Leveling the curve of Spee with a continuous archwire technique: A ...
Leveling the curve of Spee with a continuous archwire technique: A ...
Leveling the curve of Spee with a continuous archwire technique: A ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
ORIGINAL ARTICLE<br />
<strong>Leveling</strong> <strong>the</strong> <strong>curve</strong> <strong>of</strong> <strong>Spee</strong> <strong>with</strong> a <strong>continuous</strong><br />
<strong>archwire</strong> <strong>technique</strong>: A long term<br />
cephalometric study<br />
Rael L. Bernstein, a Charles B. Preston, b and Judith Lampasso c<br />
Buffalo, NY<br />
Introduction: The orthodontic <strong>technique</strong> favored by a clinician frequently determines how a deep <strong>curve</strong> <strong>of</strong><br />
<strong>Spee</strong> (COS) is leveled. The primary purpose <strong>of</strong> this investigation was to confirm radiographically <strong>the</strong><br />
long-term effectiveness <strong>of</strong> a <strong>continuous</strong> <strong>archwire</strong> <strong>technique</strong>—<strong>the</strong> Alexander discipline—in leveling <strong>the</strong> COS<br />
in patients <strong>with</strong> Class II Division 1 deep-bite malocclusions treated <strong>with</strong>out extractions. Methods: The sample<br />
for this retrospective cephalometric study consisted <strong>of</strong> <strong>the</strong> randomly selected orthodontic records <strong>of</strong> 31 subjects<br />
(22 female, 9 male) treated <strong>with</strong> <strong>the</strong> <strong>continuous</strong> <strong>archwire</strong> <strong>technique</strong> in <strong>the</strong> private practice <strong>of</strong> Dr R.G. “Wick”<br />
Alexander in Arlington, Texas. Results: The mean pretreatment COS for this sample was 2.47 mm, and <strong>the</strong><br />
corresponding mean posttreatment COS was 0.19 mm. The COS was completely level in 21 patients after<br />
treatment, and <strong>the</strong> rest had slight residual COS at <strong>the</strong> end <strong>of</strong> this phase. Ten <strong>of</strong> <strong>the</strong> 31 subjects remained level<br />
from 5 to 25 years after orthodontic treatment. Conclusions: The results indicate that most leveling was<br />
accomplished by <strong>the</strong> extrusion <strong>of</strong> <strong>the</strong> premolars. The <strong>continuous</strong> <strong>archwire</strong> <strong>technique</strong> is effective in leveling <strong>the</strong><br />
COS in patients <strong>with</strong> Class II Division 1 deep-bite malocclusions treated <strong>with</strong>out extractions when <strong>the</strong> initial COS<br />
is 2 to 4 mm. The leveling <strong>of</strong> <strong>the</strong> COS <strong>with</strong> <strong>the</strong> <strong>continuous</strong> <strong>archwire</strong> <strong>technique</strong> takes place by a combination <strong>of</strong><br />
premolar extrusion and, to a lesser extent, incisor intrusion. (Am J Orthod Dent<strong>of</strong>acial Orthop 2007;131:363-71)<br />
The need to correct an accentuated <strong>curve</strong> <strong>of</strong> <strong>Spee</strong><br />
(COS) that is commonly encountered in a malocclusion<br />
characterized by a deep bite presents<br />
diagnostic and <strong>the</strong>rapeutic challenges for <strong>the</strong> orthodontist.<br />
1,2 Unfortunately, <strong>the</strong> orthodontic <strong>technique</strong> favored<br />
by each clinician, ra<strong>the</strong>r than <strong>the</strong> nature <strong>of</strong> a specific<br />
malocclusion, will frequently determine how deep bites<br />
are corrected. There is some disagreement among <strong>the</strong><br />
proponents <strong>of</strong> <strong>the</strong> various orthodontic <strong>technique</strong>s as to<br />
what mechanical approach is <strong>the</strong> most suitable to level<br />
an exaggerated COS.<br />
3-5 Clinicians who follow a segmented<br />
wire approach to arch leveling suggest that<br />
leveling <strong>with</strong> <strong>continuous</strong> <strong>archwire</strong>s will extrude <strong>the</strong><br />
posterior teeth, which, in turn, will result in increased<br />
lower facial height.<br />
3-7 They also believe that, in patients<br />
<strong>with</strong> strong muscles <strong>of</strong> mastication, <strong>the</strong> extrusion <strong>of</strong> <strong>the</strong><br />
buccal segments will tend to relapse after orthodontic<br />
treatment. Fur<strong>the</strong>rmore, <strong>the</strong>se clinicians believe that<br />
placing a reverse COS in a <strong>continuous</strong> <strong>archwire</strong> for arch<br />
a Private practice, Calif.<br />
b Pr<strong>of</strong>essor and chair, School <strong>of</strong> Dental Medicine, University at Buffalo.<br />
c Assistant pr<strong>of</strong>essor, School <strong>of</strong> Dental Medicine, University at Buffalo.<br />
Reprint requests to: Charles B. Preston, School <strong>of</strong> Dental Medicine, State<br />
University <strong>of</strong> New York at Buffalo, 140 Squire Hall, 3435 Main St, Buffalo,<br />
NY 14214; e-mail, cbp@buffalo.edu<br />
Submitted, February 2005; revised and accepted, May 2005.<br />
0889-5406/$32.00<br />
Copyright © 2007 by <strong>the</strong> American Association <strong>of</strong> Orthodontists.<br />
doi:10.1016/j.ajodo.2005.05.056<br />
leveling will almost always flare <strong>the</strong> mandibular incisors<br />
labially. 8,9 On <strong>the</strong> o<strong>the</strong>r hand, proponents <strong>of</strong> <strong>the</strong><br />
<strong>continuous</strong>-arch treatment philosophy contend that premolar<br />
and molar extrusions represent stable occlusal<br />
changes, whereas mandidular incisor intrusion is an<br />
unstable movement that will almost certainly relapse in<br />
time. 6,7,10-16<br />
Cephalometric studies undertaken to compare <strong>the</strong><br />
sectional and <strong>continuous</strong> arch leveling methods report<br />
that both <strong>the</strong> Ricketts<br />
4 and <strong>the</strong> modified Tweed<br />
5 <strong>technique</strong>s<br />
successfully correct deep overbites. At <strong>the</strong> same<br />
time, a comparative study <strong>of</strong> <strong>the</strong>se 2 approaches to<br />
orthodontic treatment found that <strong>the</strong>y result in similar<br />
mandibular incisor positions.<br />
17<br />
In support <strong>of</strong> <strong>the</strong> contention that it is important to<br />
18<br />
level an excessive COS, Andrews noted that <strong>the</strong><br />
occlusal planes <strong>of</strong> nonorthodontically treated normal<br />
occlusions tend to be level. He associated a COS <strong>with</strong><br />
postorthodontic treatment relapse and concluded that,<br />
even though not all normal occlusions have flat planes<br />
<strong>of</strong> occlusion, this should be an orthodontic treatment<br />
goal. Because <strong>of</strong> <strong>the</strong> tendency for <strong>the</strong> COS to return<br />
after orthodontic treatment, o<strong>the</strong>r authors in support <strong>of</strong><br />
Andrews’ point <strong>of</strong> view suggest that it should be an aim<br />
