

Demonstration of the course of the posterior intercostal artery on CT ...
Demonstration of the course of the posterior intercostal artery on CT ...
Demonstration of the course of the posterior intercostal artery on CT ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
to <str<strong>on</strong>g>the</str<strong>on</strong>g> angle <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>the</str<strong>on</strong>g> rib, <str<strong>on</strong>g>the</str<strong>on</strong>g> area that approximates<br />
<str<strong>on</strong>g>the</str<strong>on</strong>g> mid-axillary line (mean<br />
deviati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> 2.3±0.366 mm; range,<br />
0–5.2 mm). There was also less variati<strong>on</strong><br />
in <str<strong>on</strong>g>the</str<strong>on</strong>g> observed distance, indicating<br />
a more c<strong>on</strong>sistent locati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>the</str<strong>on</strong>g><br />
PIA when compared to <str<strong>on</strong>g>the</str<strong>on</strong>g> PPV or <str<strong>on</strong>g>the</str<strong>on</strong>g><br />
AR (P = 0.0052) (Table 3, Fig.).<br />
Tortuosity: Tortuosity was defined<br />
subjectively <strong>on</strong> a scale <str<strong>on</strong>g>of</str<strong>on</strong>g> 0–3 (8). Over<br />
75% <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>the</str<strong>on</strong>g> PIA had ei<str<strong>on</strong>g>the</str<strong>on</strong>g>r grade 1 or 2<br />
tortuosity. Our results showed that tortuosity<br />
is highly variable, and statistical<br />
analysis showed it to be independent<br />
<str<strong>on</strong>g>of</str<strong>on</strong>g> both age (P = 0.79) and gender<br />
(P = 0.65).<br />
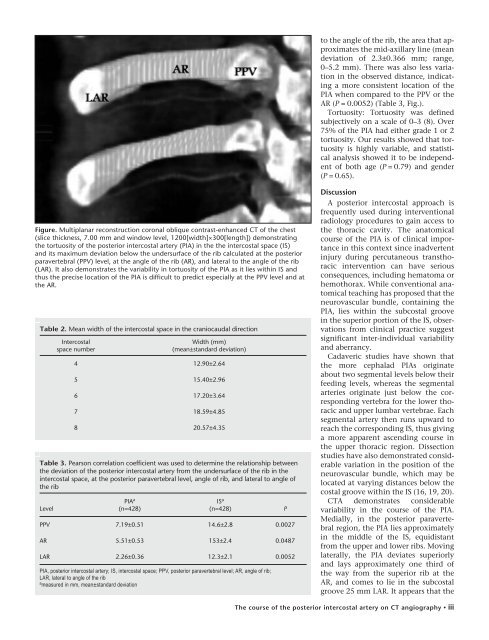
Figure. Multiplanar rec<strong>on</strong>structi<strong>on</strong> cor<strong>on</strong>al oblique c<strong>on</strong>trast-enhanced <strong>CT</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>the</str<strong>on</strong>g> chest<br />
(slice thickness, 7.00 mm and window level, 1200[width]×300[length]) dem<strong>on</strong>strating<br />
<str<strong>on</strong>g>the</str<strong>on</strong>g> tortuosity <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>the</str<strong>on</strong>g> <str<strong>on</strong>g>posterior</str<strong>on</strong>g> <str<strong>on</strong>g>intercostal</str<strong>on</strong>g> <str<strong>on</strong>g>artery</str<strong>on</strong>g> (PIA) in <str<strong>on</strong>g>the</str<strong>on</strong>g> <str<strong>on</strong>g>the</str<strong>on</strong>g> <str<strong>on</strong>g>intercostal</str<strong>on</strong>g> space (IS)<br />
and its maximum deviati<strong>on</strong> below <str<strong>on</strong>g>the</str<strong>on</strong>g> undersurface <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>the</str<strong>on</strong>g> rib calculated at <str<strong>on</strong>g>the</str<strong>on</strong>g> <str<strong>on</strong>g>posterior</str<strong>on</strong>g><br />
paravertebral (PPV) level, at <str<strong>on</strong>g>the</str<strong>on</strong>g> angle <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>the</str<strong>on</strong>g> rib (AR), and lateral to <str<strong>on</strong>g>the</str<strong>on</strong>g> angle <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>the</str<strong>on</strong>g> rib<br />
(LAR). It also dem<strong>on</strong>strates <str<strong>on</strong>g>the</str<strong>on</strong>g> variability in tortuosity <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>the</str<strong>on</strong>g> PIA as it lies within IS and<br />
thus <str<strong>on</strong>g>the</str<strong>on</strong>g> precise locati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>the</str<strong>on</strong>g> PIA is difficult to predict especially at <str<strong>on</strong>g>the</str<strong>on</strong>g> PPV level and at<br />
