The need for a lower total PSA cut-off value with PSA assays ...
The need for a lower total PSA cut-off value with PSA assays ...
The need for a lower total PSA cut-off value with PSA assays ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>The</strong> <strong>need</strong> <strong>for</strong> a <strong>lower</strong> <strong>total</strong> <strong>PSA</strong> <strong>cut</strong>-<strong>off</strong> <strong>value</strong> <strong>with</strong><br />
<strong>PSA</strong> <strong>assays</strong> calibrated to the new WHO standard<br />
<strong>The</strong> recalibration of <strong>PSA</strong> <strong>assays</strong> to the new World Health Organisation WHO 96/670 standard<br />
has certainly led to improved harmonisation of testing, but it has not yet resulted in the complete<br />
con<strong>for</strong>mity expected by many clinicians and laboratory managers. <strong>The</strong>re is also an urgent <strong>need</strong><br />
<strong>for</strong> manufacturers to redefine a valid clinical decision limit after <strong>PSA</strong> assay recalibration to WHO<br />
standard, in order to maintain a similar clinical per<strong>for</strong>mance of the measurement. <strong>The</strong> consequence<br />
of not providing a new <strong>cut</strong>-<strong>off</strong> <strong>value</strong> is that a higher number of <strong>PSA</strong> results may be interpreted as<br />
negative in the presence of prostate cancer.<br />
by Dr V. Jarrige<br />
Prostate cancer is the second leading cause of cancer<br />
death in men, exceeded only by lung cancer. It is the<br />
most common <strong>for</strong>m of malignancy in Europeans,<br />
<strong>with</strong> its incidence increasing more than <strong>with</strong> any<br />
other cancer over the last 20 years. According to WHO,<br />
about 190,000 new cases occur each year. Prostatespecific<br />
antigen (<strong>PSA</strong>) is the serum biomarker most<br />
widely used <strong>for</strong> early detection of prostate cancer and<br />
monitoring of patients <strong>with</strong> the disease. As men age,<br />
<strong>PSA</strong> levels generally rise. <strong>The</strong> most frequent reasons<br />
<strong>for</strong> elevated serum <strong>PSA</strong> <strong>value</strong>s are benign prostatic<br />
hyperplasia (BPH) or prostate cancer. Measurements<br />
of <strong>total</strong> <strong>PSA</strong> allow detection of cancer as early as five<br />
years be<strong>for</strong>e symptoms appear [1].<br />
Clinicians have always been aware that <strong>PSA</strong> <strong>assays</strong><br />
may differ significantly from one manufacturer to<br />
another; the drive towards recalibration was designed<br />
to address this issue. However, recalibration alone has<br />
no impact on the improvement in the clinical interpretation<br />
of results and may have led to the erroneous<br />
assumption that all <strong>assays</strong> are now the same.<br />
More European countries now request laboratories to<br />
use <strong>PSA</strong> <strong>assays</strong> that are calibrated to the WHO 96/670<br />
standard. However, this standard is not the one that<br />
was used to establish the clinically relevant <strong>PSA</strong> <strong>cut</strong>-<strong>off</strong><br />
<strong>value</strong> of 4.0 ng/mL. (This was defined using the original<br />
Hybritech Tandem-R <strong>PSA</strong> calibration system).<br />
Despite this, the <strong>cut</strong>-<strong>off</strong> <strong>value</strong> of 4.0 ng/mL is still<br />
used <strong>with</strong> the WHO-standardised assay from many<br />
manufacturers. Different results can still be produced<br />
by different <strong>PSA</strong> <strong>assays</strong> even if they are standardised<br />
