Download e-copy - Smile Dental Journal
Download e-copy - Smile Dental Journal
Download e-copy - Smile Dental Journal

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> - December 2011 - Volume 6, Issue 4 - www.smiledentaljournal.com - Distributed free of charge<br />
<strong>Dental</strong> <strong>Journal</strong><br />
Adhesion of Candida<br />
Albicans to Denture<br />
Base and Denture<br />
Liners with Different<br />
Surface Roughness<br />
An In-vitro Study<br />
Solving TMJ Problems<br />
with Orthodontic Treatment<br />
and Cosmetic Mouth<br />
Rehabilitation<br />
Case Series<br />
<strong>Dental</strong> Implants’<br />
Homepages:<br />
Are they Educative?<br />
A Cross-Sectional Study<br />
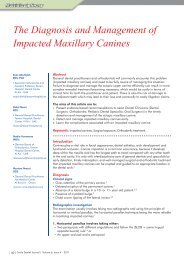
The Diagnosis and<br />
Management of<br />
Impacted<br />
Maxillary Canines<br />
Outcomes Following<br />
Zygomatic<br />
A Retrospective Study<br />
ISSN: 2072-473X
S et free your skills<br />
STERN S280 TRC INTERNAT ION AL<br />
Discover Stern S280TRc, the treatment centre built around your skills, made to merge performance<br />
and design, in an unprecedented blend of operative comfort. The suspended patient chair helps you<br />
achieve optimum posture at all times. This reduces fatigue and leads to improved concentration.<br />
The best way to express your skills and maximise interaction within the team.<br />
YOUR TALENT INSPIRES US<br />
Another good reason for choosing Stern Weber.<br />
Via Bicocca, 14/C40026 Imola (BO) Italy,<br />
Tel. 0542 653441 - Fax 0542 653601<br />
S SERIES, TR SERIES, TRC SERIES: 20 STERN WEBER ITC MODELS TO SUIT YOUR SPECIFIC NEEDS.<br />
www.sternweber.com<br />
sternweber@sternweber.com AEEDC DUBAI 31/01 – 02/02/2012 - Hall 7 Stand 412<br />
SW_<strong>Smile</strong> Mag_TRc S280_DICEMBRE2011.indd 1 17/11/11 12.00
Simplicity is the real innovation<br />
• Only one sterile NiTi instrument per root canal in most cases<br />
• Decreases the global shaping time by up to 40%*<br />
• Reciprocating technology respecting the root canal anatomy<br />
• Single use as new standard of care<br />
*data on file<br />
www.dentsplymea.com
Beauty. Versatility.<br />
Performance.<br />
IntroducIng<br />
Sultan Healthcare introduces VersaCOMP , a complete line of<br />
restorative materials that offers easy handling, versatility and<br />
clinical performance…all at a great price. The result is the<br />
ideal combination of performance and value.<br />
BEFORE<br />
AFTER<br />
VersaCOMP <br />
Universal Hybrid Composite<br />
VersaCOMP <br />
Flowable Composite<br />
VersaCOMP <br />
Universal Total Etch Adhesive<br />
411 Hackensack Avenue, 9th Floor • Hackensack, NJ 07601, USA • Phone: +1 (201)-871-1232 • Fax: +1 (201)-871-0321 • sultanhealthcare.com
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong><br />
December 2011<br />
Volume 6, Issue 4<br />
Quarterly Issued<br />
Distributed Free of Charge<br />
+962 7 96367954<br />
Amman, Jordan<br />
+961 70 32 32 75<br />
Lebanon<br />
sola@smiledentaljournal.com<br />
www.smiledentaljournal.com<br />
Director<br />
Dr. Ma’moon A. Salhab<br />
Director in Charge &<br />
Chief Editor<br />
Dr. Issa S. Bader<br />
Editorial Director<br />
Dr. Hassan A. Maghaireh<br />
Marketing Director<br />
Solange R. Sfeir<br />
Art & Design<br />
Solange R. Sfeir<br />
Cover Design<br />
Stephanie S. Moufarrej<br />
Published by MENA Co. for<br />
<strong>Dental</strong> Services<br />
Jordanian National Library<br />
Registration # 3954/2008/P<br />
ISSN 2072-473X<br />
Printed By:<br />
Ad-Dustour Commercial Printing Press<br />
Amman, Jordan<br />
Mission Statement<br />
Bridging the gap between advanced upto-date<br />
peer-reviewed dental literature and<br />
the dental practitioners enabling them to<br />
do their jobs better- is our ultimate target.<br />
