Pemphigus and BMZ diseases in people: presentations and ...
Pemphigus and BMZ diseases in people: presentations and ...
Pemphigus and BMZ diseases in people: presentations and ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Pemphigus</strong> <strong>and</strong> <strong>BMZ</strong> <strong>diseases</strong> <strong>in</strong> <strong>people</strong>: <strong>presentations</strong> <strong>and</strong> management<br />
Dr. Lizbeth Intong,<br />
Dermatology Fellow, St. George Hospital, Sydney, Australia<br />
Autoimmune bullous <strong>diseases</strong><br />
Autoimmune bullous <strong>diseases</strong> are due to circulat<strong>in</strong>g antibodies directed aga<strong>in</strong>st specific target antigens <strong>in</strong> the<br />
sk<strong>in</strong>. The cl<strong>in</strong>ical presentation of the disease is usually <strong>in</strong>fluenced by the location of the target antigen.<br />
Antibodies directed aga<strong>in</strong>st desmosomal prote<strong>in</strong>s that anchor the kerat<strong>in</strong>ocytes to one another <strong>in</strong> the<br />
epidermis result <strong>in</strong> pemphigus <strong>and</strong> its variants. Due to the superficial location of the antigens, blisters are<br />
usually flaccid <strong>and</strong> often present cl<strong>in</strong>ically as erosions. On the other h<strong>and</strong>, antibodies directed aga<strong>in</strong>st<br />
hemidesmosomal prote<strong>in</strong>s that anchor the basal kerat<strong>in</strong>ocytes to the basement membrane zone (<strong>BMZ</strong>) result<br />
<strong>in</strong> pemphigoid <strong>and</strong> its variants. In this group of <strong>diseases</strong>, blister<strong>in</strong>g is sub-epidermal <strong>and</strong> blisters appear tense.<br />
Diagnosis of these <strong>diseases</strong> is confirmed by histology <strong>and</strong> immunofluorescence. This review will focus on<br />
the cl<strong>in</strong>ical presentation of these various autoimmune blister<strong>in</strong>g <strong>diseases</strong>, as well as an overview of their<br />
management.<br />
Molecular Basis<br />
The sk<strong>in</strong> structure is ma<strong>in</strong>ta<strong>in</strong>ed by secure adhesion between kerat<strong>in</strong>ocytes with<strong>in</strong> the epidermis <strong>and</strong> between<br />
the basal kerat<strong>in</strong>ocytes <strong>and</strong> the underly<strong>in</strong>g basement membrane. The structures that are ma<strong>in</strong>ly responsible<br />
for adhesion are the desmosomes between epidermal kerat<strong>in</strong>ocytes <strong>and</strong> the hemidesmosomes anchor<strong>in</strong>g the<br />
basal kerat<strong>in</strong>ocytes to the basement membrane. Disruption of any of the prote<strong>in</strong>s conta<strong>in</strong>ed <strong>in</strong> these<br />
complexes leads to destabilization of the sk<strong>in</strong> structure lead<strong>in</strong>g to blisters. 1,2<br />
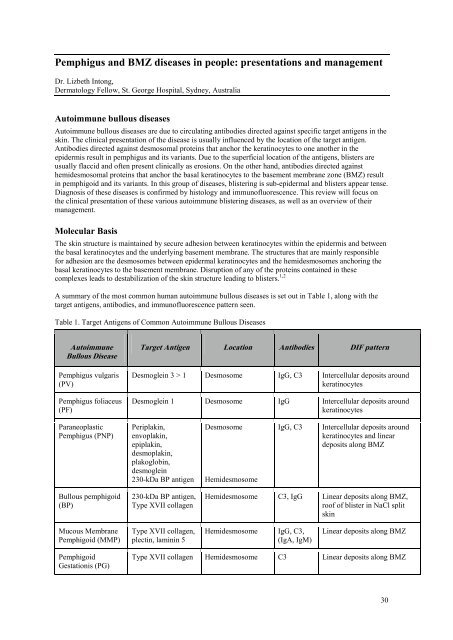
A summary of the most common human autoimmune bullous <strong>diseases</strong> is set out <strong>in</strong> Table 1, along with the<br />
target antigens, antibodies, <strong>and</strong> immunofluorescence pattern seen.<br />
Table 1. Target Antigens of Common Autoimmune Bullous Diseases<br />
Autoimmune<br />
Bullous Disease<br />