to the same WHO standard; this is because variations<br />
in assay architecture and antibody choice prevent full<br />
achievement of standardisation. <strong>The</strong> use of the WHO<br />
standard thus only improves harmonisation between<br />
<strong>assays</strong> [2]. <strong>The</strong> use of the 4.0 ng/mL <strong>cut</strong>-<strong>off</strong> <strong>with</strong> results<br />
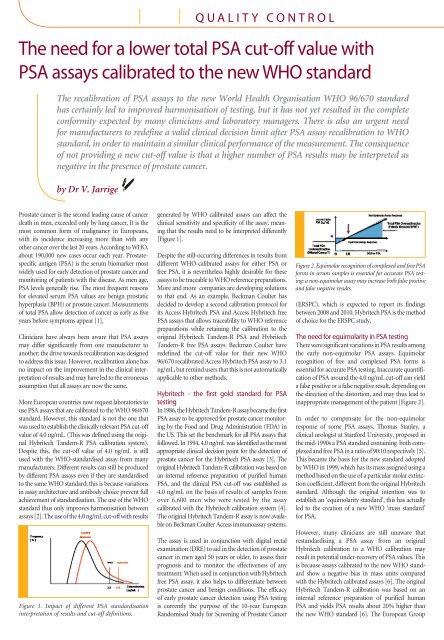
Figure 1. Impact of different <strong>PSA</strong> standardisation<br />
interpretation of results and <strong>cut</strong>-<strong>off</strong> definitions.<br />
Q u A l i T y c O n T r O l<br />
generated by WHO calibrated <strong>assays</strong> can affect the<br />
clinical sensitivity and specificity of the assay, meaning<br />
that the results <strong>need</strong> to be interpreted differently<br />
[Figure 1].<br />
Despite the still-occurring differences in results from<br />
different WHO-calibrated <strong>assays</strong> <strong>for</strong> either <strong>PSA</strong> or<br />
free <strong>PSA</strong>, it is nevertheless highly desirable <strong>for</strong> these<br />
<strong>assays</strong> to be traceable to WHO reference preparations.<br />
More and more companies are developing solutions<br />
to that end. As an example, Beckman Coulter has<br />
decided to develop a second calibration protocol <strong>for</strong><br />
its Access Hybritech <strong>PSA</strong> and Access Hybritech free<br />
<strong>PSA</strong> <strong>assays</strong> that allows traceability to WHO reference<br />
preparations while retaining the calibration to the<br />
original Hybritech Tandem-R <strong>PSA</strong> and Hybritech<br />
Tandem-R free <strong>PSA</strong> <strong>assays</strong>. Beckman Coulter have<br />
redefined the <strong>cut</strong>-<strong>off</strong> <strong>value</strong> <strong>for</strong> their new WHO<br />
96/670 recalibrated Access Hybritech <strong>PSA</strong> assay to 3.1<br />
ng/mL, but remind users that this is not automatically<br />
applicable to other methods.<br />
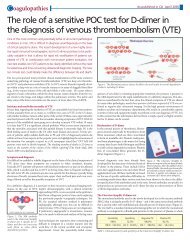
Hybritech - the first gold standard <strong>for</strong> <strong>PSA</strong><br />
testing<br />
In 1986, the Hybritech Tandem-R assay became the first<br />
<strong>PSA</strong> assay to be approved <strong>for</strong> prostate cancer monitoring<br />
by the Food and Drug Administration (FDA) in<br />
the US. This set the benchmark <strong>for</strong> all <strong>PSA</strong> <strong>assays</strong> that<br />
followed. In 1994, 4.0 ng/mL was identified as the most<br />
appropriate clinical decision point <strong>for</strong> the detection of<br />
prostate cancer <strong>for</strong> the Hybritech <strong>PSA</strong> assay [3]. <strong>The</strong><br />
original Hybritech Tandem-R calibration was based on<br />
an internal reference preparation of purified human<br />
<strong>PSA</strong>, and the clinical <strong>PSA</strong> <strong>cut</strong>-<strong>off</strong> was established as<br />
4.0 ng/mL on the basis of results of samples from<br />
over 6,600 men who were tested by the assay<br />
calibrated <strong>with</strong> the Hybritech calibration system [4].<br />
<strong>The</strong> original Hybritech Tandem-R assay is now available<br />
on Beckman Coulter Access immunoassay systems.<br />
<strong>The</strong> assay is used in conjunction <strong>with</strong> digital rectal<br />
examination (DRE) to aid in the detection of prostate<br />
cancer in men aged 50 years or older, to assess their<br />
prognosis and to monitor the effectiveness of any<br />
treatment. When used in conjunction <strong>with</strong> Hybritech<br />
free <strong>PSA</strong> assay, it also helps to differentiate between<br />
prostate cancer and benign conditions. <strong>The</strong> efficacy<br />