<strong>of</strong> orthodontic treatment to establish a level occlusal<br />
plane. 19,20<br />
Several authors commented on <strong>the</strong> amount and<br />
363
364 Bernstein, Preston, and Lampasso<br />
Table I. Sample (n 31; 9 male, 22 female) and time<br />
characteristics<br />
Characteristic Time<br />
Mean age at T1 12 y6mo<br />
Mean age at T2 14 y 11 mo<br />
Mean age at T3 26 y4mo<br />
Mean treatment time (T2-T1) 2y5mo<br />
Mean fixed retention time 3y4mo<br />
Mean postretention time (T3-T2) 11 y5mo<br />
type <strong>of</strong> occlusal relapse after orthodontic treatment.<br />
3,12,17,21-30 In general, <strong>the</strong>se studies noted - in<br />
creases in overjet, overbite, and mandibular incisor<br />
crowding along <strong>with</strong> decreases in arch length and arch<br />
width. Although postorthodontic relapse was studied in<br />
some detail, relatively little is known about <strong>the</strong> longterm<br />
stability <strong>of</strong> leveling <strong>the</strong> COS and how <strong>the</strong> different<br />
methods <strong>of</strong> arch leveling relate to its subsequent relapse.<br />
The primary purpose <strong>of</strong> this investigation was to<br />
determine radiographically <strong>the</strong> long-term effectiveness<br />
<strong>of</strong> <strong>the</strong> Alexander discipline (<strong>continuous</strong> <strong>archwire</strong> <strong>technique</strong>)<br />
in leveling <strong>the</strong> COS in Class II Division 1<br />
deep-bite nonextraction patients. We also report on<br />
some relevant cephalometric changes that take place<br />
during arch leveling <strong>with</strong> <strong>the</strong> <strong>continuous</strong> <strong>archwire</strong><br />
<strong>technique</strong>. The cephalometric data obtained were used<br />
to determine whe<strong>the</strong>r a COS that was leveled remains<br />
stable in <strong>the</strong> long term.<br />
MATERIAL AND METHODS<br />
The sample for this retrospective study consisted <strong>of</strong><br />
<strong>the</strong> randomly selected orthodontic records <strong>of</strong> 31 white<br />
patients treated <strong>with</strong>out extractions in <strong>the</strong> private practice<br />
<strong>of</strong> Dr R.G. “Wick” Alexander in Arlington, Texas<br />
(Table I). These patients all met <strong>the</strong> following criteria<br />
for selection: <strong>the</strong>y had Class II (ANB angle 4°)<br />
skeletal patterns, at least half-step Class II molar dental<br />
relationships, incisor overbites <strong>of</strong> 50% or greater as<br />
measured on <strong>the</strong> initial (T1) study models, and angles<br />
between <strong>the</strong> mandibular plane (MP) (Go-Gn) and <strong>the</strong><br />
sella-nasion (S-N) line less than 32°. A COS equal to or<br />
deeper than 2 mm was present on all T1 models.<br />
Only patients <strong>with</strong> complete clinical records were<br />
included in this study. These records consisted <strong>of</strong><br />
radiographs and dental casts taken at T1, posttreatment<br />
(T2), and postretention (T3). All patients were retained<br />
<strong>with</strong> lower fixed canine-to-canine lingual retainers for a<br />
mean period <strong>of</strong> 3 years 4 months. The patients were all<br />
treated <strong>with</strong> fully preadjusted fixed orthodontic appliances<br />
according to <strong>the</strong> <strong>continuous</strong> <strong>archwire</strong> <strong>technique</strong>.<br />
We selected this <strong>technique</strong> for this study because <strong>of</strong> its<br />
American Journal <strong>of</strong> Orthodontics and Dent<strong>of</strong>acial Orthopedics<br />
March 2007<br />
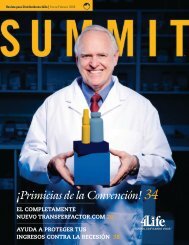
Fig 1. Cephalometric landmarks and lines.<br />
biomechanical principles that aim to provide a level<br />
occlusal plane (OP) during and at <strong>the</strong> end <strong>of</strong> active<br />
treatment. 31<br />
Three radiographs (T1, T2, T3) were collected for<br />
each subject. The 93 radiographs were assigned random<br />
numbers to enable 1 investigator (R.L.B.) to measure<br />
each in a random, blind fashion.<br />
All radiographs were taken on a Quint Sectograph<br />
machine (Los Angeles, Calif) and were hand traced by<br />
1 operator (R.L.B.) from <strong>the</strong> original radiographs.<br />
Standard cephalometric landmarks (S, N, ANS, PNS,<br />
A, B, Go, Gn) were used to construct <strong>the</strong> reference lines<br />
required to obtain <strong>the</strong> crani<strong>of</strong>acial measurements re-<br />
32<br />
corded in this study (Fig 1). The functional OP was<br />
defined by a line intersecting <strong>the</strong> intercuspation <strong>of</strong> <strong>the</strong><br />
posterior occlusion (Fig 2).<br />
33 The following additional<br />
reference points and planes were used to measure <strong>the</strong><br />
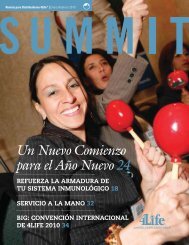
COS; <strong>the</strong>se form <strong>the</strong> focus <strong>of</strong> this study (Figs 1 and 2):<br />
I1, <strong>the</strong> incisal tip <strong>of</strong> <strong>the</strong> most extruded mandibular<br />
incisor; L6, <strong>the</strong> highest cusp tip <strong>of</strong> <strong>the</strong> mandibular<br />
permanent first molar; L1-MP, tip <strong>of</strong> <strong>the</strong> L1 perpendicular<br />
to Go-Gn; L6-MP, mesial cusp tip <strong>of</strong> <strong>the</strong> L6<br />
perpendicular to Go-Gn; L4-MP, <strong>the</strong> cusp tip <strong>of</strong> <strong>the</strong> L4<br />
perpendicular to Go-Gn; COS line, <strong>the</strong> line joining <strong>the</strong>
American Journal <strong>of</strong> Orthodontics and Dent<strong>of</strong>acial Orthopedics<br />
Volume 131, Number 3<br />
Fig 2. COS and lower dental height measurements.<br />
highest cusp tip <strong>of</strong> <strong>the</strong> L6 to <strong>the</strong> tip <strong>of</strong> <strong>the</strong> most extruded<br />
mandibular incisor (L1) 34 ; and COS, <strong>the</strong> depth <strong>of</strong> <strong>the</strong><br />
COS measured as <strong>the</strong> perpendicular distance from <strong>the</strong><br />
tooth cusp <strong>of</strong> <strong>the</strong> most infra-erupted premolar to <strong>the</strong><br />
COS line.<br />
The premolar used in measuring <strong>the</strong> deepest part <strong>of</strong><br />
<strong>the</strong> COS had to be in occlusal contact <strong>with</strong> an opposing<br />
tooth in <strong>the</strong> maxillary dentition. Because no patients<br />
in this study had <strong>the</strong>ir second molars fully erupted at<br />
T1, <strong>the</strong> COS was measured to <strong>the</strong> first molars only.<br />
Each COS was measured from <strong>the</strong> radiographic tracings<br />
by using a commercially available 0.5-mm scale<br />
ruler. Because <strong>the</strong> cephalometric radiographic scans<br />
taken on <strong>the</strong> Quint Sectograph were adjusted to focus<br />
primarily on <strong>the</strong> left half <strong>of</strong> <strong>the</strong> face, only <strong>the</strong> depth <strong>of</strong><br />
<strong>the</strong> COS on <strong>the</strong> left side could be determined accurately.<br />
