hilfsmittel ist zu belegen…<br />
Mihai R et al. A quantitative review and meta-analysis of performance of non-standard laryngoscopes and rigid<br />
fibreoptic intubation aids. Anaesthesia 2008;63:745-60<br />
7
R. <strong>Gottschall</strong>, <strong>Die</strong> <strong>fiberoptische</strong> <strong>Intubation</strong> +<br />
<strong>Sicherung</strong> <strong>des</strong> <strong>Atemweges</strong>,<br />
Video - Laryngoskope<br />
□ Primär methodische Ausbildung<br />
(Supervision, Lernkurve)<br />
□ Sekundär schwieriger Atemweg<br />
(↑Blickwinkel, Vergrößerung)<br />
( STORZ) (ACUTRONIC / IFM) (SATURN / SAEGELING)<br />
Kaplan MB et al. A new video laryngoscope – an aid to intubation and teaching. J Clin Anesth 2002;14:620-6<br />
Kaplan MB et al. Seeing is believing: the importance of video laryngoscopy in teaching and in the managing the<br />
difficult airway. Surg Endosc 2006;Suppl 2:S479-83<br />
Retromolares <strong>Intubation</strong>sfiberskop n. Bonfils<br />
40º 40°<br />
Rudolph & Schlender: Anaesthesiol Reanimat 1996;21:127-0<br />
Rudolph C et al Minerva Anestesiol 2007;73:567-74<br />
Alternative Laryngoskope / starre Optiken<br />
□ Unerwartet: Cormack & Lehane ≥ Grad 3 („can oxygenate“)<br />
□ Erwartet: - Alternative (Wach-)<strong>Intubation</strong><br />
- HWS - Probleme<br />
- Limitierte Mund - Kiefer - Öffnung<br />
- Kritischer (maxillärer) Zahnstatus<br />
□ Sonstige: - Habituelle Kieferluxation, Stimmberuf<br />
- Second look, Umintubation (TWK)<br />
- Training in Tagesroutine<br />
Suhl, 04.04.2009, Seite 8<br />
Video - Laryngoskope<br />
□ C & L - Scores besser<br />
□ Erfolgsrate (<strong>Intubation</strong>) höher<br />
□ Zeitaufwand (<strong>Intubation</strong>) geringer<br />
□ Erfordernis von Zusatzmanövern<br />
(z.B. BURP) geringer<br />
□ Spatelvarianten wünschenswert<br />
□ <strong>Intubation</strong>sbedingungen verbessert<br />
□ Empfehlung für schwieriges Atemwegsmanagement<br />
Stroumpoulis K et al. Videolaryngoscopy in the management of the difficult airway: a comparison with the<br />
Macintosh blade. Eur J Anaesthesiol 2009;26:218-22<br />
Jungbauer A et al. Expexted difficult tracheal intubation: a prospective comparison of direct laryngoscopy<br />
and video laryngoscopy in 200 patients. Br J Anaesth 2009;<br />
Airtraq ® : Optisches Einweg - Laryngoskop<br />
www.airtraq.com<br />
www.b-und-p.com<br />
Dhonneur G et al. Anesthesiology 2007;106:629-0<br />
Maharaj CH et al. Anaesthesia 2008;63:182-8<br />
Verifizierung der Tubuslage<br />
□ Kapnografie / Kapnometrie<br />
(≥ 4 kPa / 30 mm Hg)<br />
□ Direkte Laryngoskopie<br />
□ Flexible Endoskopie via Tubus<br />
Thompson & Jaffe Respir Care 2005;50:100-8<br />
Salem MR Anesthesiol Clin N Am 2001;19:813-39<br />
?<br />
8
R. <strong>Gottschall</strong>, <strong>Die</strong> <strong>fiberoptische</strong> <strong>Intubation</strong> +<br />
<strong>Sicherung</strong> <strong>des</strong> <strong>Atemweges</strong>,<br />
Algorithmus – Sinn oder Unsinn?<br />
□ Vorgabe zur Problemlösung<br />
□ Bestandteil von Leitlinien (= Freiwilligkeit)<br />
- Wissensvermittlung<br />
- Qualitätsverbesserung<br />
- Angemessenheit<br />
- Kosteneffizienz<br />
Pro: - Verhaltensregel / Trainingsoption für Notfall<br />
- Standardisierung / Handlungskorridor (für Ärzte!)<br />
