Volvulus in two preterm infants: abdominal massage as a risk factor?
Volvulus in two preterm infants: abdominal massage as a risk factor?
Volvulus in two preterm infants: abdominal massage as a risk factor?

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
SWISS SOCIETY OF NEONATOLOGY<br />
<strong>Volvulus</strong> <strong>in</strong> <strong>two</strong> <strong>preterm</strong><br />
<strong>in</strong>fants: abdom<strong>in</strong>al <strong>m<strong>as</strong>sage</strong><br />
<strong>as</strong> a <strong>risk</strong> <strong>factor</strong>?<br />
DECEMBER 2006
Par<strong>as</strong>kevopoulos E, Arlettaz R, Neonatal Intensive<br />
Care Unit, University Hospital Zurich, Switzerland<br />
© Swiss Society of Neonatology, Thom<strong>as</strong> M Berger, Webm<strong>as</strong>ter
This is a report about <strong>two</strong> <strong>preterm</strong> <strong>in</strong>fants with a di-<br />
agnosis of <strong>in</strong>test<strong>in</strong>al volvulus without identifiable<br />
predispos<strong>in</strong>g <strong>in</strong>test<strong>in</strong>al malformation.<br />
The first c<strong>as</strong>e <strong>in</strong>volves an 800 g female <strong>in</strong>fant born<br />
to a 4-year-old G /P mother by cesarean section at<br />
7 weeks of gestation because of preeclampsia and<br />
silent CTG. Apgar scores were , 7, 6 at 1, 5, and 10<br />
m<strong>in</strong>utes, respectively. The baby developed respiratory<br />
distress, necessitat<strong>in</strong>g n<strong>as</strong>al CPAP and on the second<br />
day of life mechanical ventilation. She w<strong>as</strong> extubated<br />
on the third day of life and placed on n<strong>as</strong>al CPAP.<br />
Dur<strong>in</strong>g the follow<strong>in</strong>g weeks, the abdomen w<strong>as</strong> no-<br />
ticed to be distended but soft, and defecation w<strong>as</strong><br />
difficult although the baby w<strong>as</strong> exclusively fed with<br />
bre<strong>as</strong>t milk. Intensive abdom<strong>in</strong>al <strong>m<strong>as</strong>sage</strong> w<strong>as</strong> perfor-<br />
med several times a day by the nurses. The baby w<strong>as</strong><br />
also reported to be rather fussy. On the nd day of<br />
life, she became acutely ill with a distended and tense<br />
abdomen (Fig. 1), hypothermia ( 5.9° C), poor sk<strong>in</strong><br />
perfusion, and apne<strong>as</strong>. Stools were normal but g<strong>as</strong>tric<br />
<strong>as</strong>pirates were bilious. The abdom<strong>in</strong>al X-ray showed<br />
markedly dilated loops of bowel with air-fluid levels<br />
and no evidence for necrotiz<strong>in</strong>g enterocolitis (Fig. ).<br />
The baby w<strong>as</strong> <strong>in</strong>tubated, put on antibiotics and trans-<br />
ferred to the pediatric surgical unit. On laparotomy,<br />
volvulus of the small bowel w<strong>as</strong> diagnosed. 1 0 cm<br />
of small bowel were resected and a jejunostomy and<br />
colostomy were placed. The postoperative course w<strong>as</strong><br />
CASE REPORTS<br />
CASE 1
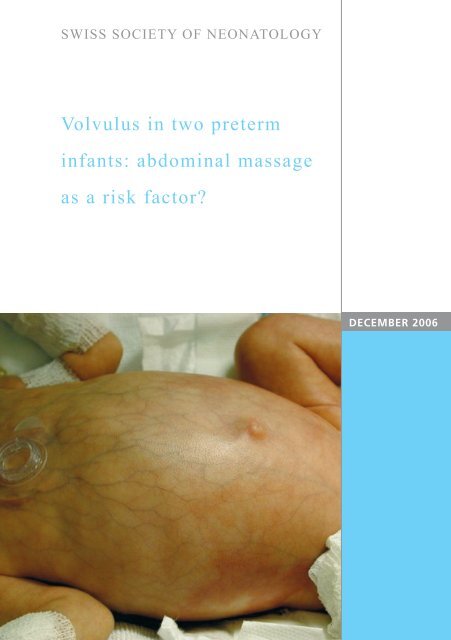
Fig. 1<br />
Tensely distended abdomen with <strong>in</strong>cre<strong>as</strong>ed venous<br />
mark<strong>in</strong>gs.<br />
4
5<br />
Abdom<strong>in</strong>al x-ray (horizontal beam technique) show-<br />
<strong>in</strong>g dilated loops of bowel but no free air or pneu-<br />