<strong>Pemphigus</strong> vulgaris<br />
(PV)<br />
<strong>Pemphigus</strong> foliaceus<br />
(PF)<br />
Paraneoplastic<br />
<strong>Pemphigus</strong> (PNP)<br />
Bullous pemphigoid<br />
(BP)<br />
Mucous Membrane<br />
Pemphigoid (MMP)<br />
Pemphigoid<br />
Gestationis (PG)<br />
Target Antigen Location Antibodies DIF pattern<br />
Desmogle<strong>in</strong> 3 > 1 Desmosome IgG, C3 Intercellular deposits around<br />
kerat<strong>in</strong>ocytes<br />
Desmogle<strong>in</strong> 1 Desmosome IgG Intercellular deposits around<br />
kerat<strong>in</strong>ocytes<br />
Periplak<strong>in</strong>,<br />
envoplak<strong>in</strong>,<br />
epiplak<strong>in</strong>,<br />
desmoplak<strong>in</strong>,<br />
plakoglob<strong>in</strong>,<br />
desmogle<strong>in</strong><br />
230-kDa BP antigen<br />
230-kDa BP antigen,<br />
Type XVII collagen<br />
Type XVII collagen,<br />
plect<strong>in</strong>, lam<strong>in</strong><strong>in</strong> 5<br />
Desmosome<br />
Hemidesmosome<br />
IgG, C3 Intercellular deposits around<br />
kerat<strong>in</strong>ocytes <strong>and</strong> l<strong>in</strong>ear<br />
deposits along <strong>BMZ</strong><br />
Hemidesmosome C3, IgG L<strong>in</strong>ear deposits along <strong>BMZ</strong>,<br />
roof of blister <strong>in</strong> NaCl split<br />
sk<strong>in</strong><br />
Hemidesmosome IgG, C3,<br />
(IgA, IgM)<br />
L<strong>in</strong>ear deposits along <strong>BMZ</strong><br />
Type XVII collagen Hemidesmosome C3 L<strong>in</strong>ear deposits along <strong>BMZ</strong><br />
30
Autoimmune<br />
Bullous Disease<br />
L<strong>in</strong>ear IgA Disease<br />
(LAD)<br />
Epidermolysis<br />
Bullosa (EBA)<br />
Dermatitis<br />
herpetiformis (DH)<br />
Diagnostic Tests<br />
Target Antigen Location Antibodies DIF pattern<br />
Type XVII collagen<br />
(97-kDa <strong>and</strong> 120kDa<br />
cleaved<br />
fragments)<br />
Type VII collagen<br />
(anchor<strong>in</strong>g fibrils)<br />
gliad<strong>in</strong>, reticulum,<br />
smooth muscle<br />
endomysium<br />
Hemidesmosome IgA L<strong>in</strong>ear deposits along <strong>BMZ</strong>,<br />
roof <strong>and</strong> floor of blister <strong>in</strong><br />
NaCl split sk<strong>in</strong><br />
Sub-basal layer IgG, C3 L<strong>in</strong>ear deposits along <strong>BMZ</strong>,<br />
floor of blister <strong>in</strong> NaCl split<br />
sk<strong>in</strong><br />
Dermal papillae IgA Granular <strong>in</strong> dermal papillary<br />
tips<br />
A rout<strong>in</strong>e sk<strong>in</strong> punch biopsy (3-4 mm) is taken from the edge of the blister, <strong>in</strong>clud<strong>in</strong>g a portion of normal<br />
sk<strong>in</strong> <strong>and</strong> this sent for haematoxyl<strong>in</strong> <strong>and</strong> eos<strong>in</strong> (H&E) sta<strong>in</strong><strong>in</strong>g. A biopsy is helpful <strong>in</strong> mak<strong>in</strong>g the diagnosis<br />
s<strong>in</strong>ce it will show the level of the split (<strong>in</strong>traepidermal for pemphigus <strong>and</strong> subepidermal for pemphigoid). It<br />
will also show the <strong>in</strong>flammatory cells which are a clue to the disease. Bullous pemphigoid, for example, has<br />
a predom<strong>in</strong>antly eos<strong>in</strong>ophilic <strong>in</strong>filtrate, which accounts for the pruritus associated with the disease. L<strong>in</strong>ear<br />