Besides, <strong>Smile</strong> provides readers with<br />
information regarding the available dental<br />
products, armamentarium, news<br />
and proceedings of dental symposia,<br />
workshops and conferences.<br />
Disclaimer<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> makes every<br />
effort to report clinical information and<br />
manufacturers’ product news accurately, but<br />
cannot assume responsibility for the validity<br />
of product claims or typographical errors.<br />
Opinions or interpretations expressed by the<br />
authors are their own and do not necessarily<br />
reflect nor hold <strong>Smile</strong> team responsible for<br />
the validity of the content.<br />
Editorial Review Board<br />
• Prof. Dr. Marco Esposito / Italy<br />
DDS, PhD Implant Dentistry & Periodontics<br />
• Prof. Louis Hardan / Lebanon<br />
DDS, DEA, PhD, Restorative & Esthetic Dentistry<br />
• Dr. Maher Abdeljawad / Jordan<br />
BDS, MDentSci, Restorative Dentistry<br />
• Dr. Hani Abudiak / UK<br />
BDS, MFDS RCSFRCD, PhD Paediatric Dentistry<br />
• Dr. Eyas Abu-Hijleh / UAE<br />
DDS, PhD, Orthodontics & Dentofacial Orthopedics<br />
• Dr. Layla Abu-Naba’a / Jordan<br />
BDS, MFD, RCS, PhD, Prosthodontics<br />
• Dr. Ali Abu Nemeh / Jordan<br />
BDS, NDB, MSc, Endodontics<br />
• Dr. Hazem Al-Ahmad / Jordan<br />
BDS, MSc, FDSRCS, Maxillo-Facial Surgery<br />
• Dr. Muna Al-Ali / Australia<br />
BDS, MFDS<br />
• Dr. Suhail H. Al-Amad / UAE<br />
D.Clin.Dent (Melb), FRACDS-Oral Med, GradDip<br />
ForOdont (Melb), JMC-Oral Med<br />
• Dr. Zaid Al-Bitar / Jordan<br />
BDS, MSc, MOrth, RCS, Orthodontics<br />
• Dr. Wesam Aleid / UK<br />
BDS, MBBS, MRCSEd, FFDRCSI(OSOM), FRCS(OMFS)<br />
Oral, facial, and Head & Neck Surgeon<br />
• Dr. Raed Al-Jallad / Palestine<br />
BDS, MSc, FFDRCS, FDSRCS, Oral & Maxillofacial Surgery<br />
• Dr. Hani Al Kadi / KSA<br />
BDS, Dip ODONT, MDS, Endodontics<br />
• Dr. Alan Al-Qassab / Erbil-Iraq<br />
BDS, HDD (Ortho), MSc, MOMS RCPS(Glasg), Oral &<br />
Maxillofacial Surgery<br />
• Dr. Mohammad Al-Rabab’ah / Jordan<br />
BDS, MFD RCSIre, MRD(Pros), RCSEd, JB(Cons) PhD<br />
• Dr. Hatem Al-Rashdan/ Jordan<br />
BDS, MSc, Jordanian Board of Maxillofacial Surgery<br />
• Dr. Majd Al-Saleh / Jordan<br />
BDS, DDS, MSc, Pediatric Dentistry<br />
• Dr. Ahmad Al-Tarawneh / Jordan<br />
DDS, M.Clin.Dent, Jordanian Board of Orthodontics<br />
• Dr. Hayder Al-Waeli / Jordan<br />
BDS, MSc, Jordanian Board of Periodontology<br />
• Dr. Muayad Assaf / Jordan<br />
BDS, MSc Endodontics<br />
• Dr. Manal Azzeh / Jordan<br />
BDS, MSc, Jordanian Board of Periodontology<br />
• Dr. Lama Jarrah / Jordan<br />
BDS, MSc, Jordanian Board of Orthodontics<br />
• Dr. Ghada Karien / Jordan<br />
BDS, JDB, Pediatric Dentistry<br />
• Dr. Edgard El Chaar / USA<br />
DDS, MS. Periodontology & Implantology<br />
• Dr. Ahmad Kutkut / USA<br />
DDS, MS, Prosthodontics, USA<br />
• Dr. Yousef Sadik Marafie / Kuwait<br />
BDS, MSD, Prosthodontics<br />
• Dr. Hakam Mousa / Jordan<br />
BDS, MSD, Operative Dentistry<br />
• Dr. Jumana Sabbarini / Jordan<br />
BDS, MSc, Jordanian Board of Pediatric Dentistry<br />
• Dr. Samer Sunna / Jordan<br />
BDS, MSc, M.Orth, RCS, Orthodontics<br />
• Dr. Marwan Qasem / Palestine<br />
DDS, PG Fellowship Imlpantology<br />
• Dr. Thamer Theeb / Jordan<br />
BDS, MSc, Prosthodontics<br />
• Dr. Leema Yaghmour / Jordan<br />
BDS, DUA, DUB, Pediatric & Community Dentistry<br />
International Advisory Board<br />
• Prof. Abdullah Al-Shammery / KSA<br />
BDS, MS Restorative Dentistry / Rector, Riyadh Colleges of<br />
Dentistry & Pharmacy<br />
• Prof. Magid Amin Ahmed / Egypt<br />
Oral & Maxillo-Facial Surgery / Vice President MSA University<br />
Dean, Faculty of Dentistry MSA University<br />