- Verbesserung <strong>des</strong> Outcome / Schadensverhütung<br />
Con: - Praxisfremde „Kochbuchmedizin“ / keine Evidenz<br />
- Innovationseinschränkung / Überreglementierung<br />
- Ignoranz individueller Situationen<br />
- Ursache forensischer Konsequenzen<br />
Algorithmus – Beispiel Uni Kiel<br />
Dörges V, Bein B Atemwegsmanagement… AINS 2006;9:564-74<br />
modif. n. Georgi R, Stuttgart<br />
Anesthesiology 2003;98;1269-77<br />
Erster Algorithmus für die<br />
Bewältigung <strong>des</strong><br />
schwierigen <strong>Atemweges</strong><br />
Anesthesiologie 1993;78:597-602<br />
©Dr. R. <strong>Gottschall</strong> 01/2009<br />
Suhl, 04.04.2009, Seite 9<br />
Algorithmuskonzeption – Empfehlungen<br />
□ Handlungskorridor (für Ärzte!)<br />
□ Facharztqualität („best practice“- Prinzip)<br />
□ Präoxygenierung / Hilferuf<br />
□ Relaxation nur bei sicherer Maskenventilation (!?)<br />
□ Maximal zwei (!) <strong>Intubation</strong>sversuche<br />
□ Erhaltung von Rückzugsmöglichkeiten<br />
□ Keine Wiederholung einer Technik, die versagte…<br />
□ Situative Abweichung optional möglich<br />
□ Übersichtliche, kurz gefasste Gestaltung<br />
(→ max. 4 Entscheidungsebenen)<br />
□ Klientel, Hilfsmittel, Erfahrungsstand und Logistik<br />
vor Ort<br />
Algorithmus – „Zugang“ zum Luftweg<br />
Erwartet<br />
(Präparation!)<br />
Algorithmus Schwieriger Atemweg<br />
Evaluierung / Strategie<br />
Lagerung<br />
Präoxygenation<br />
LA / Regionalanästhesie + Plan B vs.<br />
Primäre Tracheotomie in LA vs.<br />
Wach-FOI vs. Maskeneinleitung (Sevo) vs.<br />
Alternative Ventilation / Laryngoskopie / <strong>Intubation</strong> Erschwerte<br />
Maskenventilation<br />
+<br />
-<br />
Hilferuf !<br />
Spontanatmung ?<br />
Eingriff fortführen /<br />
verschieben ?<br />
Sekundäre <strong>Intubation</strong><br />
(1 Versuch) vs. Aufwachen<br />
+<br />
-<br />
+<br />
Supraglottische Luftbrücke<br />
(2 Versuche)<br />
modif. n. Georgi R, Stuttgart<br />
Rosenblatt WH J Clin Anesth 2004;16:312-16<br />
+ „Notrohr“* -<br />
Sekundäre Tracheotomie<br />
-<br />
Unerwartet<br />
AA-Induktion*<br />
Erschwerte Laryngoskopie<br />
/ <strong>Intubation</strong> (2 Versuche)<br />
-<br />
„cicv“<br />
*HNO<br />
*Relaxation?<br />
Kompetenzentscheidung<br />
+<br />
Koniotomie<br />
englumig / weitlumig<br />
9
R. <strong>Gottschall</strong>, <strong>Die</strong> <strong>fiberoptische</strong> <strong>Intubation</strong> +<br />
<strong>Sicherung</strong> <strong>des</strong> <strong>Atemweges</strong>,<br />
Nasotracheale <strong>Intubation</strong> - nicht der Rede wert?<br />
Piepho T et al. Nasotracheal intubation: look before you leap.<br />
Br J Anaesth 2005;94:859-0<br />
Narkoseeinleitung<br />
Tubuseinführung nasal<br />
Laryngoskopie<br />
K o n i o t o m i e !<br />
Blutung aus Nasenrachen<br />
C & L Grad 4<br />
Nasotracheale <strong>Intubation</strong>stechnik<br />
3. Direkte Laryngoskopie (Zahnschutz)<br />
4. Nasale Einführung Absaugkatheter<br />
(im Tubus)<br />
5. Laryngeale Einführung Absaugkatheter<br />
(Magill-Zange)<br />
Nasotracheale <strong>Intubation</strong>stechnik<br />
6. (2 ml Xylocain-Gel nasal vor) <strong>Intubation</strong><br />
7. Polsterung / Tubusfixation nach<br />
Lagekontrolle, „Gänsehals“<br />
8. Augensalbe, -pflaster<br />