IgA disease, on the other h<strong>and</strong>, is associated with a neutrophilic <strong>in</strong>filtrate.<br />
While do<strong>in</strong>g sk<strong>in</strong> biopsies, it is also important to take a perilesional biopsy for direct immunofluorescence<br />
(DIF). This method detects antibodies deposited with<strong>in</strong> the patient’s tissue. Antibodies have the fluorescent<br />
dye attached. Fluoresce<strong>in</strong>-conjugated antibodies directed aga<strong>in</strong>st complement fractions (C3, fibr<strong>in</strong>ogen) <strong>and</strong><br />
immunoglobul<strong>in</strong>s (IgG, IgA, IgM) are placed on frozen sections of the tissue. A positive fluorescence<br />
(graded on <strong>in</strong>tensity) <strong>in</strong> a particular pattern confirms the diagnosis. The patient’s tissue may also be<br />
<strong>in</strong>cubated <strong>in</strong> 1 mol/litre NaCl prior to perform<strong>in</strong>g the DIF. This technique <strong>in</strong>duces cleavage through the<br />
lam<strong>in</strong>a lucida, <strong>and</strong> is useful <strong>in</strong> differentiat<strong>in</strong>g autoimmune <strong>diseases</strong> with a similar DIF pattern by observ<strong>in</strong>g<br />
where the IgG or C3 localizes (i.e. dermal roof pattern for BP <strong>and</strong> dermal floor pattern for EBA).<br />
Serum may also be sent for <strong>in</strong>direct immunofluorescence (IIF) which is useful as a confirmatory test. This is<br />
used to detect circulat<strong>in</strong>g autoantibodies. In this sett<strong>in</strong>g, antibodies do not have the fluorescent dye attached.<br />
This method uses serum with fluoresce<strong>in</strong>-conjugated human anti-immunoglobul<strong>in</strong> aga<strong>in</strong>st a mucosal<br />
substrate such as monkey oesophagus or rat bladder.<br />
<strong>Pemphigus</strong> vulgaris<br />
Cl<strong>in</strong>ical<br />
• This disease <strong>in</strong>volves the sk<strong>in</strong> <strong>and</strong> mucous membranes<br />
• Age 40-60 years<br />
• HLA Associations: HLA DRB1*1454, DRB1*1401 3<br />
• The oral mucosa is usually the first site of <strong>in</strong>volvement, followed by the sk<strong>in</strong> months later<br />
• May be fatal if untreated<br />
• Flaccid blisters rapidly becom<strong>in</strong>g erosions<br />
• (+) Nikolsky sign (extension of blister upon apply<strong>in</strong>g lateral pressure)<br />
• Other variants: drug-<strong>in</strong>duced pemphigus (penicillam<strong>in</strong>e, nifedip<strong>in</strong>e, captopril), pemphigus vegetans<br />
(<strong>in</strong>volves sk<strong>in</strong> folds)<br />
Histology<br />
• Suprabasal blister with acantholysis<br />
IF - see table 1<br />
31
Management<br />
• Systemic corticosteroids are ma<strong>in</strong>stay: Prednisone 1 mg/kg/day +/- other immunosuppressives<br />
• Azathiopr<strong>in</strong>e, Methotrexate, Cyclophosphamide, Mycophenolate mofetil, IVIG, Rituximab,<br />
plasmapheresis<br />
Course <strong>and</strong> prognosis<br />
• Common cause of death is <strong>in</strong>fection due to immunosuppression needed to treat the disease<br />
<strong>Pemphigus</strong> foliaceus<br />
Cl<strong>in</strong>ical<br />
• May be localised or generalised<br />
