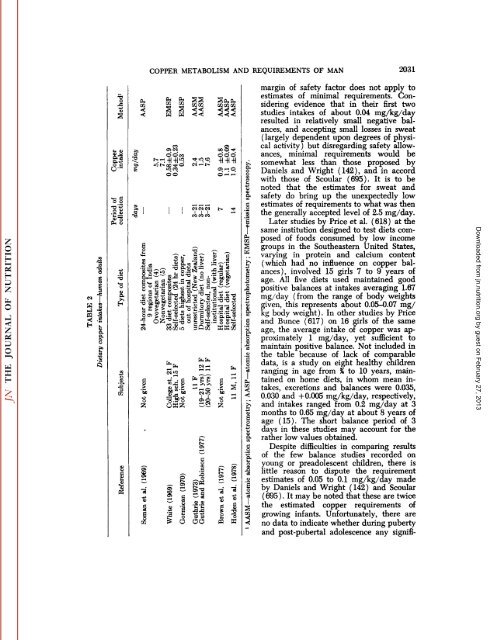
2Ü30 KARL E. MASON (394) after experiences in compensating for a <strong>copper</strong> deficiency state developing in an infant with ileal atresia <strong>and</strong> short bowel syndrome maintained on total parenteral nutrition for the first 6.75 months <strong>of</strong> life. In current practice for complete intrave nous feeding <strong>of</strong> premature infants <strong>of</strong> less than 1,050 g birth weight, James <strong>and</strong> Mac- Mahon (383) provide 50 ¿u.g/kg/day <strong>of</strong> <strong>copper</strong>. Quite in accord with these opinions are those <strong>of</strong> Ashkenazi et al. (25), record ing <strong>copper</strong> deficiency in a premature infant 6 months old fed a diet <strong>of</strong> only whole milk <strong>and</strong> 5% cane sugar, <strong>and</strong> in a premature infant subjected to bowel surgery <strong>and</strong> maintained on parenteral feeding for 3 months. Both responded rapidly to oral <strong>copper</strong>, <strong>and</strong> investigators recommended that small premature infants be given sup plements <strong>of</strong> 0.1 to 0.5 mg <strong>of</strong> <strong>copper</strong> daily while milk is their only food, or during pro longed intravenous feeding. On the basis <strong>of</strong> the evidence cited above, it seems reasonable to assume that the daily requirement <strong>of</strong> intravenous <strong>copper</strong> for infants, beyond the age at which they can depend upon prenatal tissue reserves ( about 2 months ), may be in the range <strong>of</strong> 0.1 to 0.2 mg/day. On the assumption that approximately 40^ <strong>of</strong> orally ingested cop per is absorbed, this requirement would be the equivalent <strong>of</strong> 0.25 to 0.5 mg/day <strong>of</strong> oral <strong>copper</strong>. For a 10-kg infant this would represent 0.025 to 0.05 mg/kg/day. Thus, the information provided by parenteral nutrition is in general concordance with that from studies in milk intake, <strong>copper</strong> balance <strong>and</strong> recovery from deficiency states, which indicate <strong>requirements</strong> <strong>of</strong> about 0.025 to 0.05 mg/kg/day for healthy full-term infants during early years <strong>of</strong> life, with somewhat more generous allowances for premature <strong>and</strong> low-birth-rate infants. Young children <strong>and</strong> adolescents The basis for determining the minimal daily <strong>requirements</strong> <strong>of</strong> <strong>copper</strong> for young children <strong>and</strong> adolescents is decidedly lim ited, as is indicated in table 1. Two pioneer studies on 3- to 6-year old children (142, 695), although carried out 40 or more years ago, warrant special consideration. Daniels <strong>and</strong> Wright ( 142) studied five boys <strong>and</strong> three girls <strong>and</strong> employed two diets, one high in meat <strong>and</strong> cereals <strong>and</strong> the other high in cereals without meat, but similar in <strong>copper</strong> content. After 3 days <strong>of</strong> adjustment to the diet, 5-day balance studies were made. Mean <strong>copper</strong> intakes, fecal plus urinary excretions <strong>and</strong> balances were, respectively, 