matosis <strong>in</strong>test<strong>in</strong>alis.<br />
Fig. 2
CASE 2<br />
complicated by several episodes of nosocomial <strong>in</strong>fec-<br />
tions and stenosis of the stoma. The baby w<strong>as</strong> dischar-<br />
ged from hospital <strong>in</strong> good condition at a corrected age<br />
of seven months with a weight of 51 0 g.<br />
The second c<strong>as</strong>e w<strong>as</strong> very similar: a <strong>preterm</strong> 800 g<br />
female <strong>in</strong>fant w<strong>as</strong> born to 7-year-old G1/P1 by<br />
cesarean section at 7 weeks of gestation because of<br />
maternal preeclampsia. Apgar scores were 7, 9, and<br />
9 at 1, 5, and 10 m<strong>in</strong>utes, respectively. The baby w<strong>as</strong><br />
placed on n<strong>as</strong>al CPAP because of RDS. With<strong>in</strong> the first<br />
<strong>two</strong> hours of life she required mechanical ventilation<br />
and surfactant w<strong>as</strong> given. She w<strong>as</strong> extubated on the<br />
4th day of life and put on n<strong>as</strong>al CPAP. Enteral feed<strong>in</strong>gs<br />
with bre<strong>as</strong>t milk were started on the second day of life<br />
and tolerated without problems. Abdom<strong>in</strong>al <strong>m<strong>as</strong>sage</strong><br />
w<strong>as</strong> performed several times a day because of abdomi-<br />
nal distension felt to be secondary to n<strong>as</strong>al CPAP. On<br />
the 19th day of life, the baby developed cl<strong>in</strong>ical (tense,<br />
distended abdomen, absence of stools, biliary g<strong>as</strong>tric<br />
<strong>as</strong>pirates) and radiological signs of an ileus (Fig. ).<br />
She w<strong>as</strong> described <strong>as</strong> be<strong>in</strong>g uncomfortable and cry<strong>in</strong>g<br />
<strong>in</strong>consolably. An enema with normal sal<strong>in</strong>e did not lead<br />
to any improvement. Antibiotics were started and the<br />
baby w<strong>as</strong> transferred to the pediatric surgery unit. On<br />
laparotomy, volvulus of the ileum w<strong>as</strong> found. 14 cm of<br />
ileum were resected and an end-to-end an<strong>as</strong>tomosis<br />
w<strong>as</strong> performed. The further course w<strong>as</strong> complicated by<br />
g<strong>as</strong>tro-esophageal reflux necessitat<strong>in</strong>g enteral feed<strong>in</strong>g<br />
through a jejunal tube for several weeks. The baby w<strong>as</strong><br />
6
7<br />
Babygram show<strong>in</strong>g dilated and thickened loops of<br />
bowel.<br />
Fig. 3
DISCUSSION<br />
discharged from hospital at a corrected age of seven<br />
weeks with a weight of 700 g.<br />
<strong>Volvulus</strong> of the small <strong>in</strong>test<strong>in</strong>es is rare <strong>in</strong> neonates (1).<br />
Malrotation, which occurs <strong>in</strong> 1/6000 live births, is a<br />
cl<strong>as</strong>sical <strong>risk</strong> <strong>factor</strong> for volvulus, but w<strong>as</strong> not present<br />
<strong>in</strong> both of the babies described ( ). Kitano et al. re-<br />
ported on 8 newborns with a diagnosis of volvulus<br />
and found a malrotation <strong>in</strong> 74% of the c<strong>as</strong>es ( ). In<br />
Nigeria, Ameh et al. analysed 8 newborns with vol-<br />
vulus: % of c<strong>as</strong>es were <strong>as</strong>sociated with malrotation,<br />