of early prostate cancer detection using <strong>PSA</strong> testing<br />
is currently the purpose of the 10-year European<br />
Randomised Study <strong>for</strong> Screening of Prostate Cancer<br />
Figure 2. Equimolar recognition of complexed and free <strong>PSA</strong><br />
<strong>for</strong>ms in serum samples is essential <strong>for</strong> accurate <strong>PSA</strong> testing:<br />
a non-equimolar assay may increase both false positive<br />
and false negative results.<br />
(ERSPC), which is expected to report its findings<br />
between 2008 and 2010. Hybritech <strong>PSA</strong> is the method<br />
of choice <strong>for</strong> the ERSPC study.<br />
<strong>The</strong> <strong>need</strong> <strong>for</strong> equimolarity in <strong>PSA</strong> testing<br />
<strong>The</strong>re were significant variations in <strong>PSA</strong> results among<br />
the early non-equimolar <strong>PSA</strong> <strong>assays</strong>. Equimolar<br />
recognition of free and complexed <strong>PSA</strong> <strong>for</strong>ms is<br />
essential <strong>for</strong> accurate <strong>PSA</strong> testing. Inaccurate quantification<br />
of <strong>PSA</strong> around the 4.0 ng/mL <strong>cut</strong>-<strong>off</strong> can yield<br />
a false positive or a false negative result, depending on<br />
the direction of the distortion, and may thus lead to<br />
inappropriate management of the patient [Figure 2].<br />
In order to compensate <strong>for</strong> the non-equimolar<br />
response of some <strong>PSA</strong> <strong>assays</strong>, Thomas Stanley, a<br />
clinical urologist at Stan<strong>for</strong>d University, proposed in<br />
the mid-1990s a <strong>PSA</strong> standard containing both complexed<br />
and free <strong>PSA</strong> in a ratio of 90:10 respectively [5].<br />
This became the basis <strong>for</strong> the new standard adopted<br />
by WHO in 1999, which has its mass assigned using a<br />
method based on the use of a particular molar extinction<br />
coefficient, different from the original Hybritech<br />
standard. Although the original intention was to<br />
establish an ‘equimolarity standard’, this has actually<br />
led to the creation of a new WHO ‘mass standard’<br />
<strong>for</strong> <strong>PSA</strong>.<br />
However, many clinicians are still unaware that<br />
restandardising a <strong>PSA</strong> assay from an original<br />
Hybritech calibration to a WHO calibration may<br />
result in potential under-recovery of <strong>PSA</strong> <strong>value</strong>s. This<br />
is because <strong>assays</strong> calibrated to the new WHO standard<br />
show a negative bias in mass units compared<br />
<strong>with</strong> the Hybritech calibrated <strong>assays</strong> [6]. <strong>The</strong> original<br />
Hybritech Tandem-R calibration was based on an<br />
internal reference preparation of purified human<br />
<strong>PSA</strong> and yields <strong>PSA</strong> results about 20% higher than<br />
the new WHO standard [6]. <strong>The</strong> European Group
on Tumour Markers (EGTM) clearly<br />
recommends that "every laboratory<br />
report should contain the name of the<br />
assay used and a valid reference range,<br />
specifically generated <strong>for</strong> this assay."<br />
In addition, some European countries<br />
require laboratories to report <strong>PSA</strong> and<br />
free <strong>PSA</strong> <strong>value</strong>s standardised to WHO<br />
96/670 and 96/668, respectively.<br />
recalibrating <strong>for</strong> WHO<br />
standards<br />
In order to verify the Hybritech standard<br />
against the WHO standard, Beckman<br />
Coulter Immunodiagnostics (BCI)<br />
developed WHO primary calibrators to<br />
