Extraperiosteal Plating of Pronation-Abduction Ankle Fractures
Extraperiosteal Plating of Pronation-Abduction Ankle Fractures
Extraperiosteal Plating of Pronation-Abduction Ankle Fractures

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
139<br />
T HE JOURNAL OF BONE & JOINT SURGERY · SURGICAL TECHNIQUES MARCH 2008 · VOLUME 90-A · SUPPLEMENT 2, PART 1 · JBJS.ORG<br />
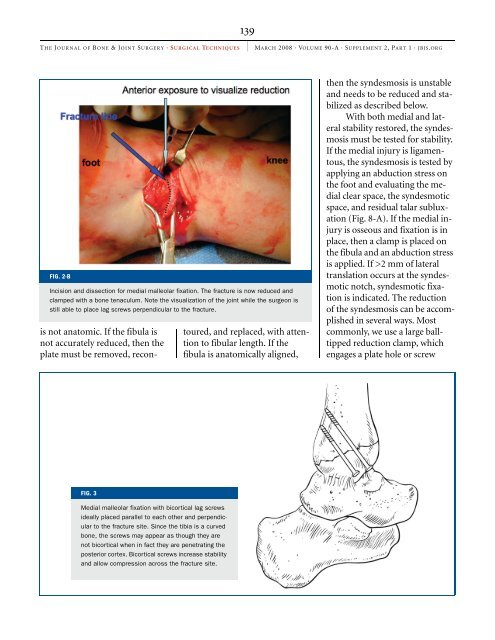
FIG. 2-B<br />
Incision and dissection for medial malleolar fixation. The fracture is now reduced and<br />
clamped with a bone tenaculum. Note the visualization <strong>of</strong> the joint while the surgeon is<br />
still able to place lag screws perpendicular to the fracture.<br />
is not anatomic. If the fibula is<br />
not accurately reduced, then the<br />
plate must be removed, recon-<br />
FIG. 3<br />
Medial malleolar fixation with bicortical lag screws<br />
ideally placed parallel to each other and perpendicular<br />
to the fracture site. Since the tibia is a curved<br />
bone, the screws may appear as though they are<br />
not bicortical when in fact they are penetrating the<br />
posterior cortex. Bicortical screws increase stability<br />
and allow compression across the fracture site.<br />
toured, and replaced, with attention<br />
to fibular length. If the<br />
fibula is anatomically aligned,<br />
then the syndesmosis is unstable<br />
and needs to be reduced and stabilized<br />
as described below.<br />
With both medial and lateral<br />
stability restored, the syndesmosis<br />
must be tested for stability.<br />
If the medial injury is ligamentous,<br />
the syndesmosis is tested by<br />
applying an abduction stress on<br />
the foot and evaluating the medial<br />
clear space, the syndesmotic<br />
space, and residual talar subluxation<br />
(Fig. 8-A). If the medial injury<br />
is osseous and fixation is in<br />
place, then a clamp is placed on<br />
the fibula and an abduction stress<br />
is applied. If >2 mm <strong>of</strong> lateral<br />
translation occurs at the syndesmotic<br />
notch, syndesmotic fixation<br />
is indicated. The reduction<br />
<strong>of</strong> the syndesmosis can be accomplished<br />
in several ways. Most<br />
commonly, we use a large balltipped<br />
reduction clamp, which<br />
engages a plate hole or screw