• Prof. Jamal Aqrabawi / Jordan<br />
DDS, DSc, DMD Endodontics / <strong>Dental</strong> Faculty, University of Jordan<br />
• Prof. Nabil Barakat / Lebanon<br />
DDS, MSc, FICD Maxillo-Facial Surgery / President of LAO & EMAO<br />
• Prof. Stephen Cohen / USA<br />
MA, DDS, FICD, FACD, Diplomate, American Board of Endodontics<br />
• Prof. Azmi Darwazeh / Jordan<br />
BDS, MSc, PhD Oral Pathology Oral Medicine / Former Dean, Faculty<br />
of Dentistry JUST / Examiner, Faculty of Dentistry RCS Ireland<br />
• Prof. Mohamed Sherine Elattar / Egypt<br />
BDS, MSc, PhD Prosthodontics / Former Dean, Faculty of Dentistry,<br />
Pharos University / President of AOIA<br />
• Prof. Fouad Kadim / Jordan<br />
BDS, MSc, PhD Conservative Dentistry / Vice Dean, Faculty of<br />
Dentistry, University of Jordan<br />
• Prof. Howard Lieb / USA<br />
DMD General Dentistry & Management Sciences / College of<br />
Dentistry, New York University<br />
• Prof. Edward Lynch / UK<br />
PhD (Lon), MA, BDentSc, TCD, FDSRCS (Ed), FADFE, FDSRCS (Lon)<br />
Head of <strong>Dental</strong> Education and Research Warwick University<br />
• Prof. Lamis D. Rajab / Jordan<br />
DDS, PhD, Pediatric Dentistry / Former Dean, Faculty of Dentistry,<br />
University of Jordan<br />
• Prof. Issam Shaaban / Syria<br />
BDS, PhD, Maxillo-Facial Surgery / Former Dean, Faculty of<br />
Dentistry Damascus University / President of Syrian OMFS Society<br />
• Prof. Yousef Talic / KSA<br />
BDS, MSc, DASO, FICOI, FICD, Consultant in Prosthodontics &<br />
Implantology, College of Dentistry, King Saud University<br />
• Prof. Abbas Zaher / Egypt<br />
BDS, MS, PhD Orthodontics, Professor of Orthodontics / Vice-<br />
Dean, Alexandria University / Vice-President, World Federation of<br />
Orthodontists<br />
• Prof. Carina Mehanna Zogheib / Lebanon<br />
DDS, PhD Restorative and Esthetic Dentistry, FICD<br />
Head of Restorative and Esthetic Dentistry Department, Saint-<br />
Joseph University<br />
• Dr. Nadim Abou-Jaoude / Lebanon<br />
CES, DU, FICD Prosthodontics, Lecturer, Lebanese University /<br />
Clinical Associate, American University of Beirut<br />
• Dr. Hasanen H. Al-Khafagy / UAE<br />
BDS, MSc, PhD Conservative Dentistry, Ajman University of Science<br />
& Technology<br />
• Dr. Jaser Al-Ma’itah / Jordan<br />
BDS, MSc Oral Surgery, Head of <strong>Dental</strong> Department, Jordanian<br />
Royal Medical Services<br />
• Dr. Maher Almasri / UK<br />
DDS, MSc, PhD, FADFE, Director of Oral Surgery Courses, Bone<br />
Graft Modules Leader, Warwick University / President of the Syrian<br />
Section of IADR<br />
• Dr. Abdelsalam Elaskary / Egypt<br />
BDS, FICOI, President of ASOI<br />
• Dr. Yasin El-Husban / Jordan<br />
DDS, MSc Prosthodontics, Former Minister of Health<br />
Former Head of <strong>Dental</strong> Department & King Hussein Hospital<br />
• Dr. Zbys Fedorowicz / Bahrain<br />
Director, The Bahrain Branch of the UK Cochrane Centre<br />
• Dr. Wolfgang Richter / UK<br />
DDS, PhD, Restorative Dentistry, President of ESCD<br />
• Dr. Mohammad Sartawi / Jordan<br />
BSc, BDS, MSc, FFDRCSI (OSOM)<br />
Senior Consultant Maxillo-Facial Surgery
14<br />
Implantology<br />
<strong>Dental</strong> Implants’ Homepages: Are they Educative?<br />
A Cross-Sectional Study<br />
By Layla Abdel-Aziz Abu-Naba’a<br />
Orthodontics<br />
Solving TMJ Problems with Orthodontic Treatment and Cosmetic<br />
Mouth Rehabilitation: Case Series<br />
26<br />
By Leonid Rubinov<br />
32<br />
Maxillofacial<br />
Outcomes Following Zygomatic: A Retrospective Study<br />
By Majed Hani Khreisat<br />
Multidisciplinary<br />
40 The Diagnosis and Management of Impacted Maxillary Canines<br />
By Eyas Abuhijleh, Dalal Masri, Nadia Farawana, Mariam Nmari<br />
Prosthodontics<br />