determine the ‘<strong>off</strong>set’ when compared<br />
directly against the original Hybritech<br />
calibration. This indicated how much<br />
adjustment was <strong>need</strong>ed <strong>for</strong> both <strong>total</strong> and<br />
free <strong>PSA</strong> across the range of the assay.<br />
When Beckman Coulter carried this out<br />
it was found an adjustment of 20% was<br />
<strong>need</strong>ed <strong>for</strong> both <strong>assays</strong>.<br />
<strong>The</strong> validation process involved a statistical<br />
analysis of how the WHO standardisation<br />
impacts on the original Hybritech<br />
data used to establish the 4.0 ng/mL<br />
<strong>cut</strong>-<strong>off</strong> [2]. During this process it became<br />
apparent that the different calibrations<br />
yielded different results, indicating that<br />
the 4.0 ng/mL <strong>cut</strong>-<strong>off</strong> would not provide<br />
optimal clinical sensitivity and specificity<br />
<strong>for</strong> the WHO calibration. <strong>The</strong> 3.1<br />
ng/mL <strong>cut</strong>-<strong>off</strong> <strong>for</strong> the WHO calibrated<br />
method was compared against the original<br />
Hybritech data set that was used to<br />
determine the <strong>cut</strong> of 4.0 ng/mL. From<br />
this, the new <strong>cut</strong>-<strong>off</strong> of 3.1 ng/mL was<br />
verified as being appropriate [Table 1].<br />
A sensitivity and specificity of 81.6% and<br />
48.0% respectively was maintained at this<br />
<strong>cut</strong>-<strong>off</strong> [4].<br />
Use of the new <strong>cut</strong>-<strong>off</strong> of 3.1 ng/mL<br />
does not impact the clinical sensitivity<br />
of tests involving<br />
the ratio of free<br />
<strong>PSA</strong> to <strong>total</strong> <strong>PSA</strong><br />
(percentage of<br />
free <strong>PSA</strong>) [Table<br />
2] because the<br />
WHO calibration<br />
<strong>value</strong>s <strong>for</strong> both<br />
<strong>total</strong> and free <strong>PSA</strong><br />
exhibit similar<br />
differences (approximately 20%) from<br />
the Hybritech calibration <strong>value</strong>s.<br />
Table 1. WHO calibration 3.1 ng/mL <strong>total</strong> <strong>PSA</strong> <strong>cut</strong>-<strong>off</strong> is clinically<br />
equivalent to Hybritech calibration 4.0 ng/mL <strong>cut</strong>-<strong>off</strong>.<br />
Why is a <strong>lower</strong> <strong>PSA</strong> <strong>cut</strong>-<strong>off</strong> important<br />
after WHO<br />
recalibration?<br />
When samples taken from men <strong>with</strong><br />
prostate cancer were evaluated using<br />
a 3.1 or a 4.0 ng/mL <strong>cut</strong>-<strong>off</strong> <strong>for</strong> the<br />
WHO calibration, use of the higher<br />
<strong>cut</strong>-<strong>off</strong> missed 15% of prostate cancers<br />
which were<br />
detected by using<br />
the <strong>cut</strong><strong>off</strong> of 3.1<br />
ng/mL [Table 3].<br />
Table 3a shows<br />
<strong>PSA</strong> results <strong>for</strong><br />
cancer patients<br />
using a 4.0 ng/<br />
mL <strong>cut</strong>-<strong>off</strong> <strong>with</strong><br />
the Hybritech<br />
calibration and<br />
a 3.1 ng/mL<br />
Table 2. Equivalent percentage free <strong>PSA</strong> results <strong>for</strong> the Hybritech and<br />
WHO calibrations.<br />
<strong>cut</strong>-<strong>off</strong> <strong>with</strong> the<br />
WHO calibration.<br />
Table 3b<br />
shows the <strong>PSA</strong> results <strong>for</strong> the same cancer<br />
patients when their samples were<br />
analysed using a 4.0 ng/mL <strong>cut</strong>-<strong>off</strong> <strong>with</strong><br />
both the Hybritech and the WHO calibrations.<br />
It is apparent that using<br />
