Extraperiosteal Plating of Pronation-Abduction Ankle Fractures
Extraperiosteal Plating of Pronation-Abduction Ankle Fractures
Extraperiosteal Plating of Pronation-Abduction Ankle Fractures

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
138<br />
T HE JOURNAL OF BONE & JOINT SURGERY · SURGICAL TECHNIQUES MARCH 2008 · VOLUME 90-A · SUPPLEMENT 2, PART 1 · JBJS.ORG<br />
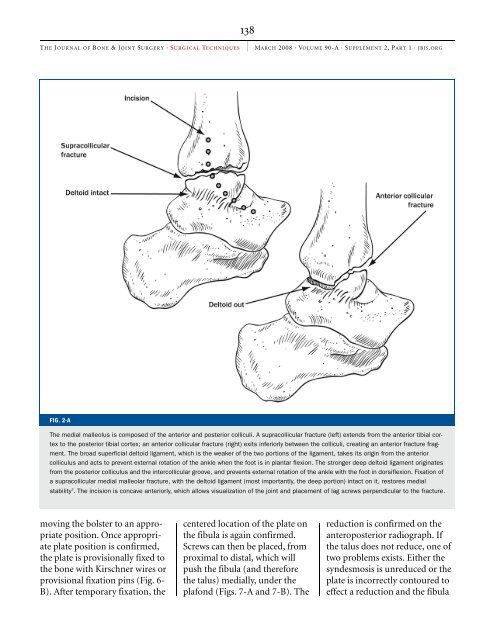
FIG. 2-A<br />
The medial malleolus is composed <strong>of</strong> the anterior and posterior colliculi. A supracollicular fracture (left) extends from the anterior tibial cortex<br />
to the posterior tibial cortex; an anterior collicular fracture (right) exits inferiorly between the colliculi, creating an anterior fracture fragment.<br />
The broad superficial deltoid ligament, which is the weaker <strong>of</strong> the two portions <strong>of</strong> the ligament, takes its origin from the anterior<br />
colliculus and acts to prevent external rotation <strong>of</strong> the ankle when the foot is in plantar flexion. The stronger deep deltoid ligament originates<br />
from the posterior colliculus and the intercollicular groove, and prevents external rotation <strong>of</strong> the ankle with the foot in dorsiflexion. Fixation <strong>of</strong><br />
a supracollicular medial malleolar fracture, with the deltoid ligament (most importantly, the deep portion) intact on it, restores medial<br />
stability 3 . The incision is concave anteriorly, which allows visualization <strong>of</strong> the joint and placement <strong>of</strong> lag screws perpendicular to the fracture.<br />
moving the bolster to an appropriate<br />
position. Once appropriate<br />
plate position is confirmed,<br />
the plate is provisionally fixed to<br />
the bone with Kirschner wires or<br />
provisional fixation pins (Fig. 6-<br />
B). After temporary fixation, the<br />
centered location <strong>of</strong> the plate on<br />
the fibula is again confirmed.<br />
Screws can then be placed, from<br />
proximal to distal, which will<br />
push the fibula (and therefore<br />
the talus) medially, under the<br />
plafond (Figs. 7-A and 7-B). The<br />
reduction is confirmed on the<br />
anteroposterior radiograph. If<br />
the talus does not reduce, one <strong>of</strong><br />
two problems exists. Either the<br />
syndesmosis is unreduced or the<br />
plate is incorrectly contoured to<br />
effect a reduction and the fibula