Adhesion of Candida Albicans to Denture Base and Denture<br />
Liners with Different Surface Roughness: An In-vitro Study<br />
46<br />
By Zahraa Nazar Al-Wahab<br />
Debate in Focus<br />
08<br />
54<br />
60<br />
Research<br />
Summaries in<br />
Focus<br />
Endodontic or <strong>Dental</strong><br />
Implant Therapy: The<br />
Factors Affecting Treatment<br />
Planning<br />
Effect of Teeth with<br />
Periradicular Lesions on<br />
Adjacent <strong>Dental</strong> Implants<br />
The Effects of Smoking on<br />
Fracture Healing<br />
66<br />
Ask the Experts<br />
Flash News<br />
Two Minutes with<br />
78<br />
Affiliation & Distributors<br />
• Bahrain:<br />
Bahrain <strong>Dental</strong> Society +973 17723767, bahds@batelco.com.bh<br />
• Egypt:<br />
Alexandria Oral Implantology Association +203 5451277<br />
www.aoiaegypt.com<br />
• Iran:<br />
Shayan Simin Teb Co. +98 21 66380364/5, info@shayansiminteb.com<br />
Iranian General <strong>Dental</strong> Association +98 2188287794/5, info@igda.ir<br />
• Iraq:<br />
Iraqi <strong>Dental</strong> Association +964 015379267, info@iraqidental.org<br />
Kurdistan <strong>Dental</strong> Association +964 7504510315,<br />
dara_saeed@yahoo.com<br />
Pro Health Line Company +964 7504544479, www.prohealthline.com<br />
Emirates Scientific Bureau +964 771 0131978, www.prohealthline.com<br />
• Jordan:<br />
Jordanian <strong>Dental</strong> Association (JDA) +962 6 5665520, info@jda.org.jo<br />
Basamat Medical (Pharmadent) +962 6 5605395, www.basamat.com<br />
• Kuwait:<br />
Kuwait <strong>Dental</strong> Association +965 5325094, www.kda.org.kw<br />
• Lebanon:<br />
Lebanese <strong>Dental</strong> Association +961 1 611555, www.lda.org.lb<br />
Lebanese <strong>Dental</strong> Laboratory Association (OPDL) +961 5955 151<br />
www.opdlb.com<br />
Richa <strong>Dental</strong> Store +961 5 452555, www.richadental.com<br />
• Oman:<br />
Oman <strong>Dental</strong> Society +968 95769039, omandent@omantel.net.om<br />
• Palestine:<br />
Palestinian Association of Implant Dentistry (PADI)<br />
+970 2 2954545, www.implant.ps<br />
• Qatar:<br />
Qatar <strong>Dental</strong> Society +974 4393144, www.qatardentalsociety.org<br />
Ali Bin Ali Medical The i-partner +974 4867871 ext. 247<br />
www.alibinali.com<br />
• Saudi Arabia:<br />
Saudi <strong>Dental</strong> Society +966 1 4677743, www.sds.org.sa<br />
• Sudan:<br />
Sudanese <strong>Dental</strong> Association +249 83 779769, sdaassnan@hotmail.com<br />
• Syria:<br />
Najjar Trading Est. +963 (11) 2244140, najjest@scs-net.org<br />
• United Arab Emirates:<br />
Noble Medical Equipment +971 4 3255046<br />
imad.kafity@noblemedical.ae<br />
Dubai Medical Equipment L.L.C. +971 6 554 0206<br />
www.mamut-dental.com<br />
Editorial Policy<br />
• Our objective is to publish a dental journal of consistent high quality and help to increase the exposure of literature written by dental professionals from our region at a global level.<br />
• Literature review, original research, clinical case reports, case series, short communication, randomized clinical trials, and book reviews are among our scope of published<br />
material, where the clinical aspect of dentistry is presented in a scientific way, starting each article with an abstract, backed up by references in accordance with<br />
the Vancouver citation style.<br />
• The journal encourages the submission of papers with a clinical approach, practical or management oriented, besides papers that bridge the gap between dental<br />
research and clinical application.<br />
• Received manuscripts are first revised by the editor to check if it is appropriate for publishing in <strong>Smile</strong> and that it complies with the author›s guidelines. The manuscript is<br />