The arch leveling was measured by <strong>the</strong> changes<br />
in <strong>the</strong> measurements <strong>of</strong> <strong>the</strong> distances <strong>of</strong> L1, L4, and L6<br />
to <strong>the</strong> MP (Go-Gn).<br />
The size <strong>of</strong> <strong>the</strong> combined method error in locating,<br />
superimposing, and measuring <strong>the</strong> changes <strong>of</strong> <strong>the</strong> various<br />
landmarks was calculated. Thirty radiographs (10<br />
subjects) were randomly selected from <strong>the</strong> original<br />
sample and remeasured by <strong>the</strong> same operator 2 weeks<br />
later, <strong>with</strong>out reference to <strong>the</strong> previous measurements.<br />
The casual error was calculated according to Dahlberg’s<br />
formula 35 :S 2 d2/2n, where S 2 is <strong>the</strong> error<br />
variance and d is <strong>the</strong> difference between <strong>the</strong> 2 determinations<br />
<strong>of</strong> <strong>the</strong> same variable, and <strong>the</strong> systematic error<br />
was calculated <strong>with</strong> paired t tests. A significance level<br />
<strong>of</strong> 1% was used for this part <strong>of</strong> <strong>the</strong> study.<br />
The results achieved for <strong>the</strong> COS measurements<br />
from an earlier study were compared statistically <strong>with</strong><br />
Bernstein, Preston, and Lampasso 365<br />
21<br />
paired t tests <strong>with</strong> those we obtained. These 2 sets <strong>of</strong><br />
data were recorded independently at different times and<br />
in a random, blind fashion. The same sample group was<br />
used in both studies, and <strong>the</strong> respective study models<br />
and radiographs were obtained at <strong>the</strong> same time.<br />
Because on average all patients in <strong>the</strong> sample were<br />
still undergoing active skeletal growth during and after<br />
<strong>the</strong> treatment period, <strong>the</strong> growth <strong>of</strong> <strong>the</strong> mandible<br />
probably had some effect on <strong>the</strong> observed changes in<br />
<strong>the</strong> linear measurements. Sex-based growth charts <strong>of</strong><br />
untreated normal patients in <strong>the</strong> same age and time<br />
period showed that, in our sample, <strong>the</strong> COS measurements<br />
could have been affected by appositional bone<br />
growth in <strong>the</strong> mandibular incisor, premolar, and molar<br />
regions. To calculate net mean dental movement, <strong>the</strong><br />
appropriate mean growth increments were added to <strong>the</strong><br />
affected dimensions. 36 The limitations inherent <strong>with</strong><br />
using historical data, as was done here, must, however,<br />
be kept in mind.<br />
37<br />
RESULTS<br />
The casual errors determined in this study did not<br />
exceed 0.5 mm or 0.5°, and no variable had<br />
statistically significant (P .01) systematic errors. Indications<br />
<strong>of</strong> nonnormality <strong>of</strong> <strong>the</strong> data at T1 (Dn <br />
0.2336, Lilliefors P .001) and T2 (Dn 0.4182,<br />
Lilliefors P .001) reflect <strong>the</strong> high number <strong>of</strong> repeats<br />
in <strong>the</strong> measurements (eg, 12 twos at T1 and 21 zeros at<br />
T2). Because <strong>the</strong> sample size was greater than 30, <strong>the</strong><br />
results <strong>of</strong> <strong>the</strong> t tests can, however, be considered<br />
acceptably accurate.<br />
There were no statistically significant differences<br />
(P .01) between <strong>the</strong> pairs <strong>of</strong> COS measurements (radiographic<br />
vs study model<br />
21 ) for any <strong>of</strong> <strong>the</strong> 31 patients<br />
studied at T1, T2, and T3. The cephalometric data<br />
measured from <strong>the</strong> sample <strong>of</strong> radiographs are given in<br />
Tables II and III. Paired t tests were conducted for <strong>the</strong>se<br />
measurements, and <strong>the</strong> statistical findings are shown in<br />
Table IV.<br />
The mean reduction in <strong>the</strong> ANB angle as a result <strong>of</strong><br />
treatment (T2-T1) was 2.98° (SD, 1.55°) (P <br />
.0001); this is equivalent to a 57.75% decrease in <strong>the</strong><br />
size <strong>of</strong> this angle. The overall (T3-T1) mean reduction<br />
<strong>of</strong> <strong>the</strong> ANB angle was 3.16° (SD, 2.34°).<br />
The mean Y-axis change associated <strong>with</strong> treatment<br />
was a clockwise rotation <strong>of</strong> 1.05° (SD, 1.34°)<br />
(P .0001). After treatment, this angle became more<br />
acute by a mean <strong>of</strong> 0.34° (Table II), producing an<br />
overall (T3-T1) mean opening rotation <strong>of</strong> <strong>the</strong> Y-axis<br />
angle <strong>of</strong> 0.71° (SD, 1.73°).<br />
Associated <strong>with</strong> treatment (T2-T1), <strong>the</strong> SN-OP<br />
angle showed a mean reduction <strong>of</strong> 2.98° (SD, <br />
3.09°), whereas <strong>the</strong> mean treatment change in <strong>the</strong>
366 Bernstein, Preston, and Lampasso<br />
Table II. Changes in cephalometric measurements from T1 to T3<br />
Measurement<br />
T1 T2 T3<br />
Mean SD Mean SD Mean SD<br />
L4-COS line (mm) 2.47 0.69 0.19 0.31 0.69 0.64<br />
L1-MP perp (mm) 38.89 3.02 39.42 2.94 41.08 3.27<br />
L4-MP perp (mm) 32.50 2.76 35.31 3.01 36.31 3.18<br />
L6-MP perp (mm) 29.16 2.14 31.47 2.81 32.70 3.20<br />
L1-MP (°) 94.85 5.43 95.68 6.93 94.50 5.80<br />
L1 to A-Po (mm) 1.18 1.98 0.34 1.51 0.24 2.04<br />
L1-NB (°) 22.81 5.16 24.18 4.82 23.15 4.94<br />
SNA angle (°) 82.03 3.33 79.39 4.08 79.76 4.14<br />
SNB angle (°) 76.87 3.34 77.21 3.75 77.76 3.91<br />
ANB angle (°) 5.16 1.60 2.18 1.76 2.00 2.25<br />
Y-axis (°) 66.21 2.91 67.26 3.36 66.92 3.77<br />
SN-MP (°) 31.23 4.35 32.21 5.54 31.65 6.30<br />
SN-OP (°) 17.76 3.31 14.77 2.94 14.58 3.63<br />
OP-MP (°) 13.47 3.18 17.44 4.58 17.06 4.23<br />
SN-PP (°) 8.00 2.89 8.95 3.35 8.23 3.04<br />
U6-PP perp (mm) 20.00 4.15 22.73 2.52 23.97 2.84<br />
U6-PP (°) 78.89 6.29 81.00 6.24 83.11 6.27<br />
U1-PP perp 26.29 2.46 26.87 2.84 28.29 3.10<br />
U1-PP (°) 109.24 9.31 111.23 5.30 111.97 7.87<br />
U1-NA (°) 19.18 8.27 22.68 4.25 23.68 5.74<br />
U1-L1 (°) 134.27 13.56 130.53 7.02 131.35 7.98<br />
L6-MP (°) 84.95 4.10 78.53 5.60 80.40 6.05<br />
Perp, Perpendicular.<br />
American Journal <strong>of</strong> Orthodontics and Dent<strong>of</strong>acial Orthopedics<br />
March 2007<br />
OP-MP angle was 3.90° (SD, 3.83). Both changes molar (L6), <strong>the</strong> most infra-occluded premolar (L4), and<br />
were statistically significant (P .0001).<br />
<strong>the</strong> most extruded incisor (L1) were measured <strong>with</strong><br />
According to <strong>the</strong> literature, angular changes <strong>of</strong> less reference to <strong>the</strong> mandibular plane. Since appositional<br />
than 10° in <strong>the</strong> long axes <strong>of</strong> <strong>the</strong> teeth do not have a bony growth at <strong>the</strong> inferior border <strong>of</strong> <strong>the</strong> mandible can<br />
