HEALTH PHYSICAL FORM - Huntington University
HEALTH PHYSICAL FORM - Huntington University
HEALTH PHYSICAL FORM - Huntington University

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
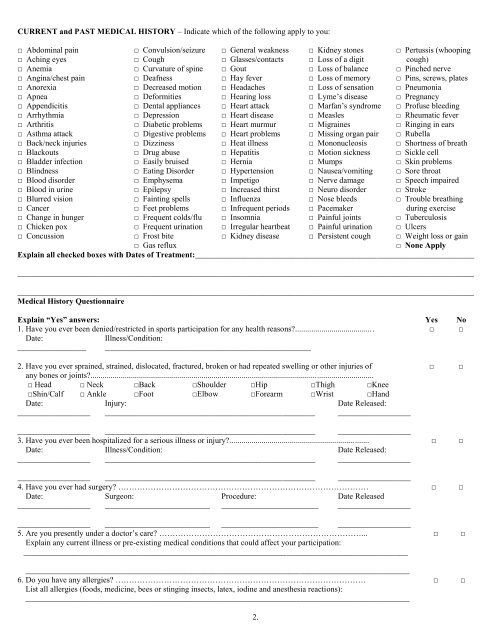
CURRENT and PAST MEDICAL HISTORY – Indicate which of the following apply to you:<br />
□ Abdominal pain □ Convulsion/seizure □ General weakness □ Kidney stones □ Pertussis (whooping<br />
□ Aching eyes □ Cough □ Glasses/contacts □ Loss of a digit cough)<br />
□ Anemia □ Curvature of spine □ Gout □ Loss of balance □ Pinched nerve<br />
□ Angina/chest pain □ Deafness □ Hay fever □ Loss of memory □ Pins, screws, plates<br />
□ Anorexia □ Decreased motion □ Headaches □ Loss of sensation □ Pneumonia<br />
□ Apnea □ Deformities □ Hearing loss □ Lyme’s disease □ Pregnancy<br />
□ Appendicitis □ Dental appliances □ Heart attack □ Marfan’s syndrome □ Profuse bleeding<br />
□ Arrhythmia □ Depression □ Heart disease □ Measles □ Rheumatic fever<br />
□ Arthritis □ Diabetic problems □ Heart murmur □ Migraines □ Ringing in ears<br />
□ Asthma attack □ Digestive problems □ Heart problems □ Missing organ pair □ Rubella<br />
□ Back/neck injuries □ Dizziness □ Heat illness □ Mononucleosis □ Shortness of breath<br />
□ Blackouts □ Drug abuse □ Hepatitis □ Motion sickness □ Sickle cell<br />
□ Bladder infection □ Easily bruised □ Hernia □ Mumps □ Skin problems<br />
□ Blindness □ Eating Disorder □ Hypertension □ Nausea/vomiting □ Sore throat<br />
□ Blood disorder □ Emphysema □ Impetigo □ Nerve damage □ Speech impaired<br />
□ Blood in urine □ Epilepsy □ Increased thirst □ Neuro disorder □ Stroke<br />
□ Blurred vision □ Fainting spells □ Influenza □ Nose bleeds □ Trouble breathing<br />
□ Cancer □ Feet problems □ Infrequent periods □ Pacemaker during exercise<br />
□ Change in hunger □ Frequent colds/flu □ Insomnia □ Painful joints □ Tuberculosis<br />
□ Chicken pox □ Frequent urination □ Irregular heartbeat □ Painful urination □ Ulcers<br />
□ Concussion □ Frost bite □ Kidney disease □ Persistent cough □ Weight loss or gain<br />
□ Gas reflux<br />
□ None Apply<br />
Explain all checked boxes with Dates of Treatment:_____________________________________________________________________<br />
_________________________________________________________________________________________________________________<br />
_________________________________________________________________________________________________________________<br />
Medical History Questionnaire<br />
Explain “Yes” answers: Yes No<br />
1. Have you ever been denied/restricted in sports participation for any health reasons?....................................... □ □<br />
Date:<br />
Illness/Condition:<br />
_________________ ___________________________________________________<br />
2. Have you ever sprained, strained, dislocated, fractured, broken or had repeated swelling or other injuries of □ □<br />
any bones or joints?............................................................................................................................................<br />
□ Head □ Neck □Back □Shoulder □Hip □Thigh □Knee<br />
□Shin/Calf □ Ankle □Foot □Elbow □Forearm □Wrist □Hand<br />
Date: Injury: Date Released:<br />
__________________ ____________________________________________________ __________________<br />
__________________ ____________________________________________________ __________________<br />
3. Have you ever been hospitalized for a serious illness or injury?..................................................................... □ □<br />
Date: Illness/Condition: Date Released:<br />
__________________ ____________________________________________________ __________________<br />
__________________ ____________________________________________________ __________________<br />
4. Have you ever had surgery? ………………………………………………………………………………… □ □<br />
Date: Surgeon: Procedure: Date Released<br />
__________________ __________________________ ________________________ __________________<br />
__________________ __________________________ ________________________ __________________<br />
5. Are you presently under a doctor’s care? …………………………………………………………………... □ □<br />
Explain any current illness or pre-existing medical conditions that could affect your participation:<br />
_______________________________________________________________________________________________<br />
_______________________________________________________________________________________________<br />
6. Do you have any allergies? ………………………………………………………………………………… □ □<br />
List all allergies (foods, medicine, bees or stinging insects, latex, iodine and anesthesia reactions):<br />
_______________________________________________________________________________________________<br />
2.