then forwarded to two or more professional reviewers. Anonymity of both the author and reviewer is preserved (double blinded peer-review process).<br />
• Our editorial policy which controls the quality of articles and assures their accuracy, clarity, and smooth readability through high level enthusiast regional and<br />
international team of experts is our golden key for success.<br />
• Finally, we believe that a controlled content of advertisements could be informative and beneficial especially in dentistry, where the armamentarium and pharmaceuticals<br />
are a major and integral part of the dental science.
The <strong>Smile</strong>...<br />
Past - Present - Future<br />
If we take a look at the pathway of Dentistry over the past century, we would notice that<br />
The <strong>Smile</strong> was certainly not the primary focus of the dentist`s awareness and concern until<br />
recently. <strong>Dental</strong> Aesthetics is one of the revolutions in dentistry since World War II with the<br />
others being the technology and equipment of the 1950s, the emphasis of prevention for<br />
teeth conservation in the 1960s and lately implant dentistry in the 1980s. In fact providing<br />
aesthetic dentistry to patients became an economic necessity for dentists.<br />
In 1989, while chairing the scientific committee at the Lebanese University-School of Dentistry, we organized the 1 st<br />
meeting worldwide on “The <strong>Smile</strong>” for 2 days that included the contributions of all dental and oro-facial specialties.<br />
Our editorial at the time focused not only on the relationship between health and aesthetics but stressed on the interlink<br />
established between a society of consumption constantly influenced by the mass media, a medical industry catering for<br />
marketing, a dental profession exploring new horizons and a patient constantly seeking for beauty. Such vicious circle<br />
could expose medicine to lose its nobility and with it its true identity.<br />
Today, 22 years later, our opinion has not only not changed but all our apprehension and fear of aesthetic abuses has been<br />
justified specially when considering all the disasters resulting and/or hidden behind the so called “Hollywood <strong>Smile</strong>”.<br />
Nowadays, the smile still plays a major role in communication and is considered as one of the main tools in advertising.<br />
However, are we really attracted to teeth that are falsely so white and chalky without any natural transparency or<br />
translucency and look so fake? Are we satisfied as dentists to look at magazines covers only to find smiles that all look the<br />
same, in which one size fits everybody and encourage our patients to request <strong>copy</strong>cats because it is the smile of their idols?<br />
Are we not responsible to control and guide the mass media in educating the public and spreading the correct information<br />
rather than adverts not evidence based. Finally shouldn’t we even prepare guidelines about the Ethics of Aesthetics!<br />
With such observations, Aesthetics should be revisited and we would have to pay Mother Nature more respect. Aesthetics<br />
should be viewed in term of rejuvenation with a custom made approach and some consideration to the individual<br />
characteristics. It would have to make people look younger but not cloned to such extent that they loose their personality.<br />
The smile is part of the body and not a wear that changes with years along with fashion.<br />
According to the philosopher Kant, Beauty is defined as “What Attracts Universally and Without any Concept”.<br />
Concerning the smile, we have to go back to our basics:<br />
1. The color is not the only variable in tooth aesthetics, we have to consider position, volume, texture... It is Microaesthetics<br />
