HEALTH PHYSICAL FORM - Huntington University
HEALTH PHYSICAL FORM - Huntington University
HEALTH PHYSICAL FORM - Huntington University

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
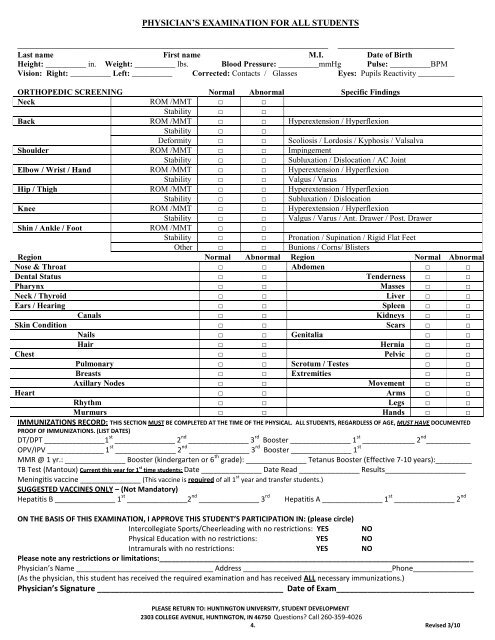
PHYSICIAN’S EXAMINATION FOR ALL STUDENTS<br />
________________________________________________________________<br />
________________________<br />
Last name First name M.I. Date of Birth<br />
Height: __________ in. Weight: __________ lbs. Blood Pressure: __________mmHg Pulse: __________BPM<br />
Vision: Right: __________ Left: __________ Corrected: Contacts / Glasses Eyes: Pupils Reactivity _________<br />
ORTHOPEDIC SCREENING Normal Abnormal Specific Findings<br />
Neck ROM /MMT □ □<br />
Stability □ □<br />
Back ROM /MMT □ □ Hyperextension / Hyperflexion<br />
Stability □ □<br />
Deformity □ □ Scoliosis / Lordosis / Kyphosis / Valsalva<br />
Shoulder ROM /MMT □ □ Impingement<br />
Stability □ □ Subluxation / Dislocation / AC Joint<br />
Elbow / Wrist / Hand ROM /MMT □ □ Hyperextension / Hyperflexion<br />
Stability □ □ Valgus / Varus<br />
Hip / Thigh ROM /MMT □ □ Hyperextension / Hyperflexion<br />
Stability □ □ Subluxation / Dislocation<br />
Knee ROM /MMT □ □ Hyperextension / Hyperflexion<br />
Stability □ □ Valgus / Varus / Ant. Drawer / Post. Drawer<br />
Shin / Ankle / Foot ROM /MMT □ □<br />
Stability □ □ Pronation / Supination / Rigid Flat Feet<br />
Other □ □ Bunions / Corns/ Blisters<br />
Region Normal Abnormal Region Normal Abnormal<br />
Nose & Throat □ □ Abdomen □ □<br />
Dental Status □ □ Tenderness □ □<br />
Pharynx □ □ Masses □ □<br />
Neck / Thyroid □ □ Liver □ □<br />
Ears / Hearing □ □ Spleen □ □<br />
Canals □ □ Kidneys □ □<br />
Skin Condition □ □ Scars □ □<br />
Nails □ □ Genitalia □ □<br />
Hair □ □ Hernia □ □<br />
Chest □ □ Pelvic □ □<br />
Pulmonary □ □ Scrotum / Testes □ □<br />
Breasts □ □ Extremities □ □<br />
Axillary Nodes □ □ Movement □ □<br />
Heart □ □ Arms □ □<br />
Rhythm □ □ Legs □ □<br />
Murmurs □ □ Hands □ □<br />
IMMUNIZATIONS RECORD: THIS SECTION MUST BE COMPLETED AT THE TIME OF THE <strong>PHYSICAL</strong>. ALL STUDENTS, REGARDLESS OF AGE, MUST HAVE DOCUMENTED<br />
PROOF OF IMMUNIZATIONS. (LIST DATES)<br />
DT/DPT _______________1 st _______________ 2 nd _______________ 3 rd Booster _______________ 1 st _____________ 2 nd ___________<br />
OPV/IPV ______________ 1 st _______________ 2 nd _______________ 3 rd Booster _______________ 1 st<br />
MMR @ 1 yr.: _______________ Booster (kindergarten or 6 th grade): _______________ Tetanus Booster (Effective 7-10 years):_________<br />
TB Test (Mantoux) Current this year for 1 st time students: Date _______________ Date Read _______________ Results____________________<br />
Meningitis vaccine _______________ (This vaccine is required of all 1 st year and transfer students.)<br />
SUGGESTED VACCINES ONLY – (Not Mandatory)<br />
Hepatitis B _______________ 1 st _______________2 nd _______________ 3 rd<br />
Hepatitis A _______________ 1 st _______________ 2 nd<br />
ON THE BASIS OF THIS EXAMINATION, I APPROVE THIS STUDENT’S PARTICIPATION IN: (please circle)<br />
Intercollegiate Sports/Cheerleading with no restrictions: YES NO<br />
Physical Education with no restrictions: YES NO<br />
Intramurals with no restrictions: YES NO<br />
Please note any restrictions or limitations:______________________________________________________________________________<br />
Physician’s Name __________________________________ Address _____________________________________Phone_______________<br />
(As the physician, this student has received the required examination and has received ALL necessary immunizations.)<br />
Physician’s Signature __________________________________________ Date of Exam_______________________________<br />
PLEASE RETURN TO: HUNTINGTON UNIVERSITY, STUDENT DEVELOPMENT<br />
2303 COLLEGE AVENUE, HUNTINGTON, IN 46750 Questions? Call 260-359-4026<br />
4. Revised 3/10