9. <strong>Intubation</strong>skissen entfernen<br />
Suhl, 04.04.2009, Seite 10<br />
Nasotracheale <strong>Intubation</strong>stechnik<br />
1. Abschwellen der Nasenschleimhaut<br />
→ 1ml Lidocain 3% + Phenylephrin<br />
0,25% mittels Nasalzerstäuber (MAD)<br />
2. Narkoseeinleitung<br />
Nasotracheale <strong>Intubation</strong>stechnik<br />
Weshalb macht ein Absaugkatheter (14 F) im Tubus Sinn ?<br />
□ Freie Nasen - Rachen - Passage erkennbar<br />
□ Tubus - Lumen geschützt<br />
□ Tubus - Cuff geschützt (Magill - Zange)<br />
□ Tubuspassage (meist) erleichtert<br />
□ Sofortige Absaugung möglich<br />
□ Verbesserte Patientensicherheit !<br />
Komplikationen beim Atemwegsmanagement<br />
□ Kardiovaskulär (Arrhythmie, Hypertonie, Myokardischämie, …)<br />
□ Respiratorisch (Hypoxie, Hyperkarbie, Laryngo,- bronchospasmus)<br />
□ ZNS (ICP↑; neuroaxiale Läsionen)<br />
□ Augen (IOP↑; Druckschäden)<br />
□ Kiefergelenke, HWS, atlanto - occipitaler Übergang<br />
□ Strukturelle Läsionen (Zahnschäden, Weichteiltrauma)<br />
□ Fehlintubation (ösophageal)<br />
□ Verschiedenes (Pharmakol. NW, Latexallergie, Barotrauma)<br />
□ Schmerzen, Hospitalisierung, Kosten, soziale / berufliche Folgen…<br />
Hagberg C et al. Complications of managing the airway. Best Pract Res Clin Anaesthesiol 2005;19:641-59<br />
10
R. <strong>Gottschall</strong>, <strong>Die</strong> <strong>fiberoptische</strong> <strong>Intubation</strong> +<br />
<strong>Sicherung</strong> <strong>des</strong> <strong>Atemweges</strong>,<br />
Algorithmus – Stellenwert der Larynxmaske<br />
Benumof JL Anesthesiology 1996;84:686-99<br />
Bilder: Prof. S. Kapral, Wien<br />
Higgs A et al. Anaesthesia 2005;60:915-20<br />
Cook TM et al. Anaesthesia 2005;60:1129-36<br />
Zura A et al. Anesth Analg 2006;103:785<br />
Aintree - Katheter<br />
Sek. <strong>Intubation</strong> nach „bridging“<br />
mit supraglottischen<br />
Luftbrücken / (ETT-Wechsel)<br />
unter <strong>fiberoptische</strong>r Sicht…<br />
„Can´t intubate - can´t ventilate“<br />
Gesichtsmasken - Ventilation<br />
0 ∞<br />
einfach unmöglich<br />
1. 2. 3.<br />
C&L IIIº C&L IVº<br />
Laryngoskopie / Fehlintubation<br />
modif. n. Janssens & Hartenstein Eur J Anaesthesiol 2001;18:3-12<br />
Mort TC Anesth Analg 2004;99:607-13<br />
Läsion<br />
Hypoxie<br />
Tod<br />
Suhl, 04.04.2009, Seite 11<br />
Aintree - Katheter<br />
Länge: 56 cm<br />
AD: 19F (5,75 mm)<br />
ID: 4,7 mm<br />
ETT: ≥ 6,5 mm ID<br />
FFO: ≤ 4.5 mm AD<br />
Atherton DP et al. A ventilation-exchange bougie for fibreoptic intubations with laryngeal mask airway.<br />
Anaesthesia 1996;51:123-6<br />
Laryngoskopie - Score n. Cormack & Lehane<br />
I Stimmlippen komplett einsehbar<br />
II (b/a) Aryknorpel / hintere Stimmlippenregion sichtbar<br />
III nur Epiglottis sichtbar<br />
IV Strukturen I-III nicht sichtbar<br />
0.3 – 20%<br />
I II III IV<br />
Cormack RS, Lehane J Anaesthesia 1984;39:1105-11; Williams KN et al. Br J Anaesth 1991;66:38-44<br />
Komplikationsrate wiederholter Laryngoskopieversuche<br />
n = 2833 (notfallmäßige <strong>Intubation</strong>en kritisch Kranker)<br />
≤ 2 Versuche<br />
Hypoxämie 11.8 %<br />
Regurgitation 1.9 %<br />
Aspiration 0.8 %<br />
Bradykardie 1.6 %<br />
Asystolie 0.7 %<br />
> 2 Versuche<br />
vs. 70 %<br />
vs. 22 %<br />
vs. 13 %<br />