2. The tooth is only one variable in the smile components that include the periodontium, lips, smile reveal... It is Macroaesthetics<br />
3. The smile is part of the Facial Harmony that involves the eyes, nose, and chin<br />
The ideal smile team would include an Orthodontist, a Periodontist and a Prosthodontist or a General Dentist in order to<br />
have a multi disciplinary approach and take the best from every specialty. A Maxillo–Facial Surgeon could be consulted in<br />
certain conditions.<br />
Taking all these data into consideration, we have to admit that the time factor plays a major role when a multidisciplinary<br />
approach is indicated for a long lasting result. This time, essential for therapy, that the patient wants to be always shorter<br />
and faster, becomes in fact the only judge for success.<br />
Finally, communication is an issue that we should not overlook if we want to meet our patients’ expectations. Since they<br />
usually pay up front for a series of procedures with an outcome they envision quite differently than we do.<br />
In such circumstances we might fall into Charles Revlon thought:<br />
“In the Factory we Make Cosmetics and in the Store we Sell… Hope”<br />
Prof. Jean-Marie Megarbane DCD, CAGS, FAIDS, FICD<br />
Masters <strong>Dental</strong> Clinic, Beirut-Lebanon<br />
info@mastersdentalclinic.com<br />
www.mastersdentalclinic.com<br />
| 4 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 34 - 2011
International Events<br />
6 - 8 February<br />
14 th King Saud University &<br />
23 rd Saudi <strong>Dental</strong> Society<br />
International <strong>Dental</strong><br />
Conference<br />
Riyadh, KSA<br />
www.sds.org.sa<br />
12 - 15 March<br />
3 rd International Conference<br />
of King Abdulaziz University<br />
Jeddah, KSA<br />
www.kau.edu.sa<br />
30 - 31 March<br />
2 nd Iraqi <strong>Dental</strong> Reunion IDR Annual<br />
Conference 2012<br />
Erbil, Iraq<br />
www.cappmea.com/idr2012<br />
3 - 4 May<br />
6<br />
th CAD/CAM &<br />
Computerized Dentistry<br />
International Conference<br />
Dubai, UAE<br />
www.cappmea.com/<br />
cadcam6<br />
3 - 5 February<br />
1 st Annual Conference of The Arabian<br />
Academy of Esthetic Dentistry<br />
Cairo, Egypt<br />
www.araed-org.com<br />
26 - 28 April<br />
Sky Meeting 2012 (AOIA)<br />
Alexandria, Egypt<br />
www.aoiaegypt.com<br />
12 - 13 April<br />
8 th Gulf <strong>Dental</strong> Association<br />
Conference & 2 nd Qatar<br />
Internationl <strong>Dental</strong><br />
Association Conference<br />
Doha, Qatar<br />
17 - 19 May<br />
7 th Lebanese <strong>Dental</strong><br />
Laboratory Seminar<br />
(LDLS)<br />
Beirut, Lebanon<br />
www.opdlb.org<br />
25 - 26 May<br />
Tarnow Alumni & Friends<br />
Venice, Italy<br />
www.tarnowalumni.com<br />
For more dental events please visit www.smiledentaljournal.com or our page on Facebook<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011| 5 |
<strong>Smile</strong> Message<br />
1 st <strong>Smile</strong> <strong>Dental</strong> Symposium; the First Step in Long Term<br />
Evidence Based <strong>Dental</strong> Program<br />
Dentistry is a continually developing science. Over the past 20 years or so there have<br />
been changes of opinion and practice: some techniques and opinions previously<br />
advocated are not so today; controversies and conflicts surrounding the practice of dentistry have arisen; and a full<br />
circle of opinions have been travelled by dentists over a period of time.<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> was proud to launch its <strong>Smile</strong> <strong>Dental</strong> Symposia with the theme of “<strong>Dental</strong> Implants: Is Quicker<br />
