

Urology & Kidney Disease News - Cleveland Clinic
Urology & Kidney Disease News - Cleveland Clinic
Urology & Kidney Disease News - Cleveland Clinic

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
40 <strong>Urology</strong> & <strong>Kidney</strong> <strong>Disease</strong> <strong>News</strong><br />
Female <strong>Urology</strong><br />
Excision of Extruded Vaginal Mesh<br />
Howard B. Goldman, MD<br />
Transvaginal prolapse repairs utilizing mesh recently have<br />
become popular because of dissatisfaction with recurrence<br />
rates of traditional transvaginal repairs. Along with the<br />
increasing numbers of these repairs being performed we<br />
have seen an increase in referrals for complications related<br />
to mesh use. One of the common complications is extrusion<br />
of the mesh into the vagina. In women who are not<br />
sexually active this may be asymptomatic, but in some it<br />
may cause vaginal discharge. If a woman is sexually active,<br />
it may cause dyspareunia or pain to her sexual partner<br />
during intercourse. Published extrusion rates are about<br />
10% but with more experience and better vaginal wall dissection<br />
techniques, the rate has dropped to the 2-4% range.<br />
Nevertheless, given the large number of these mesh procedures<br />
being performed, there are many women presenting<br />
with post-operative vaginal mesh extrusion.<br />
We have found that the majority of these patients can be<br />
treated in a straightforward manner with excision of the<br />
extruded vaginal mesh.<br />
The technique involves:<br />
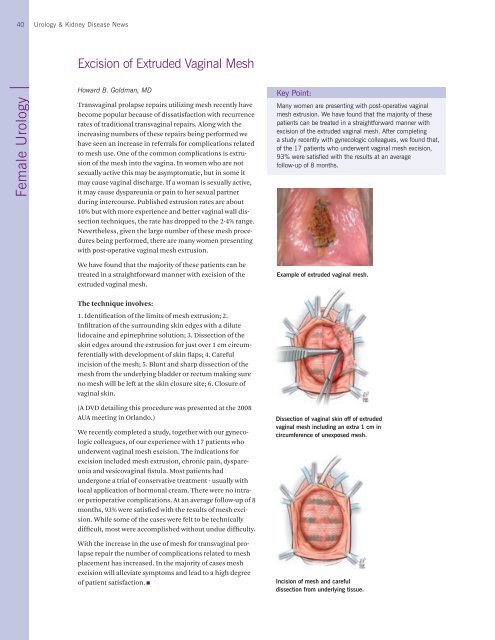
1. Identification of the limits of mesh extrusion; 2.<br />
Infiltration of the surrounding skin edges with a dilute<br />
lidocaine and epinephrine solution; 3. Dissection of the<br />
skin edges around the extrusion for just over 1 cm circumferentially<br />
with development of skin flaps; 4. Careful<br />
incision of the mesh; 5. Blunt and sharp dissection of the<br />
mesh from the underlying bladder or rectum making sure<br />
no mesh will be left at the skin closure site; 6. Closure of<br />
vaginal skin.<br />
(A DVD detailing this procedure was presented at the 2008<br />
AUA meeting in Orlando.)<br />
We recently completed a study, together with our gynecologic<br />
colleagues, of our experience with 17 patients who<br />
underwent vaginal mesh excision. The indications for<br />
excision included mesh extrusion, chronic pain, dyspareunia<br />
and vesicovaginal fistula. Most patients had<br />
undergone a trial of conservative treatment - usually with<br />
local application of hormonal cream. There were no intra-<br />
or perioperative complications. At an average follow-up of 8<br />
months, 93% were satisfied with the results of mesh excision.<br />
While some of the cases were felt to be technically<br />
difficult, most were accomplished without undue difficulty.<br />
With the increase in the use of mesh for transvaginal prolapse<br />
repair the number of complications related to mesh<br />
placement has increased. In the majority of cases mesh<br />
excision will alleviate symptoms and lead to a high degree<br />
of patient satisfaction.<br />
Key Point:<br />
Many women are presenting with post-operative vaginal<br />
mesh extrusion. We have found that the majority of these<br />
patients can be treated in a straightforward manner with<br />
excision of the extruded vaginal mesh. After completing<br />
a study recently with gynecologic colleagues, we found that,<br />
of the 17 patients who underwent vaginal mesh excision,<br />
93% were satisfied with the results at an average<br />
follow-up of 8 months.<br />
Example of extruded vaginal mesh.<br />
Dissection of vaginal skin off of extruded<br />
vaginal mesh including an extra 1 cm in<br />
circumference of unexposed mesh.<br />
Incision of mesh and careful<br />
dissection from underlying tissue.