vs. 21 %<br />
vs. 11 %<br />
Mort TC<br />
Emergency tracheal intubation: complications associated with repeated laryngoscopic attempts.<br />
Anesth Analg 2004:99:607-13<br />
11
R. <strong>Gottschall</strong>, <strong>Die</strong> <strong>fiberoptische</strong> <strong>Intubation</strong> +<br />
<strong>Sicherung</strong> <strong>des</strong> <strong>Atemweges</strong>,<br />
Welche Situationen sind zu unterscheiden ?<br />
□ „Can´t ventilate – can intubate“ → 1 <strong>Intubation</strong>sversuch sinnvoll<br />
□ „Can ventilate – can´t intubate“<br />
→ Kompetenzentscheidung über Priorität von Oxygenation,<br />
Rückzugsstrategie vs. sekundäre <strong>Intubation</strong><br />
□ „Can´t intubate / can´t see anything – can´t ventilate“<br />
→ häufig Folge inadäquaten Atemwegsmanagements,<br />
Notfallmaßnahmen zwingend !<br />
□ “Can’t perform cricothyrotomy<br />
Surgery (or trauma)<br />
Hematoma (or abscess)<br />
Obesity (or access problem)<br />
Radiation distortion (or deformity)<br />
Tumor<br />
Neues zur Maskenventilation<br />
PCV<br />
Druck: 13 cm WS<br />
PEEP: 3 cm WS<br />
Frequenz: variabel<br />
→ Spitzendruck < 20 cm WS<br />
von Goedecke A et al. Mechanical versus manual ventilation via face mask during the induction of<br />
Anesthesia: a prospective randomized, crossover study. Anesth Analg 2004;98:260-3<br />
von Goedecke A u. Mitarb. Maskenbeatmung als Rückzugsstrategie zur endotrachealen <strong>Intubation</strong>.<br />
Anaesthesist 2006;55:70-9<br />
Koniotomie - Verfahren: englumig<br />
n. Ravussin n. Enk<br />
(VBM) (COOK)<br />
Ravussin & Freeman Can Anaesth Soc J 1985;32:60-4<br />
Enk D Anästh Intensivbeh 2002;4:5-7<br />
Scrase & Woolard Anaesthesia 2006;61:962-74<br />
70º<br />
Erfolg<br />
- Priorität ?<br />
Suhl, 04.04.2009, Seite 12<br />
„Can‘t intubate - can‘t ventilate“<br />
Erfolg<br />
- Priorität ?<br />
Erfolg<br />
- sek. Tracheotomie<br />
- 100% O 2 , Krikoiddruck<br />
- Hilferuf + Equipment<br />
- oro-, nasopharyngeale Luftbrücken<br />
- Zwei-Personen-Maskenventilation<br />
Misserfolg*<br />
- Supraglottische Luftbrücke (LM, LT, CT, ET)<br />
Misserfolg*<br />
- TTO (Katheter, englumig) vs.<br />
- Koniotomie (weitlumig)<br />
Misserfolg → Hypoxie vs. †<br />
* Situationsmanagement / Kompetenzentscheid<br />
Transtracheale Oxygenation (TTO)<br />
□ Postoperativ<br />
□ Posttraumatisch<br />
□ Infektion<br />
□ Neoplasie<br />
Jacoby et al. JAMA 1956;162:625-8<br />
□ Präventiv<br />
McLellan et al. Can J Anaesth 1988;35:404-5<br />
Gerig HJ et al. Anaesthesia 2005;60:801-5<br />
Gulleth & Spiro Arch Otolaryngol Head Neck Surg 2005;131:886-90<br />
□ „Angioödem“<br />
□ Gendefekt<br />
□ Fremdkörper<br />
□ Cicv - Szenario<br />
Transtracheale Oxygenation (TTO)<br />
□ Katheter - Punktion (englumig)<br />
-Bei inkompletter Atemwegsobstruktion<br />
- Geringster Zeitaufwand<br />
- Geringste Invasivität<br />
- Wachapplikation in LA möglich<br />
- Diverse Sets vorhanden (z.B. COOK / VBM)<br />
- Kombination mit <strong>Intubation</strong>sverfahren<br />
- Tracheotomie im Einzelfall vermeidbar<br />
Schwarzkopf u. Mitarb.: Anaesthesist 2001;50:933-336<br />
Kunitz u. Mitarb.: AINS 2002;37:697-700<br />
Craven & Vanner: Anaesthesia 2004;59:95-599<br />
12
R. <strong>Gottschall</strong>, <strong>Die</strong> <strong>fiberoptische</strong> <strong>Intubation</strong> +<br />