Always Better?”. The 1 st <strong>Smile</strong> <strong>Dental</strong> Symposium aimed to look into one of the interesting branches of dentistry; <strong>Dental</strong><br />
Implantology. The science of dental implantology is not only regarded as one of the major innovations in dentistry, but<br />
also has come a long way in a relatively short period of time.<br />
The one-day event featured a high-quality scientific program along with an up to date and advanced dental show.<br />
The majority of the delegates agreed that this symposium had provided them with evidence based and clinical tips<br />
which they can apply in their day to day dental implant practice.<br />
The symposium social event – “<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> 5 th Anniversary Gala dinner” – took place at the glamorous<br />
five star Land Mark hotel in Amman, under the patronage of the president of the Jordan <strong>Dental</strong> Association; Dr.<br />
Qadoomi. The symposium was organized in co-operation with the Scientific Committee in the Jordan <strong>Dental</strong><br />
Association and was also well supported by the dental and local private companies who have sponsored the prizes<br />
for the quiz show during the Gala dinner.<br />
This successful symposium was not the end. It is not even the beginning of the end. But it is, perhaps, the end of<br />
the beginning, as we promise the dental community in the Middle East more of these advanced and well structured<br />
dental symposia covering different dental specialties in various countries, aiming to bridge the gap between evidence<br />
based and clinical practice in the whole area.<br />
For the full symposium report and photos, please refer to the Event section.<br />
Behind the scenes we are very fortunate to have a small and dedicated team who work hard to ensure the <strong>Smile</strong><br />
<strong>Dental</strong> <strong>Journal</strong> functions smoothly. Thank you to all the directors, Dr. Mamoon Salhab Tamimi, Dr. Issa Bader and<br />
Miss. Solange Sfeir.<br />
Finally, I would like to thank all <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> reviewers, the international advisory board and our beloved<br />
readers for their support and encouragement over the last year.<br />
New Authors Guidelines are Well Received<br />
Since we have updated our authors’ guidelines for submitting manuscripts to <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> to meet the<br />
international requirements for reporting on health research are continuously evolving, we have started to receive a<br />
better quality articles from authors all around the world. We made it clear that the key point is to focus on quality<br />
rather than quantity, and I think that we are on the right track.<br />
Even better, I am now delighted to announce that we are now been recognized by a number of high standards<br />
dental schools as one of the esteemed indexed journals where staff and students can publish their studies and reports<br />
as a mean for granting promotion. If anything, this recognition is a great proof that in a short time, <strong>Smile</strong> <strong>Dental</strong><br />
<strong>Journal</strong> has managed to prove that we are a peer reviewed, evidence based dental journal which aims to improve<br />
the quality of dental care provided to dental patient in this area.<br />
While we promise to continue this thousand mile journey, we urge our readers to support us by continuing to submit<br />
high quality dental articles which are of interest to practitioners in all areas of dental practice, including general<br />
practice, community and hospital dentistry, the armed forces, corporate bodies.<br />
Dr. Hassan Maghaireh<br />
Editorial Director<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong><br />
| 6 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 14 - 2011