<str<strong>on</strong>g>the</str<strong>on</strong>g> AR.<br />
Table 2. Mean width <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>the</str<strong>on</strong>g> <str<strong>on</strong>g>intercostal</str<strong>on</strong>g> space in <str<strong>on</strong>g>the</str<strong>on</strong>g> craniocaudal directi<strong>on</strong><br />
Intercostal<br />
space number<br />
Width (mm)<br />
(mean±standard deviati<strong>on</strong>)<br />
4 12.90±2.64<br />
5 15.40±2.96<br />
6 17.20±3.64<br />
7 18.59±4.85<br />
8 20.57±4.35<br />
Table 3. Pears<strong>on</strong> correlati<strong>on</strong> coefficient was used to determine <str<strong>on</strong>g>the</str<strong>on</strong>g> relati<strong>on</strong>ship between<br />
<str<strong>on</strong>g>the</str<strong>on</strong>g> deviati<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>the</str<strong>on</strong>g> <str<strong>on</strong>g>posterior</str<strong>on</strong>g> <str<strong>on</strong>g>intercostal</str<strong>on</strong>g> <str<strong>on</strong>g>artery</str<strong>on</strong>g> from <str<strong>on</strong>g>the</str<strong>on</strong>g> undersurface <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>the</str<strong>on</strong>g> rib in <str<strong>on</strong>g>the</str<strong>on</strong>g><br />
<str<strong>on</strong>g>intercostal</str<strong>on</strong>g> space, at <str<strong>on</strong>g>the</str<strong>on</strong>g> <str<strong>on</strong>g>posterior</str<strong>on</strong>g> paravertebral level, angle <str<strong>on</strong>g>of</str<strong>on</strong>g> rib, and lateral to angle <str<strong>on</strong>g>of</str<strong>on</strong>g><br />
<str<strong>on</strong>g>the</str<strong>on</strong>g> rib<br />
Level<br />
PIA a<br />
(n=428)<br />
IS a<br />
(n=428)<br />
PPV 7.19±0.51 14.6±2.8 0.0027<br />
AR 5.51±0.53 153±2.4 0.0487<br />
LAR 2.26±0.36 12.3±2.1 0.0052<br />
PIA, <str<strong>on</strong>g>posterior</str<strong>on</strong>g> <str<strong>on</strong>g>intercostal</str<strong>on</strong>g> <str<strong>on</strong>g>artery</str<strong>on</strong>g>; IS, <str<strong>on</strong>g>intercostal</str<strong>on</strong>g> space; PPV, <str<strong>on</strong>g>posterior</str<strong>on</strong>g> paravertebral level; AR, angle <str<strong>on</strong>g>of</str<strong>on</strong>g> rib;<br />
LAR, lateral to angle <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>the</str<strong>on</strong>g> rib<br />
a measured in mm, mean±standard deviati<strong>on</strong><br />
P<br />
Discussi<strong>on</strong><br />
A <str<strong>on</strong>g>posterior</str<strong>on</strong>g> <str<strong>on</strong>g>intercostal</str<strong>on</strong>g> approach is<br />
frequently used during interventi<strong>on</strong>al<br />
radiology procedures to gain access to<br />
<str<strong>on</strong>g>the</str<strong>on</strong>g> thoracic cavity. The anatomical<br />
<str<strong>on</strong>g>course</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>the</str<strong>on</strong>g> PIA is <str<strong>on</strong>g>of</str<strong>on</strong>g> clinical importance<br />
in this c<strong>on</strong>text since inadvertent<br />
injury during percutaneous transthoracic<br />
interventi<strong>on</strong> can have serious<br />
c<strong>on</strong>sequences, including hematoma or<br />
hemothorax. While c<strong>on</strong>venti<strong>on</strong>al anatomical<br />
teaching has proposed that <str<strong>on</strong>g>the</str<strong>on</strong>g><br />
neurovascular bundle, c<strong>on</strong>taining <str<strong>on</strong>g>the</str<strong>on</strong>g><br />