<strong>Sicherung</strong> <strong>des</strong> <strong>Atemweges</strong>,<br />
Koniotomie - Verfahren: weitlumig<br />
□ Chirurgische Koniotomie<br />
□ Punktions-Koniotomie<br />
□ Dilatations-Koniotomie<br />
→ bei kompletter oberer<br />
Atemwegsobstruktion zwingend !<br />
Breitmeier u. Mitarb. AINS 2004;39:94-100<br />
Melker & Gabrielli Ann Otol Rhinol Laryngol 2005;114:525-8<br />
Byhahn & Meininger AINS 2006;9:576-84<br />
www.vbm-medical.de<br />
www.cookmedical.com<br />
Chirurgische Koniotomie (rapid four - step cricothyrotomy)<br />
1. Tasten<br />
2. Längsinzision (Haut) / Querinzision (Ligament)<br />
3. Zug + Spreizung 4. <strong>Intubation</strong><br />
Schwieriger Atemweg …und danach ?<br />
□ Klinische Visite(n); ggf. HNO-Konsil<br />
□ Dokumentation A - Protokoll<br />
□ Anästhesie - Ausweis (+ Kopie Krankenakte !)<br />
□ Information Patient (Folgetag)<br />
□ Schriftlicher Sachverhalt (→ Patient) ?<br />
□ Interne Aufarbeitung, ggf. externe Aufarbeitung<br />
PaSOS Website: http://www.pasos-ains.de<br />
Airway Management. Leitlinie der DGAI. A&I 2004;45:302-306<br />
Rall M u. Mitrarb. AINS 2008:43:628-32<br />
Suhl, 04.04.2009, Seite 13<br />
Koniotomie - Verfahren: weitlumig<br />
→ bei kompletter oberer<br />
Atemwegsobstruktion zwingend !<br />
□ Kombi - Set:<br />
Chirurgische Koniotomie + Dilatations - Koniotomie<br />
SURGICAL SELDINGER www.cookmedical.com<br />
Koniotomie - Verfahren: weitlumig<br />
→ bei kompletter oberer<br />
Atemwegsobstruktion zwingend !<br />
□ Kombi - Set:<br />
Chirurgische Koniotomie + Dilatations - Koniotomie<br />
SURGICAL SELDINGER www.cookmedical.com<br />
13
R. <strong>Gottschall</strong>, <strong>Die</strong> <strong>fiberoptische</strong> <strong>Intubation</strong> +<br />
<strong>Sicherung</strong> <strong>des</strong> <strong>Atemweges</strong>,<br />
Atemwegsmanagement - Medikolegale Aspekte<br />
Leitlinien = Orientierung, kein Standard !<br />
→ individuelle Sorgfalt wesentlicher<br />
Kuwatsch S<br />
Haftungsrechtliche Bedeutung von Leitlinien ärztlicher Fachgesellschaften<br />
Anaesthesist 2008;57:1103-4<br />
Leitlinien (ASA, DGAI) werden<br />
gutachterlich einbezogen…<br />
Breitmeier D u. Mitarb.<br />
Rechtsmedizinische Begutachtung von Behandlungsfehlervorwürfen zu<br />
To<strong>des</strong>fällen nach schwieriger <strong>Intubation</strong><br />
Rechtsmedizin 2005;15:363-70<br />
Fazit<br />
□ Primum nihil nocere !<br />
□ Selbstschutz<br />
□ Information<br />
□ Kommunikation<br />
□ Leitlinien<br />
□ Eigenes Konzept → Akzeptanz!<br />
□ Equipment<br />
□ Training<br />
□ Assistenz<br />
□ Analyse<br />
Suhl, 04.04.2009, Seite 14<br />
Welches Equipment?<br />
□ Alternatives Laryngoskop / starre Fiberoptik<br />
■ Gerader Laryngoskopspatel<br />
■ Anatomisch vorgeformtes Instrument<br />
□ Alternative Einführungshilfe für ETT<br />
□ Supraglottische Luftbrücken<br />
□ Flexible Fiberoptiken<br />
□ Aintree ® - Katheter<br />
□ Tubuswechselkatheter<br />
□ Koniotomie - Sets (eng- und weitlumig)<br />
„Airway-Tag“ - KAI SRH Zentralklinikum Suhl gGmbH, 04. April 2009<br />
Winterling [Eranthis hyemalis]<br />
19.03.2006 Rautal / Jena-Closewitz<br />
Danke für Ihr<br />
Interesse !<br />
reiner.gottschall@med.uni-jena.de<br />
14