Extraperiosteal Plating of Pronation-Abduction Ankle Fractures
Extraperiosteal Plating of Pronation-Abduction Ankle Fractures
Extraperiosteal Plating of Pronation-Abduction Ankle Fractures

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
143<br />
T HE JOURNAL OF BONE & JOINT SURGERY · SURGICAL TECHNIQUES MARCH 2008 · VOLUME 90-A · SUPPLEMENT 2, PART 1 · JBJS.ORG<br />
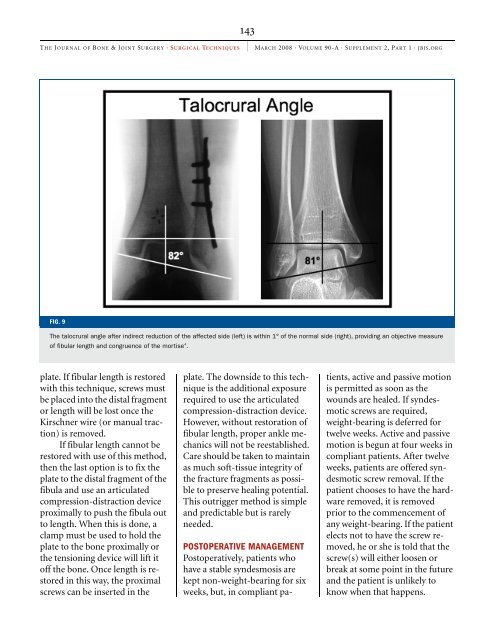
FIG. 9<br />
The talocrural angle after indirect reduction <strong>of</strong> the affected side (left) is within 1° <strong>of</strong> the normal side (right), providing an objective measure<br />
<strong>of</strong> fibular length and congruence <strong>of</strong> the mortise 4 .<br />
plate. If fibular length is restored<br />
with this technique, screws must<br />
be placed into the distal fragment<br />
or length will be lost once the<br />
Kirschner wire (or manual traction)<br />
is removed.<br />
If fibular length cannot be<br />
restored with use <strong>of</strong> this method,<br />
then the last option is to fix the<br />
plate to the distal fragment <strong>of</strong> the<br />
fibula and use an articulated<br />
compression-distraction device<br />
proximally to push the fibula out<br />
to length. When this is done, a<br />
clamp must be used to hold the<br />
plate to the bone proximally or<br />
the tensioning device will lift it<br />
<strong>of</strong>f the bone. Once length is restored<br />
in this way, the proximal<br />
screws can be inserted in the<br />
plate. The downside to this technique<br />
is the additional exposure<br />
required to use the articulated<br />
compression-distraction device.<br />
However, without restoration <strong>of</strong><br />
fibular length, proper ankle mechanics<br />
will not be reestablished.<br />
Care should be taken to maintain<br />
as much s<strong>of</strong>t-tissue integrity <strong>of</strong><br />
the fracture fragments as possible<br />
to preserve healing potential.<br />
This outrigger method is simple<br />
and predictable but is rarely<br />
needed.<br />
POSTOPERATIVE MANAGEMENT<br />
Postoperatively, patients who<br />
have a stable syndesmosis are<br />
kept non-weight-bearing for six<br />
weeks, but, in compliant pa-<br />
tients, active and passive motion<br />
is permitted as soon as the<br />
wounds are healed. If syndesmotic<br />
screws are required,<br />
weight-bearing is deferred for<br />
twelve weeks. Active and passive<br />
motion is begun at four weeks in<br />
compliant patients. After twelve<br />
weeks, patients are <strong>of</strong>fered syndesmotic<br />
screw removal. If the<br />
patient chooses to have the hardware<br />
removed, it is removed<br />
prior to the commencement <strong>of</strong><br />
any weight-bearing. If the patient<br />
elects not to have the screw removed,<br />
he or she is told that the<br />
screw(s) will either loosen or<br />
break at some point in the future<br />
and the patient is unlikely to<br />
know when that happens.