PIA, lies within <str<strong>on</strong>g>the</str<strong>on</strong>g> subcostal groove<br />
in <str<strong>on</strong>g>the</str<strong>on</strong>g> superior porti<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>the</str<strong>on</strong>g> IS, observati<strong>on</strong>s<br />
from clinical practice suggest<br />
significant inter-individual variability<br />
and aberrancy.<br />
Cadaveric studies have shown that<br />
<str<strong>on</strong>g>the</str<strong>on</strong>g> more cephalad PIAs originate<br />
about two segmental levels below <str<strong>on</strong>g>the</str<strong>on</strong>g>ir<br />
feeding levels, whereas <str<strong>on</strong>g>the</str<strong>on</strong>g> segmental<br />
arteries originate just below <str<strong>on</strong>g>the</str<strong>on</strong>g> corresp<strong>on</strong>ding<br />
vertebra for <str<strong>on</strong>g>the</str<strong>on</strong>g> lower thoracic<br />
and upper lumbar vertebrae. Each<br />
segmental <str<strong>on</strong>g>artery</str<strong>on</strong>g> <str<strong>on</strong>g>the</str<strong>on</strong>g>n runs upward to<br />
reach <str<strong>on</strong>g>the</str<strong>on</strong>g> corresp<strong>on</strong>ding IS, thus giving<br />
a more apparent ascending <str<strong>on</strong>g>course</str<strong>on</strong>g> in<br />
<str<strong>on</strong>g>the</str<strong>on</strong>g> upper thoracic regi<strong>on</strong>. Dissecti<strong>on</strong><br />
studies have also dem<strong>on</strong>strated c<strong>on</strong>siderable<br />
variati<strong>on</strong> in <str<strong>on</strong>g>the</str<strong>on</strong>g> positi<strong>on</strong> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>the</str<strong>on</strong>g><br />
neurovascular bundle, which may be<br />
located at varying distances below <str<strong>on</strong>g>the</str<strong>on</strong>g><br />
costal groove within <str<strong>on</strong>g>the</str<strong>on</strong>g> IS (16, 19, 20).<br />
<strong>CT</strong>A dem<strong>on</strong>strates c<strong>on</strong>siderable<br />
variability in <str<strong>on</strong>g>the</str<strong>on</strong>g> <str<strong>on</strong>g>course</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>the</str<strong>on</strong>g> PIA.<br />
Medially, in <str<strong>on</strong>g>the</str<strong>on</strong>g> <str<strong>on</strong>g>posterior</str<strong>on</strong>g> paravertebral<br />
regi<strong>on</strong>, <str<strong>on</strong>g>the</str<strong>on</strong>g> PIA lies approximately<br />
in <str<strong>on</strong>g>the</str<strong>on</strong>g> middle <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>the</str<strong>on</strong>g> IS, equidistant<br />
from <str<strong>on</strong>g>the</str<strong>on</strong>g> upper and lower ribs. Moving<br />
laterally, <str<strong>on</strong>g>the</str<strong>on</strong>g> PIA deviates superiorly<br />
and lays approximately <strong>on</strong>e third <str<strong>on</strong>g>of</str<strong>on</strong>g><br />
<str<strong>on</strong>g>the</str<strong>on</strong>g> way from <str<strong>on</strong>g>the</str<strong>on</strong>g> superior rib at <str<strong>on</strong>g>the</str<strong>on</strong>g><br />
AR, and comes to lie in <str<strong>on</strong>g>the</str<strong>on</strong>g> subcostal<br />
groove 25 mm LAR. It appears that <str<strong>on</strong>g>the</str<strong>on</strong>g><br />
The <str<strong>on</strong>g>course</str<strong>on</strong>g> <str<strong>on</strong>g>of</str<strong>on</strong>g> <str<strong>on</strong>g>the</str<strong>on</strong>g> <str<strong>on</strong>g>posterior</str<strong>on</strong>g> <str<strong>on</strong>g>intercostal</str<strong>on</strong>g> <str<strong>on</strong>g>artery</str<strong>on</strong>g> <strong>on</strong> <strong>CT</strong> angiography • iii













