

Urology & Kidney Disease News - Cleveland Clinic
Urology & Kidney Disease News - Cleveland Clinic
Urology & Kidney Disease News - Cleveland Clinic

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
32 <strong>Urology</strong> & <strong>Kidney</strong> <strong>Disease</strong> <strong>News</strong><br />
<strong>Kidney</strong><br />
Auto-Transplantation for Intractable Nephrolithiasis<br />
Alvin Wee, MD, Stuart Flechner, MD, Ho Y. Tiong, MD, Ray<br />
Littleton, MD, and Mark J. Noble, MD<br />
Auto-transplantation historically has been used to treat a<br />
variety of disorders including bench surgical reconstruction<br />
of the renal artery for aneurism; bench excision of a malignant<br />
tumor; therapeutic intervention for Loin-Pain,<br />
Hematuria Syndrome; and preservation of a kidney when<br />
the ureter must be excised for a variety of reasons (e.g., long<br />
strictures or ureteral tumors). There are few reports of<br />
auto-transplantation to treat medically refractory stone<br />
disease, and even fewer reports of bilateral treatment. Yet,<br />
the literature suggests that the procedure is generally successful<br />
in both preserving the kidney(s) and also helping<br />
the patient to pass stones more easily (via pyelovesicostomy).<br />
We believe this procedure should be offered to more<br />
patients despite its complexity, as it has a high success rate<br />
in reducing the inevitable dependence on narcotics seen in<br />
many recurrent stone patients. It also seems to greatly<br />
reduce the tendency to form new stones. We present our<br />
results to date in a combined series with Henry Ford<br />
Hospital.<br />
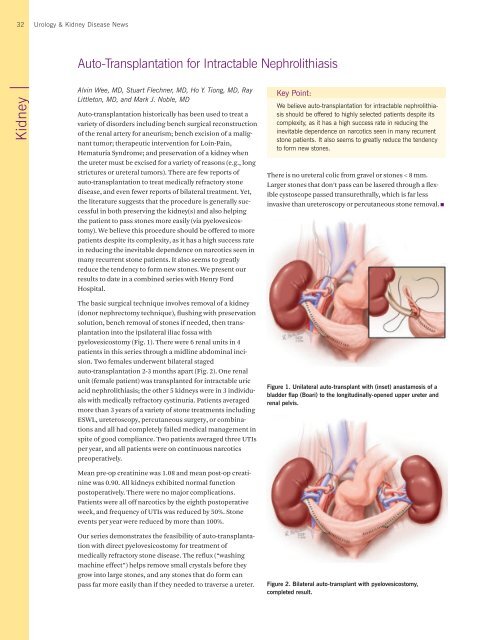
The basic surgical technique involves removal of a kidney<br />
(donor nephrectomy technique), flushing with preservation<br />
solution, bench removal of stones if needed, then transplantation<br />
into the ipsilateral iliac fossa with<br />
pyelovesicostomy (Fig. 1). There were 6 renal units in 4<br />
patients in this series through a midline abdominal incision.<br />
Two females underwent bilateral staged<br />
auto-transplantation 2-3 months apart (Fig. 2). One renal<br />
unit (female patient) was transplanted for intractable uric<br />
acid nephrolithiasis; the other 5 kidneys were in 3 individuals<br />
with medically refractory cystinuria. Patients averaged<br />
more than 3 years of a variety of stone treatments including<br />
ESWL, ureteroscopy, percutaneous surgery, or combinations<br />
and all had completely failed medical management in<br />
spite of good compliance. Two patients averaged three UTIs<br />
per year, and all patients were on continuous narcotics<br />
preoperatively.<br />
Mean pre-op creatinine was 1.08 and mean post-op creatinine<br />
was 0.90. All kidneys exhibited normal function<br />
postoperatively. There were no major complications.<br />
Patients were all off narcotics by the eighth postoperative<br />
week, and frequency of UTIs was reduced by 50%. Stone<br />
events per year were reduced by more than 100%.<br />
Our series demonstrates the feasibility of auto-transplantation<br />
with direct pyelovesicostomy for treatment of<br />
medically refractory stone disease. The reflux (“washing<br />
machine effect”) helps remove small crystals before they<br />
grow into large stones, and any stones that do form can<br />
pass far more easily than if they needed to traverse a ureter.<br />
Key Point:<br />
We believe auto-transplantation for intractable nephrolithiasis<br />
should be offered to highly selected patients despite its<br />
complexity, as it has a high success rate in reducing the<br />
inevitable dependence on narcotics seen in many recurrent<br />
stone patients. It also seems to greatly reduce the tendency<br />
to form new stones.<br />
There is no ureteral colic from gravel or stones < 8 mm.<br />
Larger stones that don’t pass can be lasered through a flexible<br />
cystoscope passed transurethrally, which is far less<br />
invasive than ureteroscopy or percutaneous stone removal.<br />
Figure 1. Unilateral auto-transplant with (inset) anastamosis of a<br />
bladder flap (Boari) to the longitudinally-opened upper ureter and<br />
renal pelvis.<br />
Figure 2. Bilateral auto-transplant with pyelovesicostomy,<br />
completed result.