the 4.0 ng/mL <strong>cut</strong>-<strong>off</strong> <strong>with</strong> the<br />
WHO calibration fails to pick up<br />
38 of the 255 patients (15%) whose<br />
prostate cancer may be missed as a<br />
result. Laboratories <strong>need</strong> to make two<br />
key points clear to their clinicians.<br />
First, there is a new <strong>cut</strong>-<strong>off</strong> <strong>value</strong> of 3.1<br />
ng/mL <strong>for</strong> the WHO calibrated Access<br />
Hybritech <strong>PSA</strong> assay. Secondly, this<br />
new <strong>cut</strong><strong>off</strong> cannot be automatically<br />
applied to other methods, as <strong>cut</strong><strong>off</strong><br />
validation must be assay specific<br />
according to EGTM. It is important<br />
that other manufacturers invest in the<br />
individual validation and verification<br />
of their WHO calibrated <strong>assays</strong>.<br />
Further in<strong>for</strong>mation<br />
Technical in<strong>for</strong>mation <strong>for</strong> Beckman Coulter <strong>assays</strong><br />
on the Hybritech calibration and WHO calibration<br />
options, the <strong>lower</strong> <strong>total</strong> <strong>PSA</strong> <strong>cut</strong>-<strong>off</strong> required when<br />
calibrating to the WHO standard and QC <strong>value</strong>s<br />
<strong>for</strong> Hybritech and WHO calibrations are available<br />
from mjeremaes@beckmancoulter.com. Please note<br />
that the WHO ca calibrated assay is not currently<br />
available in the US.<br />
references<br />
1. H. Ballentine Carter et al.<br />
Longitudinal Evaluation of Prostate-<br />
Specific Antigen Levels in Men With<br />
and Without Prostate Disease. JAMA<br />
1992; 267: No 16.<br />
2. Blijenberg BG, Storm BN, Kruger<br />
As published in April 2007<br />
AE and Schroder<br />
FH. On the standardisation<br />
of <strong>total</strong><br />
prostate-specific<br />
antigen: an exercise<br />
<strong>with</strong> two referencepreparations.<br />
Clin Chem<br />
Lab Med 1999;<br />
37: 545-552.<br />
3. Catalona WJ<br />
et al. Selection<br />
of optimal <strong>PSA</strong><br />
<strong>cut</strong><strong>off</strong> <strong>for</strong> early<br />
detection of prostate cancer, ROC<br />
curves. J Urol 1994; 152:2037–2042.<br />
4. Catalona WJ et al. Comparison of<br />
digital rectal examination and serum<br />
prostate specific antigen in the early<br />
detection of prostate cancer: Results<br />
of a multicenter clinical trial of 6,630<br />
men. J Urol 1994; 151: 1283–1290.<br />
5. Stamey TA, Teplow DB, Graves<br />
HC. Identity of <strong>PSA</strong> purified from<br />
seminal fluid by different methods:<br />
comparison by amino acid analysis<br />
and assigned extinction coefficients.<br />
Prostate 1995; 27: 198–203.<br />
6. Link RE et al. Variation in prostate<br />
specific antigen results from 2<br />
different assay plat<strong>for</strong>ms: Clinical<br />
impact on 2,304 patients undergoing<br />
prostate cancer screening. J Urol<br />
2004; 171: 2234–2238.<br />
7. Semjonow A, Albrecht W, Bialk P,<br />
Gerl A, Lamerz R, Schmid HP and van<br />
Poppel H: Tumour markers in prostate<br />
cancer: EGTM recommendations.<br />
Anticancer Res 1999; 19: 2799-2801.<br />
Table 3. Distribution, by <strong>PSA</strong> <strong>cut</strong>-<strong>off</strong>, of subjects tested <strong>for</strong> prostate<br />
cancer by <strong>PSA</strong> test.<br />
<strong>The</strong> author<br />
Veronique Jarrige, Ph.D.<br />
European Scientific Manager,<br />
Immunodiagnostics,<br />
Beckman Coulter Europe,<br />
c/o 22 rue Juste-Olivier,<br />
P.O. Box 1044,<br />
1260 Nyon 1, Switzerland<br />
Tel +33 490 50 64 72<br />
e-mail: vjarrige@beckman.com<br />
Go to Hotline www.cli-online.com & tick 23465