1.48, 1.03 <strong>and</strong> +0.45 mg/day. It was concluded that diets for children <strong>of</strong> pre-school age should include not less than 0.10 mg/kg/day <strong>of</strong> <strong>copper</strong>. Scoular (695) carried out similar balance studies on three boys <strong>of</strong> the same age, based upon three different but well con trolled diets. On the average, <strong>copper</strong> in takes, fecal <strong>and</strong> urinary losses <strong>and</strong> reten tions were, respectively, 1.36, 0.60, <strong>and</strong> +0.76 mg/kg/day. In their best judgment, the minimal requirement <strong>of</strong> boys <strong>of</strong> that age would be between 0.053 <strong>and</strong> 0.085 mg/kg/day. Similar conclusions were reached by Macy (477) in balance studies on school children 8 <strong>and</strong> 11 years <strong>of</strong> age. It may be noted that both <strong>of</strong> these esti mates fall within the range <strong>of</strong> estimated <strong>copper</strong> <strong>requirements</strong> for infants (0.05-0.1 mg/kg/day) as discussed above. Balance studies carried out by Engel et al. (190) on groups <strong>of</strong> 12 girls 6 to 10 years <strong>of</strong> age, during summer months <strong>of</strong> 1956, 1958 <strong>and</strong> 1962, employing liberal pro tein, low animal protein <strong>and</strong> vegetarian type diets, leave open questions concern ing <strong>requirements</strong>. Calculations made (by writer) from the data given indicate that the first two <strong>of</strong> these diets provided aver age <strong>copper</strong> intakes <strong>of</strong> 0.04 <strong>and</strong> 0.037 mg/ kg/day <strong>and</strong> <strong>copper</strong> balances <strong>of</strong> —0.01<strong>and</strong> —0.08mg/day, respectively. Comparable values for the vegetarian diet were 0.12 mg/kg/day <strong>and</strong> +1.02 mg/day. These data would suggest a minimal intake somewhat less than proposed in the two studies just described. However, Engel et al. ( 190) estimated, by regression analysis, that the daily intake in their studies was 1.3 mg/ day, <strong>and</strong> that the suggested allowance be 2.5 mg/day. In this suggestion was in cluded a sweat loss <strong>of</strong> 0.5 mg/day <strong>and</strong> a safety margin <strong>of</strong> 0.7 mg/day, added to the 1.3 mg/day intake. For matters <strong>of</strong> com parison, sweat loss was not incorporated in other balance studies recorded, <strong>and</strong> the estimated loss appears to be more than generous for the subjects. Furthermore, the Downloaded from jn.nutrition.org by guest on February 27, 2013
s &5°.S0 0lì»"oPH o^—•3'S tT"* i•«OaM d."io i«^-v-— * ^3 |W 8tJ -gPQ S< •§H ».WI.111*^ | ÈS15":»1 1Jjfe COPPER METABOLISM AND REQUIREMENTS OF MAN 2031 £S3 * ss< Weo» W «".^.§ 00«g mW00s, •8 'e° 1 ~.co ^ca*"1 p ^.Ã2- , ^" u —° e *'ß c l.0"!'^Sili M'S'S -si"ìr^!i?^o s'S "*^~ 35 S o-Sá? "Si ^S >*j^"O*JL'2s COC^iO^feB ='a §>"'&!z ^«"JZ UÅ’Z•I2 g— 'S ' ' »rt to•a as c«IJJte «t£ **-•suaifefefe^"èr-H u «JL'"ffiffiSfeC C£M ^^NS2¿^ ^ï •,^^t^~O×eL5 ^v o«tà ||O 0)•C'C"S o' o -H-H-HO3-H Oo' --ÃŒt~ -i •*'—• ^^V C.>^.S5X! «aCJa a1"ca^T^|il|"-- gì -2.t- * ^S's ^-1 ^- u ¿ o3^it^03 ^d • C • S "^> 3~'& '"g ^"H"3 "*« 'S« *î 1£ "o P3 K£ 3OÜ¡II«•