significant effect on <strong>the</strong> perpendicular linear measure-<br />
38<br />
ments made from L1, L4, or L6 to <strong>the</strong> MP. In this<br />
radiographic study, no patients had angular changes<br />
greater than 10° for any teeth in question (Table III).<br />
The mean COS at T1 for <strong>the</strong> 31 patients treated <strong>with</strong><br />
<strong>the</strong> <strong>continuous</strong> <strong>archwire</strong> <strong>technique</strong> was 2.47 mm (SD,<br />
0.69 mm; range, 2.00-4.00 mm). The mean COS at T2<br />
for this sample was 0.19 mm (SD, 0.31 mm; range,<br />
0.00-1.00 mm) (P .0001). During treatment, <strong>the</strong> mean<br />
reduction in <strong>the</strong> COS was 2.27 mm (SD, 0.77 mm),<br />
which corresponds to a 92.16% average reduction in<br />
this measurement. Twenty-one <strong>of</strong> <strong>the</strong> 31 subjects<br />
(about 67.80%) were completely level at T2, but 10 had<br />
slight residual COS at <strong>the</strong> end <strong>of</strong> this phase. The mean<br />
COS at T3 was 0.69 mm (SD, 0.64 mm; range,<br />
0.00-2.00 mm). The mean increase in <strong>the</strong> COS from T2<br />
to T3 was 0.49 mm (SD, 0.69 mm) (P .001). The<br />
overall mean time from T1 to T3 was 14 years 4<br />
add significant amounts to <strong>the</strong>se measurements, growth<br />
prediction charts for normal white American youths<br />
were used to calculate net treatment (T2-T1) and<br />
posttreatment (T3-T2) changes.<br />
months, <strong>with</strong> a range <strong>of</strong> 7 years to 28 years 8 months.<br />
Over this period, <strong>the</strong> overall effect on <strong>the</strong> COS was an<br />
average reduction <strong>of</strong> 1.78 mm, which represents a<br />
72.97% reduction.<br />
The perpendicular heights <strong>of</strong> <strong>the</strong> mandibular first<br />
36 No growth data were<br />
found for mandibular premolar heights (L4-MP); <strong>the</strong>refore,<br />
figures midway between those <strong>of</strong> <strong>the</strong> molars and<br />
36<br />
<strong>the</strong> incisors were used for comparison. Growth adjustments<br />
were made by adding <strong>the</strong> relevant mean<br />
growth increments from <strong>the</strong> growth charts to <strong>the</strong><br />
respective measurements made at T2 and T3. Paired<br />
t tests (<strong>with</strong> set at 0.01) were calculated for both<br />
<strong>the</strong> growth-adjusted and <strong>the</strong> unadjusted measurements<br />
(Table IV).<br />
Analysis <strong>of</strong> <strong>the</strong> data, unadjusted for growth, showed<br />
that <strong>the</strong>re were statistically significant changes associated<br />
<strong>with</strong> treatment for premolar (L4-MP) and first<br />
molar (L6-MP) vertical heights (P .0001). The mean<br />
treatment changes for <strong>the</strong> dental heights were 0.53 mm<br />
(SD, 1.60 mm) for L1-MP, 2.81 mm (SD, 1.69<br />
mm) for L4-MP, and 2.31 mm (SD, 2.28 mm) for<br />
L6-MP (Table III). All unadjusted posttreatment (T3-<br />
T2) t test results for <strong>the</strong> L1, L4, and L6 perpendiculars
American Journal <strong>of</strong> Orthodontics and Dent<strong>of</strong>acial Orthopedics<br />
Volume 131, Number 3<br />
Table III. Cephalometric measurements from T1 to T3<br />
Measurement<br />
Treatment changes<br />
(T1-T2)<br />
to <strong>the</strong> mandibular plane (Tables III and IV) were<br />
statistically significant (P .01).<br />
After <strong>the</strong> relevant age- and sex-related mean growth<br />
increments were added to <strong>the</strong> data, <strong>the</strong> following results<br />
Posttreatment changes<br />
(T2-T3)<br />
Total change<br />
(T1-T3)<br />
Mean SD Mean SD Mean SD<br />
L4-COS line (mm) 2.50 0.77 0.49 0.69 1.78 0.74<br />
L1-MP perp (mm) 0.53 1.60 1.66 2.30 2.19 2.37<br />
L4-MP perp (mm) 2.81 1.69 1.00 2.00 3.81 2.15<br />
L6-MP perp (mm) 2.31 2.28 1.23 2.38 3.53 2.24<br />
L1-MP perp: growth (mm) 0.87 0.66 0.21<br />
L4-MP perp: growth (mm) 1.26 0.00 1.26<br />
L6-MP perp: growth (mm) 0.61 0.23 0.84<br />
L1-MP (°) 0.82 6.08 1.18 5.21 0.35 3.91<br />
L1 to A-Po (mm) 1.51 1.57 0.10 1.31 1.41 1.57<br />
L1-NB (°) 1.37 4.81 1.03 4.21 0.34 4.35<br />
SNA angle (°) 2.65 2.17 0.37 2.23 2.27 2.51<br />
SNB angle (°) 0.34 1.29 0.55 1.34 0.89 1.58<br />
ANB angle (°) 2.98 1.55 0.18 2.06 3.16 2.34<br />
Wits (mm) 0.52 1.86 0.06 1.45 0.59 1.95<br />
Y-axis (°) 1.05 1.34 0.34 1.33 0.71 1.73<br />
SN-MP (°) 0.98 2.43 0.56 2.44 0.42 2.75<br />
SN-OP (°) 2.98 3.09 0.19 2.56 3.18 3.22<br />
OP-MP (°) 3.90 3.83 0.32 3.14 3.58 3.18<br />
SN-PP (°) 0.95 1.91 0.73 1.64 0.23 1.78<br />
U6-MP perp (mm) 2.73 2.85 1.24 1.59 3.97 2.56<br />
U6-MP (°) 2.11 5.32 2.11 5.40 4.23 5.67<br />
U1-PP perp (mm) 0.58 1.99 1.42 1.79 2.00 2.20<br />
U1-PP (°) 1.98 9.29 0.74 5.22 2.73 9.00<br />
U1-NA (°) 3.50 8.09 1.00 3.92 4.50 7.24<br />
U1-L1 (°) 3.70 11.37 0.82 6.55 2.92 10.28<br />
L6-MP (°) 6.42 3.04 1.87 4.63 4.55 5.37<br />
Perp, Perpendicular.<br />
Table IV. Paired t tests for cephalometric measurements<br />
Measurements T1 vs T2 T2 vs T3<br />
COS P .0001 P .0004<br />
L1 perp to MP P .0742 P .0004<br />
L4 perp to MP P .0001 P .0093<br />
L6 perp to MP P .0001 P .007<br />
L1 perp to MP, growth P .0052 P .0001<br />
L4 perp to MP, growth P .0001 P .0627<br />
L6 perp to MP, growth P .1482 P .0001<br />
L1 to MP P .4569 P .2181<br />
L1 to A-Po line P .0001 P .6829<br />
L1 to NB P .1227 P .1822<br />
SN-MP P .0316 P .2072<br />
Y-axis P .0001 P .1651<br />
OP-MP P .0001 P .5151<br />
SN-OP P .0001 P .6769<br />
SN-PP P .0095 P .0198<br />
ANB angle P .0001 P .6357<br />
Perp, Perpendicular.<br />
Bernstein, Preston, and Lampasso 367<br />
were recorded. The mean adjusted (T2-T1) changes for<br />
L1-MP and L4-MP (Tables III and IV) were statistically<br />
significant (P .0052). The mean treatment<br />
changes allowing for growth were –0.87 mm for<br />
L1-MP, 1.26 mm for L4-MP, and 0.61 mm for L6-MP.<br />
The negative value calculated for <strong>the</strong> incisor represents<br />
relative intrusive movement over this time period. The<br />
posttreatment (T3-T2) changes for L1-MP and L6-MP<br />
adjusted for growth were statistically significant (P <br />
.0001). The mean net posttreatment dental movements,<br />
taking growth into account, were 0.66 mm for L1-MP,<br />
0.00 mm for L4-MP, and 0.23 mm for L6-MP.<br />
At T2, <strong>the</strong> mean increase in mandibular incisor<br />
inclination to <strong>the</strong> mandibular plane was 0.82° (SD, <br />
6.08°) (Table III). The mean amount <strong>of</strong> relapse (T3-T2)<br />
was –1.18° (SD, 5.21°). A negative number represents<br />
lingual movement (uprighting) <strong>of</strong> <strong>the</strong> mandibular<br />
incisors relative to <strong>the</strong> MP. The overall effect (T3-T1)<br />
on <strong>the</strong> mandibular incisor inclination to <strong>the</strong> MP was<br />
–0.35° (SD, 3.91°).<br />
Associated <strong>with</strong> orthodontic treatment, <strong>the</strong> mandibular<br />
incisors advanced a mean distance <strong>of</strong> 1.51 mm<br />
(SD, 1.57 mm) relative to <strong>the</strong> A-Po line (Table III).
