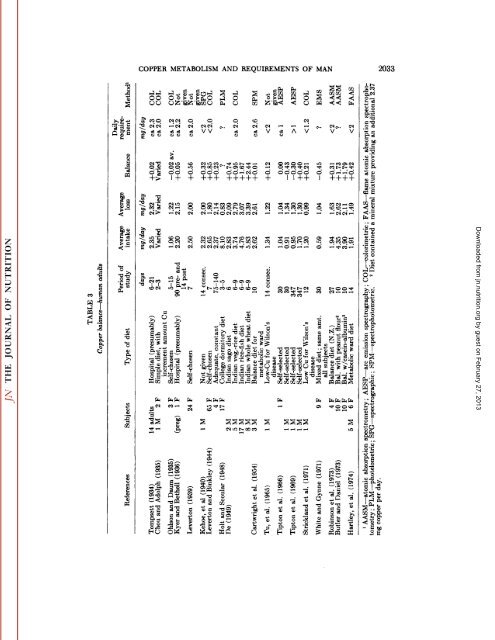
2032 KARL E. MASON cant changes in <strong>copper</strong> <strong>requirements</strong> occur. Considering the rather bizarre food intakes <strong>and</strong> eating habits <strong>of</strong> this segment <strong>of</strong> popu lations, there is real need for <strong>copper</strong> bal ance studies on pre-college teenagers. Except for the inconclusive observations <strong>of</strong> Dawson et al. ( 152 ), no consideration has been given to the special nutritional re quirements, including those <strong>of</strong> <strong>copper</strong>, in teen-age pregnancies. Considering that in such situations there is need to meet growth <strong>requirements</strong> <strong>of</strong> the adolescent mother as well as those <strong>of</strong> the developing fetus, it may be assumed that <strong>requirements</strong> are appreciably greater than in adult preg nant women. Adults Since adults are past the growing phase <strong>of</strong> life, <strong>copper</strong> <strong>requirements</strong> are expressed in terms <strong>of</strong> mg/day rather than as mg/kg/ day, as in the case <strong>of</strong> infants <strong>and</strong> adoles cents. Dietary intake. An earlier section (pp. 1998-1999) deals with the wide variation in <strong>copper</strong> content <strong>of</strong> human diets in various countries <strong>and</strong> <strong>of</strong> individuals <strong>of</strong> different ages. Table 2 summarizes additional data from studies in which the daily dietary intake <strong>of</strong> <strong>copper</strong> (<strong>of</strong>ten as only one <strong>of</strong> many trace elements), exclusive <strong>of</strong> <strong>copper</strong> balance, was <strong>of</strong> primary concern. Indian diets, which are predominately vegetarian in composition, are notably high in <strong>copper</strong> content. Analyses <strong>of</strong> diets <strong>of</strong> ovovegetarian <strong>and</strong> nonvegetarian populations in India by Soman (727) indicate, by writers's calcu lation from the data given, intakes <strong>of</strong> about 5.7 <strong>and</strong> 7.1 mg/day, respectively. An ex ceptionally high content <strong>of</strong> <strong>copper</strong> in Indian diets is also reported by De ( 154) as shown in table 3. These values are con siderably in excess <strong>of</strong> those reported from other countries. Only in the studies <strong>of</strong> Guthrie (289, 291) is mention made <strong>of</strong> the influence <strong>of</strong> liver, well known to be much higher in <strong>copper</strong> than other food constitu ents. In other studies in which composi tion <strong>of</strong> the diet employed is given, liver has not been listed as an ingredient. Somewhat surprising are the low <strong>copper</strong> levels found in student diets (White), hospital diets (Gormican; Brown et al.) <strong>and</strong> self-selected diets (Holden et al.). The values reported are appreciably lower than those for com parable types <strong>of</strong> diets in the balance studies recorded in table 3. The studies summarized in table 2 merely give some picture <strong>of</strong> variations in the <strong>copper</strong> intake <strong>of</strong> small groups <strong>of</strong> individuals in several dif ferent countries. They provide no valid in formation concerning <strong>requirements</strong> for <strong>copper</strong>, since there is no evidence <strong>of</strong> their ability to maintain positive balance over long periods <strong>of</strong> time. To a certain extent the same may be said <strong>of</strong> traditional balance studies such as recorded in table 3, but the latter do provide data on <strong>copper</strong> re tention, in terms <strong>of</strong> intake less fecal excre tion. While they provide data over only a limited period <strong>of</strong> days or weeks, they do represent a measure <strong>of</strong> daily <strong>requirements</strong> somewhat equivalent to that provided by total parenteral nutrition. Balance studies. Table 3 summarizes, in chronological sequence, data pertaining to balance studies on human adults. In 6 <strong>of</strong> the first 10 studies, extending from 1934 to 1954, the estimated requirement ranges from 2.0 to 2.6 mg/day. These data pro vided the basis for the wide acceptance <strong>of</strong> 2.0 or 2.0 to 2.5 mg as the daily require ment <strong>of</strong> <strong>copper</strong> for adult man. However, Cartwright <strong>and</strong> Wintrobe (106) later state that at lower levels <strong>of</strong> intake adjustments may be made to reduce <strong>copper</strong> excretion such that the daily requirement would be less than 2 mg <strong>and</strong> might even be negli gible. Presumably, a major factor in this adjustment would be a call upon <strong>copper</strong> stores in the liver <strong>and</strong> other organs. The levels <strong>of</strong> <strong>copper</strong> intake reported by Holt <strong>and</strong> Scoular (349) are truly excessive <strong>and</strong> the investigators, noting the much lower values recorded by Leverton <strong>and</strong> Binkley (452) for college students fed similar diets, somewhat naively attribute this difference to "a regional effect upon the composition <strong>of</strong> food." Considering also the unreasonably low fecal <strong>and</strong> urinary loss <strong>and</strong> high retention values (calculated from tabular data reported but not com mented upon in the report) the atypical results recorded suggest unknown defects in methodology. The somewhat high cop per content <strong>of</strong> Indian diets <strong>of</strong> De ( 154) is in accord with the observations <strong>of</strong> Soman (727), table 1. Whether the predominantly Downloaded from jn.nutrition.org by guest on February 27, 2013
î1co 1stW »a«a3 COPPER METABOLISM AND REQUIREMENTS OF MAN 2033 „" -g^ CO>• co'ig "OC«*--H ^I5 2>B•S C^12 t 7?ow^^îs-cS. i^^1-3y.gìY Et»fe s QJO ni O Cu ®MCßO £Ci PU O C» ci•9VSogC4O IOIMICihO1feT(M8?2!1 i-*O JgoJ NVV11«~.£cc|sUfieu *T3•S -wr- -^ c's• C—>% . .— 0) ^ O"or -Q-^- V î"S„^ O ^ *fe tÃ-t-s aizo"oUZ