• Shallow, flaccid blisters rapidly becom<strong>in</strong>g scaly, crusted erosions, may coalesce <strong>in</strong>to large denuded areas<br />
• Mucous membranes generally not affected<br />
• (+) Nikolsky sign (extension of blister upon apply<strong>in</strong>g lateral pressure)<br />
• Other variants: fogo selvagem (endemic PF associated with black fly Simulium nigrimanum <strong>in</strong> Brazil),<br />
pemphigus erythematosus (localised to cheeks <strong>and</strong> forehead, may have (+) ANA)<br />
Histology<br />
• Intraepidermal blister at the granular layer with acantholysis<br />
IF - see table 1<br />
Management<br />
• Topical corticosteroids for localised PF<br />
• Systemic corticosteroids or other immunosuppressives <strong>in</strong> recalcitrant disease<br />
Course <strong>and</strong> prognosis<br />
• Good if therapy <strong>in</strong>stituted early<br />
Paraneoplastic pemphigus<br />
Cl<strong>in</strong>ical<br />
• This is due to an underly<strong>in</strong>g malignancy (tumour antigens evoke an immune response lead<strong>in</strong>g to blisters)<br />
• Most common tumours: leukaemia, lymphoma, Waldenstroms’s macroglobul<strong>in</strong>aemia, sarcomas,<br />
thymoma, Castleman’s disease<br />
• 100% have mucosal <strong>in</strong>volvement, highly variable cutaneous lesions<br />
Histology<br />
• Suprabasal blister with acantholysis, basal vacuolation, dyskeratotic kerat<strong>in</strong>ocytes<br />
IF - see table 1<br />
• In addition, rat bladder transitional epithelium separates it from PV <strong>and</strong> PF as desmogle<strong>in</strong>s present <strong>in</strong><br />
stratified squamous epithelium only<br />
Management<br />
• Systemic corticosteroids are ma<strong>in</strong>stay: Prednisone 1 mg/kg/day +/- other immunosuppressives<br />
• Azathiopr<strong>in</strong>e, Methotrexate, Cyclophosphamide, Mycophenolate mofetil, IVIG, Rituximab,<br />
plasmapheresis<br />
Course <strong>and</strong> prognosis<br />
• High mortality (75-80%) due to underly<strong>in</strong>g neoplasm <strong>and</strong> medications required to treat this<br />
Bullous Pemphigoid<br />
Cl<strong>in</strong>ical<br />
32
• Subepidermal blister<strong>in</strong>g disease<br />
• Age > 60 years<br />
• May start as an urticarial eruption (very pruritic)<br />
• Tense blisters, common locations: abdomen, flexor surfaces of forearms, <strong>in</strong>ner thighs<br />
• (-) Nikolsky sign<br />
Histology<br />
• Subepidermal blister with prom<strong>in</strong>ent eos<strong>in</strong>ophilic <strong>in</strong>filtration<br />
IF - see table 1<br />
Management<br />
• Topical steroids or systemic corticosteroids +/- other immunosuppressives<br />
• Tetracycl<strong>in</strong>e +/- Nicot<strong>in</strong>amide, Azathiopr<strong>in</strong>e, Mycophenolate mofetil, Methotrexate, Cyclophosphamide<br />
Course <strong>and</strong> prognosis<br />
• Self-limited with good prognosis<br />
• 50% enter remission with<strong>in</strong> 2-6 years<br />
Mucous Membrane Pemphigoid (Cicatricial Pemphigoid)<br />
Cl<strong>in</strong>ical<br />
• Erosive lesions of sk<strong>in</strong> <strong>and</strong> mucous membranes<br />
• Sk<strong>in</strong> <strong>in</strong>volvement <strong>in</strong> 1/3 of patients, mostly mucosal<br />
• Heals with scarr<strong>in</strong>g (i.e. conjunctival scarr<strong>in</strong>g)<br />