368 Bernstein, Preston, and Lampasso<br />
After treatment, <strong>the</strong> incisors retroclined a mean distance<br />
<strong>of</strong> –0.10 mm relative to <strong>the</strong> A-Po line, resulting<br />
in an overall (T3) mean proclination <strong>of</strong> 1.41 mm<br />
(SD, 1.57 mm). A negative value for <strong>the</strong> measurement<br />
represents lingual movement <strong>of</strong> <strong>the</strong> tip <strong>of</strong> <strong>the</strong> tooth.<br />
There was a statistically significant difference between<br />
<strong>the</strong> T1 and T2 measurements P ( .0001) (Table IV).<br />
American Journal <strong>of</strong> Orthodontics and Dent<strong>of</strong>acial Orthopedics<br />
March 2007<br />
leveled completely, whereas 32% had slight residual<br />
COS at T2. For <strong>the</strong> latter patients, <strong>the</strong> average amount<br />
<strong>of</strong> COS at T2 was 0.19 mm; this is probably clinically<br />
insignificant. The T2 models all showed Class I molar<br />
and canine relationships <strong>with</strong> properly finished buccal<br />
DISCUSSION<br />
It is generally accepted that, <strong>with</strong> a few notable<br />
exceptions, leveling a deep COS makes an important<br />
contribution to <strong>the</strong> success <strong>of</strong> orthodontic treatment.<br />
18-20,34,39-43 In a study that compared sectional<br />
and <strong>continuous</strong> <strong>archwire</strong> treatments <strong>of</strong> adolescent patients<br />
<strong>with</strong> Class II, deep-bite, low-angle malocclusions,<br />
it was found that both <strong>technique</strong>s corrected deep<br />
bites. 4,5 Although <strong>the</strong>se studies compared <strong>the</strong> effective -<br />
ness <strong>of</strong> overbite correction as measured on cephalometric<br />
x-rays, <strong>the</strong>y did not measure <strong>the</strong> COS, or <strong>the</strong><br />
effectiveness and long-term stability <strong>of</strong> leveling <strong>the</strong><br />
COS. Our study was prompted by a belief that <strong>the</strong>re<br />
was a need for a long-term, comprehensive, radiographic,<br />
and study model analysis <strong>of</strong> <strong>the</strong> effectiveness<br />
and stability <strong>of</strong> leveling <strong>the</strong> COS.<br />
Before we analyzed <strong>the</strong> data from <strong>the</strong> cephalometric<br />
investigation, <strong>the</strong> radiographic assessment <strong>of</strong> <strong>the</strong> COS<br />
performed in this investigation required validation.<br />
Integral to this process were <strong>the</strong> COS measurements<br />
21<br />
recorded by Carcara et al in <strong>the</strong>ir study model<br />
analysis <strong>of</strong> <strong>the</strong> COS in <strong>the</strong> same sample group. The 2<br />
sets <strong>of</strong> measurements were compared and analyzed to<br />
determine whe<strong>the</strong>r <strong>the</strong> method <strong>of</strong> recording <strong>the</strong> COS<br />
from lateral cephalographic x-rays produced <strong>the</strong> same<br />
results as those recorded from <strong>the</strong> study models. There<br />
were no statistically significant differences (P .01)<br />
between <strong>the</strong> radiographic and <strong>the</strong> study model COS<br />
measurements for any <strong>of</strong> <strong>the</strong> 31 patients at T1, T2, and<br />
T3. 21 occlusions and normal overjets and overbites.<br />
Results <strong>of</strong> <strong>the</strong> paired t test comparing <strong>the</strong> COS at T2<br />
<strong>with</strong> that at T3 indicated a statistically significant<br />
change (P .001) in this metrical character. The COS<br />
increased from a mean <strong>of</strong> 0.19 mm at T2 to a mean <strong>of</strong><br />
0.69 mm at T3. Thus, <strong>the</strong> COS relapsed on average 0.5<br />
0mm over a mean period <strong>of</strong> 7 years 5 months after <strong>the</strong><br />
fixed lingual canine-to-canine mandibular retainers<br />
were removed (an average <strong>of</strong> 11 years 5 months<br />
postdebond). Although <strong>the</strong> relapse in <strong>the</strong> COS might be<br />
statistically significant, it is a relatively small change,<br />
which, in turn, probably represents a normal physiologic<br />
process.<br />
The correlation percentage between <strong>the</strong> 2 meth -<br />
ods was approximately 97%. Only 1 patient who was<br />
measured to be level after treatment in <strong>the</strong> study model<br />
analysis was not considered level in <strong>the</strong> cephalometric<br />
analysis. Taking into account all factors that could have<br />
influenced <strong>the</strong> recordings <strong>of</strong> <strong>the</strong> COS by <strong>the</strong> 2 methods<br />
and <strong>the</strong> closeness <strong>of</strong> <strong>the</strong> results, we believe that <strong>the</strong><br />
proposed radiographic assessment <strong>of</strong> <strong>the</strong> COS is valid.<br />
The cephalometric radiographs were taken on a Quint<br />
Sectograph that was set to focus on <strong>the</strong> cranial landmarks<br />
on <strong>the</strong> left side <strong>of</strong> <strong>the</strong> face.<br />
From this study, it seems that <strong>the</strong> <strong>continuous</strong><br />
<strong>archwire</strong> <strong>technique</strong> is an effective orthodontic approach<br />
for leveling a COS in Class II Division 1 nonextraction<br />
deep-bite patients whose initial COS was 2 to 4 mm.<br />
Sixty-eight percent <strong>of</strong> <strong>the</strong> patients studied here were<br />
19-21,27 A previous study, although con -<br />
firming that <strong>the</strong> leveling <strong>of</strong> <strong>the</strong> COS is a stable<br />
treatment outcome, could not show that <strong>the</strong> amount <strong>of</strong><br />
leveling was correlated <strong>with</strong> <strong>the</strong> amount <strong>of</strong> relapse <strong>of</strong><br />
this parameter. 44 Unfortunately, those authors did not<br />
specify <strong>the</strong> treatment <strong>technique</strong> used to treat <strong>the</strong>ir<br />
patients, who had various malocclusion types. In our<br />
study, <strong>the</strong> COS tended to relapse more in subjects <strong>with</strong><br />
<strong>the</strong> deepest COS at T1. The Pearson correlation coefficient<br />
(initial COS vs posttreatment changes) was<br />
0.380 (P .0349); this was statistically significant <strong>with</strong><br />
set at 0.05 but not <strong>with</strong> set at 0.01. At least 1 o<strong>the</strong>r<br />
study confirmed our finding that <strong>the</strong> more <strong>the</strong> COS is<br />
leveled during treatment, <strong>the</strong> more it relapses after<br />
treatment. 45 That study had a relatively short mean<br />
posttreatment time <strong>of</strong> 2 years 8 months in <strong>the</strong>ir patients,<br />
who were treated <strong>with</strong> various appliances, and who had<br />
different malocclusion types. Although dental heights<br />
were recorded in <strong>the</strong> study <strong>of</strong> mixed malocclusions, no<br />
attempt was made to compensate for <strong>the</strong> affects <strong>of</strong><br />
growth on <strong>the</strong>se dimensions.<br />
The overall long-term (T3-T1) effect <strong>of</strong> orthodontic<br />
treatment <strong>with</strong> <strong>the</strong> <strong>continuous</strong> arch <strong>technique</strong> was an<br />
average <strong>of</strong> 72.97% reduction in <strong>the</strong> pretreatment COS.<br />
Ten <strong>of</strong> <strong>the</strong> 31 patients remained 100% level over a time<br />
span <strong>of</strong> 5 to 25 years after orthodontic treatment. Only<br />
5 patients had residual COS <strong>of</strong> over 1 mm, and none<br />
was deeper than 2 mm. This study indicates that relapse<br />
in <strong>the</strong> COS occurred slowly and over an extended<br />
period <strong>of</strong> time.<br />
Although <strong>the</strong>re are speculations in <strong>the</strong> literature<br />
about <strong>the</strong> contributions <strong>of</strong> various occlusal elements<br />
involved in leveling <strong>the</strong> COS, <strong>the</strong>se reports do not<br />
quantify <strong>the</strong> contributions.<br />
3,19,43-47 At <strong>the</strong> outset <strong>of</strong> this<br />
study, <strong>the</strong>re was an attempt to use a mandibular<br />
superimposition method, 48 patterned after Björk’s<br />
21
American Journal <strong>of</strong> Orthodontics and Dent<strong>of</strong>acial Orthopedics<br />