one c<strong>as</strong>e with a Meckel‘s diverticulum, one with <strong>in</strong>ter-<br />
nal herniation and one c<strong>as</strong>e with a ventriculoperitone-<br />
al shunt. In 9% of the newborns no etiology could<br />
be identified (4). None of the above mentioned condi-<br />
tions w<strong>as</strong> found <strong>in</strong> our patients. Recently, Billiemaz et<br />
al. described seven <strong>preterm</strong> <strong>in</strong>fants with volvulus and<br />
raised the hypothesis that abdom<strong>in</strong>al <strong>m<strong>as</strong>sage</strong> could<br />
be responsible for caus<strong>in</strong>g the volvulus (5). The seven<br />
premature <strong>in</strong>fants had a mean gestational age of 8<br />
weeks and volvulus occurred at an average postnatal<br />
age of 1 days. As soon <strong>as</strong> the babies were fed en-<br />
terally, enem<strong>as</strong> were given regularly, and abdom<strong>in</strong>al<br />
<strong>m<strong>as</strong>sage</strong> w<strong>as</strong> performed every three hours <strong>in</strong> order to<br />
stimulate peristalsis. Follow<strong>in</strong>g their observation, this<br />
rout<strong>in</strong>e <strong>in</strong>tervention w<strong>as</strong> def<strong>in</strong>itively discont<strong>in</strong>ued and<br />
no further c<strong>as</strong>es of volvulus have s<strong>in</strong>ce occurred.<br />
In the <strong>two</strong> reported c<strong>as</strong>es, we could not f<strong>in</strong>d any <strong>risk</strong><br />
8
9<br />
<strong>factor</strong> for the volvulus, except for repeated <strong>in</strong>tensive<br />
abdom<strong>in</strong>al <strong>m<strong>as</strong>sage</strong>. This procedure h<strong>as</strong> been aban-<br />
doned <strong>as</strong> a rout<strong>in</strong>e nurs<strong>in</strong>g procedure and h<strong>as</strong> only<br />
been used <strong>in</strong> select c<strong>as</strong>es. With this change of policy,<br />
no further c<strong>as</strong>es of volvulus have been observed <strong>in</strong><br />
our unit.<br />
CONCLUSION
REFERENCES 1. Chen Y, Tseng SH, Lai HS, Chen WJ. Primary volvulus of the<br />
ileum <strong>in</strong> a <strong>preterm</strong> <strong>in</strong>fant. J Formos Med Assoc 00 ;10 :<br />
896-898<br />
. Berseth CL and Peonaru D. Structural anomalies of the<br />
g<strong>as</strong>tro<strong>in</strong>test<strong>in</strong>al tract. In: Taeusch HW, Ballard RA, Gle<strong>as</strong>on CA.<br />
Avery‘s dise<strong>as</strong>es of the newborn, 8th edition ( 005),<br />
pp.1099-1100.<br />
. Kitano Y, H<strong>as</strong>hizume K, Ohkura M. Segmental small-bowel<br />
volvulus not <strong>as</strong>sociated with malrotation <strong>in</strong> childhood.<br />
Pediatr Surg Int 1995;10: 5- 8<br />
4. Ameh EA, Nmadu PT. Intest<strong>in</strong>al volvulus: aetiology, morbidity,<br />
and mortality <strong>in</strong> Nigerian children. Pediatr Surg Int 000;<br />
16:50-5<br />
5. Billiemaz K, Varlet F, Patural H, Rayet I, Tardieu D, Lavocat MP,<br />
Teyssier G. Intest<strong>in</strong>al volvulus <strong>in</strong> extremely premature <strong>in</strong>fants.<br />
Arch Pediatr 001;8:1181-1184<br />
10
SUPPORTED BY<br />
CONTACT<br />
Swiss Society of Neonatology<br />
www.neonet.ch<br />
webm<strong>as</strong>ter@neonet.ch<br />
concept & design by mesch.ch