• Eye <strong>in</strong>volvement may lead to bl<strong>in</strong>dness<br />
• Mucosal <strong>in</strong>volvement may lead to dysphagia or even oesophageal stenosis requir<strong>in</strong>g dilatation<br />
• (-) Nikolsky sign<br />
Histology<br />
• Subepidermal blister with mixed <strong>in</strong>flammatory cell <strong>in</strong>filtration<br />
IF - see table 1<br />
In addition, antiepiligr<strong>in</strong> cicatricial pemphigoid circulat<strong>in</strong>g autoantibodies b<strong>in</strong>d to dermal side of salt-split<br />
sk<strong>in</strong><br />
Management<br />
• Topical steroids or systemic corticosteroids +/- other immunosuppressives<br />
• Tetracycl<strong>in</strong>e +/- Nicot<strong>in</strong>amide, Azathiopr<strong>in</strong>e, Mycophenolate mofetil, Methotrexate, Cyclophosphamide<br />
Course <strong>and</strong> prognosis<br />
• Chronic, progressive<br />
Pemphigoid Gestationis (Herpes gestationis)<br />
Cl<strong>in</strong>ical<br />
• Rare, autoimmune disease of pregnancy<br />
• Extremely pruritic, polymorphic bullous dermatosis with urticarial plaques<br />
• Usually starts on the abdomen spread<strong>in</strong>g peripherally spar<strong>in</strong>g the face, palms, soles, mucous membranes<br />
• Exacerbations after delivery common<br />
• Babies born to these mothers may have transient blister<strong>in</strong>g after delivery<br />
• Heals with scarr<strong>in</strong>g (i.e. conjunctival scarr<strong>in</strong>g)<br />
Histology<br />
• Subepidermal blister with eos<strong>in</strong>ophilic <strong>in</strong>filtration<br />
IF - see table 1<br />
33
Management<br />
• Topical steroids or systemic corticosteroids if required<br />
Course <strong>and</strong> prognosis<br />
• Maternal mortality rate is unaffected<br />
• Regresses without scarr<strong>in</strong>g a few days to weeks after delivery<br />
• May recur <strong>in</strong> subsequent pregnancies<br />
L<strong>in</strong>ear IgA Disease (Chronic Bullous Disease of Childhood)<br />
Cl<strong>in</strong>ical<br />
• Often <strong>in</strong> patients > 30 years;
• Subepidermal blister at level of lam<strong>in</strong>a lucida<br />
• Neutrophilic microabscesses <strong>in</strong> dermal papillae<br />
IF - see table 1<br />
Management<br />
• Dapsone or sulfapyrid<strong>in</strong>e<br />
• Gluten-free diet<br />
• Avoid iod<strong>in</strong>e <strong>and</strong> NSAIDs<br />
Course <strong>and</strong> prognosis<br />
• Persists <strong>in</strong>def<strong>in</strong>itely<br />
• Waxes <strong>and</strong> wanes<br />
References<br />
1. Fassihi H, Wong T, Wessagowit V et al. Target prote<strong>in</strong>s <strong>in</strong> <strong>in</strong>herited <strong>and</strong> acquired blister<strong>in</strong>g sk<strong>in</strong> disorders. Cl<strong>in</strong>ical<br />
<strong>and</strong> Experimental Dermatology 2006; 31: 252-259.<br />
2. Herne KL, Jordon RE, Hsu S. Autoimmune bullous <strong>diseases</strong>. In: Ali A ed. Dermatology: A Pictorial Review. Ch<strong>in</strong>a:<br />
The McGraw-Hill Companies, 2007: 139-151.<br />
3. Saha M, Harman K, Mortimer NJ et al.<strong>Pemphigus</strong> vulgaris <strong>in</strong> white Europeans is l<strong>in</strong>ked with HLA Class II Allele<br />
HLA DRB1*1454 but Not DRB1*1401 Journal of Investigative Dermatology 2010; 130: 311–314.<br />
35