Volume 131, Number 3<br />
Bernstein, Preston, and Lampasso 369<br />
structural method, 49 to measure <strong>the</strong> treatment-induced<br />
changes in dental heights. Whereas this <strong>technique</strong> was<br />
suitable for measuring changes in <strong>the</strong> mandibular incisor<br />
region (L1-MP), it produced method errors that<br />
were unacceptably large for <strong>the</strong> o<strong>the</strong>r 2 dimensions<br />
studied (L4-MP and L6-MP).<br />
Our results indicate that most <strong>of</strong> <strong>the</strong> leveling <strong>of</strong> <strong>the</strong><br />
COS was accomplished by relative extrusion <strong>of</strong> <strong>the</strong><br />
premolars (mean, 2.81 mm) as measured by <strong>the</strong> L4-MP<br />
perpendicular distance (Table III). It is, however, likely<br />
that some <strong>of</strong> <strong>the</strong> mean increase in this dimension could<br />
be attributed to bone apposition at <strong>the</strong> inferior border <strong>of</strong><br />
<strong>the</strong> mandible. Without control growth data for Class II<br />
subjects, we decided to use <strong>the</strong> growth charts derived<br />
from normal white American youths. In support <strong>of</strong> <strong>the</strong><br />
use <strong>of</strong> normal growth data, our selection criteria favored<br />
subjects <strong>with</strong> normal to shorter-than-average<br />
lower anterior facial heights as measured by <strong>the</strong> MP to<br />
SN angle (32°). The appositional growth in <strong>the</strong><br />
premolar area was taken to be <strong>the</strong> average <strong>of</strong> <strong>the</strong><br />
available mean growth increments <strong>of</strong> <strong>the</strong> molar and<br />
incisor regions. 36 In this study, <strong>the</strong> mean contribution<br />
<strong>of</strong> growth to <strong>the</strong> L4-MP perpendicular distance was<br />
calculated as 1.55 mm.<br />
36 If this estimated growth is<br />
taken into account, <strong>the</strong>n <strong>the</strong> mean net extrusion <strong>of</strong> <strong>the</strong><br />
premolar was 1.26 mm. Likewise, taking appositional<br />
36<br />
growth (1.7 mm) into account, it can be said that<br />
during treatment <strong>the</strong> mean change in <strong>the</strong> L6-MP dis-<br />
36<br />
tance was 0.61 mm. Allowing for growth (1.4 mm)<br />
from T1 to T2, <strong>the</strong> perpendicular distance L1-MP<br />
decreased by a mean <strong>of</strong> –0.87 mm. The premolar and<br />
incisor changes were statistically significant (P .01)<br />
before and after <strong>the</strong> possible effects <strong>of</strong> growth were<br />
taken into account. These findings agree <strong>with</strong> previous<br />
studies suggesting that straight-wire <strong>technique</strong>s level<br />
<strong>the</strong> COS by a combination <strong>of</strong> premolar extrusion and<br />
incisor intrusion. 4,5,19,46 Those studies did not, how -<br />
ever, provide data to quantify <strong>the</strong> suggested tooth<br />
movements.<br />
The relapse <strong>of</strong> <strong>the</strong> COS (T3-T2), although small,<br />
was none<strong>the</strong>less statistically significant (P .01). The<br />
mean observed relapse in <strong>the</strong> COS could be attributed<br />
to changes in <strong>the</strong> relative vertical heights <strong>of</strong> 2 <strong>of</strong> <strong>the</strong><br />
dental elements that were used to define <strong>the</strong> <strong>curve</strong>.<br />
Taking posttreatment growth changes into consideration,<br />
<strong>the</strong> mandibular incisor (L1-MP) erupted a mean<br />
distance <strong>of</strong> 0.66 mm, whereas <strong>the</strong> molar erupted a mean<br />
distance <strong>of</strong> 0.23 mm after treatment. The premolar,<br />
however, had no additional mean vertical dental height<br />
change after treatment and thus had no relapse. These<br />
results confirm previous findings <strong>of</strong> a slight return <strong>of</strong><br />
<strong>the</strong> COS after treatment.<br />
19-21,27<br />
<strong>archwire</strong> mechanics.<br />
Several authors noted <strong>the</strong> effects <strong>of</strong> <strong>continuous</strong><br />
3-9 These effects include flaring <strong>of</strong><br />
<strong>the</strong> mandibular incisors, extrusion <strong>of</strong> <strong>the</strong> mandibular<br />
molars, and clockwise opening rotation <strong>of</strong> <strong>the</strong> OP.<br />
Some features <strong>of</strong> <strong>the</strong> <strong>continuous</strong> arch <strong>technique</strong>, including<br />
<strong>the</strong> –5° <strong>of</strong> torque in <strong>the</strong> mandibular incisors and <strong>the</strong><br />
–6° <strong>of</strong> distal tip in <strong>the</strong> mandibular molars, are somewhat<br />
unique to this <strong>technique</strong>. These features, along<br />
<strong>with</strong> heat-treated stainless steel <strong>archwire</strong>s <strong>with</strong> reverse<br />
COS in <strong>the</strong> mandibular arch and omega stops tied back<br />
to <strong>the</strong> molar tubes, might play a role in preventing <strong>the</strong><br />
side effects reported <strong>with</strong> o<strong>the</strong>r straight-wire <strong>technique</strong>s.<br />
3-9<br />
All subjects in this study had mild to moderate<br />
mandibular incisor crowding that, <strong>with</strong> a straight<br />
wire and a nonextraction approach to treatment,<br />
would have been aggravated by <strong>the</strong> leveling <strong>of</strong> <strong>the</strong><br />
COS. 39 Despite <strong>the</strong> incisor crowding in our sample <strong>of</strong><br />
patients, <strong>the</strong> effects <strong>of</strong> <strong>the</strong> orthodontic treatment on <strong>the</strong><br />
position <strong>of</strong> <strong>the</strong>ir mandibular incisors were minimal. The<br />
angles (L1-NB, L1-MP) were not statistically significantly<br />
changed as a result <strong>of</strong> treatment (P .01). The<br />
mean treatment change <strong>of</strong> <strong>the</strong> significantly (P .01)<br />
altered variable (L1 to A-Po) was 1.51 1.57 mm.<br />
Because <strong>the</strong> T1 average position for <strong>the</strong> L1 to A-Po was<br />
–1.18 mm, a mean proclination <strong>of</strong> 1.51 mm placed <strong>the</strong><br />
tip <strong>of</strong> <strong>the</strong> L1 ahead <strong>of</strong> <strong>the</strong> A-Po line by a mean <strong>of</strong> 0.33<br />
mm. It is thus fair to say that, in this sample, orthodontic<br />
treatment did not result in excessive flaring <strong>of</strong> <strong>the</strong><br />
mandibular incisors.<br />
Since <strong>the</strong>re was very little alteration in <strong>the</strong> measures<br />
<strong>of</strong> <strong>the</strong> mean positions <strong>of</strong> <strong>the</strong> mandibular incisors during<br />
treatment, it was expected that little posttreatment<br />
change would occur. This was indeed <strong>the</strong> case; <strong>the</strong><br />
posttreatment changes in <strong>the</strong> 3 measurements <strong>of</strong> mandibular<br />
incisor position studied here were small and not<br />
statistically significant (P .01). The L1 to A-Po<br />
distance relapsed an average <strong>of</strong> –0.10 mm to leave <strong>the</strong><br />
tip <strong>of</strong> L1 just 0.23 mm ahead <strong>of</strong> <strong>the</strong> A-Po line. Both<br />
<strong>the</strong> T2 and <strong>the</strong> T3 recordings for <strong>the</strong> L1 to A-Po<br />
distance were close to <strong>the</strong> stated ideal position <strong>of</strong> this<br />
parameter. 46 In this group <strong>of</strong> patients, it can be - con<br />
cluded that <strong>the</strong> treatment-induced average advancement<br />
<strong>of</strong> <strong>the</strong> mandibular incisor was clinically acceptable and<br />
stable in <strong>the</strong> long term.<br />
From <strong>the</strong> data, it appears that <strong>the</strong> mean treatment<br />
change (T2-T1) for <strong>the</strong> mandibular molar inclination to<br />
<strong>the</strong> mandibular plane was –6.42° (SD, 3.04°). This<br />
finding indicates that <strong>the</strong> full 6° <strong>of</strong> tip back built into<br />
<strong>the</strong> molar attachments was expressed in most patients.<br />
The additional 0.42° might have been due to <strong>the</strong> use <strong>of</strong><br />
reverse <strong>curve</strong>d <strong>archwire</strong>s that would tend to cause <strong>the</strong><br />
posterior teeth to tip back even far<strong>the</strong>r than <strong>the</strong> tip<br />
incorporated in <strong>the</strong> prescription <strong>of</strong> <strong>the</strong> appliance. This
370 Bernstein, Preston, and Lampasso<br />
second-order movement relapsed an average <strong>of</strong> 1.87°<br />
(SD, 4.63°), resulting in a mean long-term uprighting<br />
<strong>of</strong> –4.55°.<br />
A straight-wire approach to Class II orthodontic<br />
treatment requiring leveling <strong>of</strong> <strong>the</strong> COS has been<br />
associated <strong>with</strong> increases in <strong>the</strong> vertical dimensions <strong>of</strong><br />
<strong>the</strong> face. 3,5-7 An analysis <strong>of</strong> <strong>the</strong> data from this study<br />
shows that in our patients <strong>the</strong> treatment did not have a<br />
major effect on 2 measurements <strong>of</strong> lower facial height.<br />
Although <strong>the</strong> Y-axis changed statistically significantly<br />
from T1 to T2 (P .001), <strong>the</strong> mean change was only <br />
1.05°. During treatment, <strong>the</strong> MP angle (SN-MP)<br />
changed by less than a mean <strong>of</strong> 1.0° (SD, 2.43°),<br />
which was not statistically significant (P .0316).<br />
There were changes in <strong>the</strong> mean angular relationships<br />
<strong>of</strong> <strong>the</strong> OP during treatment. During treatment,<br />
<strong>the</strong>re were a mean reduction <strong>of</strong> –2.98° in <strong>the</strong> SN-OP<br />
angle and a mean increase <strong>of</strong> 3.90° in <strong>the</strong> OP-MP angle.<br />
These changes occurred during <strong>the</strong> leveling <strong>of</strong> <strong>the</strong> COS,<br />
and <strong>the</strong>y represent counterclockwise rotation in <strong>the</strong> OP.<br />
The posttreatment changes in <strong>the</strong>se 2 angles were not<br />
statistically significant (P .01).<br />
We studied only patients <strong>with</strong> Class II Division 1<br />
malocclusions <strong>with</strong> specifically defined parameters.<br />
Our results cannot be arbitrarily extrapolated to <strong>the</strong><br />
success that can be achieved <strong>with</strong> o<strong>the</strong>r categories <strong>of</strong><br />
malocclusions such as those characterized by vertical<br />
growth patterns.<br />
CONCLUSIONS<br />
1. It is feasible to determine <strong>the</strong> depth <strong>of</strong> <strong>the</strong> COS<br />
from cephalometric radiographs taken <strong>with</strong> <strong>the</strong><br />
Quint Sectograph cephalometer.<br />
2. The <strong>continuous</strong> <strong>archwire</strong> <strong>technique</strong> effectively leveled<br />
<strong>the</strong> COS in this sample <strong>of</strong> Class II Division 1<br />
deep-bite patients treated <strong>with</strong>out extractions.<br />
3. In this study, <strong>the</strong> leveling <strong>of</strong> <strong>the</strong> COS <strong>with</strong> <strong>the</strong><br />
<strong>continuous</strong> <strong>archwire</strong> <strong>technique</strong> occurred by a combination<br />
<strong>of</strong> mainly premolar extrusion and, to a<br />
lesser extent, incisor intrusion.<br />
4. In <strong>the</strong> subjects studied here, <strong>the</strong> <strong>continuous</strong> <strong>archwire</strong><br />
<strong>technique</strong> effectively controlled <strong>the</strong> mandibular<br />
incisor position during <strong>the</strong> leveling process.<br />
These results appear to be stable in <strong>the</strong> long term.<br />
6. The –6° <strong>of</strong> tip back in <strong>the</strong> molar band tipped <strong>the</strong><br />
mandibular first molar back at least that amount<br />
during treatment.<br />
7. In this study, <strong>the</strong> <strong>continuous</strong> <strong>archwire</strong> <strong>technique</strong> did<br />
not cause excessive opening rotation <strong>of</strong> <strong>the</strong> Y-axis<br />
or <strong>the</strong> MP angle.<br />
American Journal <strong>of</strong> Orthodontics and Dent<strong>of</strong>acial Orthopedics<br />
March 2007<br />
REFERENCES<br />
1. Tweed CH. Clinical orthodontics. St Louis: C. V. Mosby; 1966.<br />
p. 2-82.<br />
2. Ricketts RM. Bioprogressive <strong>the</strong>rapy as an answer to orthodontic<br />
needs. Part I. Am J Orthod 1969;70:241-68.<br />
3. Otto RL, Anholm JM, Engel GA. A comparative analysis <strong>of</strong><br />
intrusion <strong>of</strong> incisor teeth achieved in adults and children according<br />
to facial types. Am J Orthod 1980;77:437-46.<br />
4. Dake ML, Sinclair PM. A comparison <strong>of</strong> <strong>the</strong> Ricketts and<br />
Tweed-type arch leveling <strong>technique</strong>s. Am J Orthod Dent<strong>of</strong>acial<br />
Orthop 1989;95:72-8.<br />
5. Weiland FJ, Bartleon HP, Droschl H. Evaluation <strong>of</strong> <strong>continuous</strong><br />
arch and segmented arch leveling <strong>technique</strong>s in adult<br />
patients: a clinical study. Am J Orthod Dent<strong>of</strong>acial Orthop<br />
1996;110:647-52.<br />
6. Wylie WL. Overbite and vertical facial dimensions in terms <strong>of</strong><br />
muscle balance. Angle Orthod 1944;14:13-7.<br />
7. Bench RW, Gugino CF, Hilgers JJ. Bioprogressive <strong>the</strong>rapy. Part 2.<br />
J Clin Orthod 1977;11:661-82.<br />
8. Berman MS. Straight wire myths—British Journal <strong>of</strong> Orthodontics<br />
interview. Br J Orthod 1988;151:57-61.<br />
9. Woods M. A reassessment <strong>of</strong> space requirements for lower arch<br />
leveling. J Clin Orthod 1986;20:770-8.<br />
10. Merritt J. A cephalometric study <strong>of</strong> <strong>the</strong> treatment and retention <strong>of</strong><br />
deep overbite cases (<strong>the</strong>sis). Baylor: University <strong>of</strong> Texas; 1964.<br />
11. Schudy FF. The association <strong>of</strong> anatomical entities as applied to<br />
clinical orthodontics. Angle Orthod 1966;36:190-203.<br />
12. Graber TM. Orthodontics: principles and practice. 3rd ed. Philadelphia:<br />
W. B. Saunders; 1972. p. 572-608.<br />
13. Ferguson JW. Lower incisor torque: <strong>the</strong> effects <strong>of</strong> rectangular<br />
<strong>archwire</strong>s <strong>with</strong> a reverse <strong>curve</strong> <strong>of</strong> <strong>Spee</strong>. Br J Orthod 1990;17:<br />
311-5.<br />
14. Schudy FF. Cant <strong>of</strong> <strong>the</strong> occlusal plane and axial inclination <strong>of</strong><br />
teeth. Angle Orthod 1963;23:69-82.<br />
15. Schudy FF. Vertical growth versus antero-posterior growth as<br />
related to function. Angle Orthod 1964;34:756-93.<br />
16. Lett RL. Overbite correction and relapse as analyzed by some<br />
cephalometric and treatment related variables (<strong>the</strong>sis). Minneapolis:<br />
University <strong>of</strong> Minnesota; 1969.<br />
17. Ellen EK, Schneider BJ, Selke T. A comparative study <strong>of</strong><br />
anchorage in bioprogressive vs. standard edgewise treatment in<br />
Class II correction <strong>with</strong> intermaxillary elastic force. Am J Orthod<br />
Dent<strong>of</strong>acial Orthop 1998;114:430-6.<br />
18. Andrews LF. The six keys to normal occlusion. Am J Orthod<br />
1972;62:296-309.<br />
19. Koyama T. A comparative analysis <strong>of</strong> <strong>the</strong> <strong>curve</strong> <strong>of</strong> <strong>Spee</strong> (lateral<br />
aspect) before and after orthodontic treatment—<strong>with</strong> particular<br />
reference to overbite patients. J Nihon Univ Sch Dent 1979;21:<br />
25-34.<br />
20. Okeson JP. Management <strong>of</strong> temporomandibular disorders and<br />
occlusion. 5th ed. St Louis: Mosby; 2003. p. 93-146.<br />
21. Carcara S, Preston CB, Jureyda O. The relationship between <strong>the</strong><br />
<strong>curve</strong> <strong>of</strong> <strong>Spee</strong>, relapse, and <strong>the</strong> Alexander discipline. Semin<br />
Orthod 2001;7:90-9.<br />
22. Fidler BC, Årtun J, Joondeph DR, Little RM. Long-term stability<br />
<strong>of</strong> Angle Class II Division 1 malocclusions <strong>with</strong> successful<br />
occlusal results at <strong>the</strong> end <strong>of</strong> active treatment. Am J Orthod<br />
Dent<strong>of</strong>acial Orthop 1995;107:276-85.<br />
23. Williams R. Eliminating lower retention. J Clin Orthod 1985;22:<br />
342-9.<br />
24. Little RM. The irregularity index: a quantitative score <strong>of</strong> mandibular<br />
anterior teeth. Am J Orthod 1975;68:554-63.
American Journal <strong>of</strong> Orthodontics and Dent<strong>of</strong>acial Orthopedics<br />
Volume 131, Number 3<br />
25. Bishara SE, Jakobsen JR, Treder JE, Stasi M. Changes in <strong>the</strong><br />
maxillary and mandibular tooth size-arch length relationship<br />
from early adolescence to early adulthood. Am J Orthod Dent<strong>of</strong>acial<br />
Orthop 1989;95:46-59.<br />
26. Burstone CJ. The mechanics <strong>of</strong> <strong>the</strong> segmental arch <strong>technique</strong>.<br />
Angle Orthod 1966;36:99-120.<br />
27. Elms TN, Buschang PH, Alexander RG. Long-term stability <strong>of</strong><br />
Class II Division 1 nonextraction cervical face-bow <strong>the</strong>rapy: I.<br />
model analysis. Am J Orthod Dent<strong>of</strong>acial Orthop 1996;109:<br />
271-6.<br />
28. Glenn G, Sinclair PM, Alexander RG. Nonextraction orthodontic<br />
<strong>the</strong>rapy: postreatment dental and skeletal stability. Am J Orthod<br />
Dent<strong>of</strong>acial Orthop 1987;92:321-8.<br />
29. Little RM, Reidel RA, Årtun J. An evaluation <strong>of</strong> changes in<br />
mandibular anterior alignment from 10 to 20 years postretention.<br />
Am J Orthod Dent<strong>of</strong>acial Orthop 1988;93:423-8.<br />
30. Sinclair PM, Little RM. Maturation <strong>of</strong> untreated normal occlusions.<br />
Am J Orthod 1983;84:114-23.<br />
31. Alexander RG. The Alexander discipline, contemporary concepts<br />
and philosophies. Glendora, Calif: Ormco; 1986.<br />
32. Rakosi T. An atlas and manual <strong>of</strong> cephalometric radiography.<br />
Worcester, United Kingdom: Ebenezer Baylis & Son; 1982.<br />
p. 35.<br />
33. Bimler HP. Bimler cephalometric analysis. J Clin Orthod 1985;<br />
56:501-23.<br />
34. Germane N, Staggers JA, Rubenstein L, Revere JT. Arch length<br />
consideration due to <strong>the</strong> <strong>curve</strong> <strong>of</strong> <strong>Spee</strong>: a ma<strong>the</strong>matical model.<br />
Am J Orthod Dent<strong>of</strong>acial Orthop 1992;102:251-5.<br />
35. Dahlberg G. Statistical methods for medical and biological<br />
students. London: George Allen and Unwin; 1940. p. 122-32.<br />
36. Riolo ML, Moyers RE, McNamara JA Jr, Hunter WS. An atlas<br />
<strong>of</strong> crani<strong>of</strong>acial growth. Crani<strong>of</strong>acial Growth Series. Ann Arbor:<br />
Bernstein, Preston, and Lampasso 371<br />
Center for Human Growth and Development; University <strong>of</strong><br />
Michigan; 1974. p. 126-8.<br />
37. Pr<strong>of</strong>fit WR, Fields HW. Contemporary orthodontics. St Louis:<br />
Mosby; 2000. p. 242.<br />
38. Gordon JB. Lower incisor intrusion in low angle, deep bite cases<br />
(<strong>the</strong>sis). Los Angeles: University <strong>of</strong> California at Los Angeles;<br />
1977.<br />
39. Baldridge DW. <strong>Leveling</strong> <strong>the</strong> <strong>curve</strong> <strong>of</strong> <strong>Spee</strong>: its effect on<br />
mandibular archlength. J Pract Orthod 1969;64:26-41.<br />
40. Dawson P. Evaluation, diagnosis and treatment <strong>of</strong> occlusal<br />
problems. St Louis: C. V. Mosby; 1974. p. 190-205.<br />
41. Hellsing E. Increased overbite and craniomandibular disorders—a<br />
clinical approach. Am J Orthod Dent<strong>of</strong>acial Orthop<br />
1990;98:516-22.<br />
42. Wheeler RC. A textbook <strong>of</strong> dental anatomy and physiology. 2nd<br />
ed. Philadelphia: W. B. Saunders; 1950. p. 352-405.<br />
43. Braun S, Hnat WP, Johnson BE. The <strong>curve</strong> <strong>of</strong> <strong>Spee</strong> revisited.<br />
Am J Orthod Dent<strong>of</strong>acial Orthop 1996;110:206-10.<br />
44. De Praeter J, Dermaut L, Martens G, Kuijpers-Jagtman A.<br />
Long-term stability <strong>of</strong> <strong>the</strong> leveling <strong>of</strong> <strong>the</strong> <strong>curve</strong> <strong>of</strong> <strong>Spee</strong>. Am J<br />
Orthod Dent<strong>of</strong>acial Orthop 2002;121:266-72.<br />
45. Shannon KR, Nanda RS. Changes in <strong>the</strong> <strong>curve</strong> <strong>of</strong> <strong>Spee</strong> <strong>with</strong><br />
treatment and at 2 years postreatment. Am J Orthod Dent<strong>of</strong>acial<br />
Orthop 2004;125:589-96.<br />
46. Engel G, Comforth G, Damerall JM, Gordon J, Levy P, McAlpine<br />
J, et al. Treatment <strong>of</strong> deep-bite cases. Am J Orthod 1980;77:<br />
1-13.<br />
47. Williams R. The diagnostic line. Am J Orthod 1969;55:458-76.<br />
48. Al-Buraiki H, Sadowsky C, Schneider B. The effectiveness and<br />
long-term stability <strong>of</strong> overbite correction <strong>with</strong> incisor intrusion<br />
mechanics. Am J Orthod Dent<strong>of</strong>acial Orthop 2005;127:47-55.<br />
49. Björk A. Prediction <strong>of</strong> mandibular growth rotation. Am J Orthod<br />
1969;55:585-99.