Colgate Total – Long-lasting protection<br />
against<br />
Colgate<br />
plaque<br />
Total –<br />
and<br />
Long-lasting<br />
gingivitis<br />
protection<br />
Colgate against plaque Total – Long-lasting and gingivitis protection<br />
against Colgate plaque Total – Long-lasting and gingivitis protection<br />
against sustained anti-bacterial plaque activity and for gingivitis<br />
12 hours<br />
Colgate 1, 2<br />
• sustained Long-lasting anti-bacterial Total protection – activity against Long-lasting plaque for 12 and hours gingivitis protection<br />
1, 2 3, 4<br />
against • Reduced Long-lasting gingival plaque protection bleeding against and 3, 4 plaque gingivitis and gingivitis 3, 4<br />
Colgate Total with unique Triclosan/Copolymer Technology provides<br />
Colgate Total with unique Triclosan/Copolymer Technology provides<br />
Colgate Total with unique Triclosan/Copolymer Technology provides<br />
sustained • Reduced anti-bacterial calculus gingival formation bleeding activity 3, 45<br />
and for oral 12 hours malodor 1, 2<br />
Colgate Total with unique Triclosan/Copolymer 3, Technology 6<br />
provides<br />
• Long-lasting Caries Reduced protection calculus protection with formation 1450 against 3, ppm 5 and plaque fluoride oral and malodor 3, 7 gingivitis 3, 6 3, 4<br />
sustained anti-bacterial activity for 12 hours 1, 2<br />
Reduced Caries protection gingival bleeding with 1450 3, 4<br />
ppm fluoride<br />
• 3, 7<br />
Colgate Long-lasting Total with protection unique against Triclosan/Copolymer plaque and gingivitis Reduced calculus formation 3, 5 Technology 3, 4<br />
and oral malodor 3, 6 provides<br />
• sustained The Reduced unique anti-bacterial gingival 3-step mechanism bleeding activity 3, 4 of for Triclosan/Copolymer<br />
12 hours Caries protection with 1450 ppm fluoride 1, 2<br />
3, 7<br />
• The Reduced Long-lasting unique calculus 3-step protection formation mechanism against 3, 5 of and plaque Triclosan/Copolymer<br />
oral and malodor gingivitis 3, 6 3, 4<br />
Adheres to both hard and soft tissues of the mouth<br />
• Caries Reduced protection gingival bleeding with 1450 3, 4 ppm fluoride 3, 7<br />
The • Reduced unique Actively Adheres<br />
calculus 3-step reduces to both mechanism formation plaque hard 3, and 5 bacteria and of soft Triclosan/Copolymer<br />
oral<br />
tissues<br />
malodor<br />
of the 3, 6 mouth<br />
• Caries Helps Actively protection prevent reduces with regrowth 1450 plaque ppm of bacteria plaque fluoridebiofilm 3, 7 for 12 hours<br />
The unique Adheres after 3-step<br />
Helps brushing prevent<br />
to both mechanism<br />
regrowth<br />
hard and of<br />
of<br />
soft Triclosan/Copolymer<br />
plaque<br />
tissues<br />
biofilm<br />
of the<br />
for<br />
mouth<br />
12 hours<br />
Actively after brushing reduces plaque bacteria<br />
The unique Adheres 3-step to both mechanism hard and of soft Triclosan/Copolymer<br />
tissues of the mouth<br />
Helps prevent regrowth of plaque biofilm for 12 hours<br />
Actively reduces plaque bacteria<br />
Adheres after brushing to both hard and soft tissues of the mouth<br />
Helps prevent regrowth of plaque biofilm for 12 hours<br />
Actively after brushing reduces plaque bacteria<br />
Helps prevent regrowth of plaque biofilm for 12 hours<br />
For after healthy brushing gums<br />
and For teeth healthy recommend gums Colgate Total<br />
and teeth recommend Colgate Total<br />
For healthy gums<br />
1 Amornchat C et al. (2004) Mahidol Dent J 24(2): 103-111<br />
2 Fine DH et al. (2006) J Am Dent Assoc 137: 1406-1413<br />
3 Panagakos and FS et al. teeth (2005) J Clin Dent recommend 16 (Suppl): S1-S20 Colgate Total<br />
4 Garcia-Godoy F et al. (1990) Am J Dent 3 (Spec Issue): S15-26<br />
5<br />
1<br />
Banoczy<br />
Amornchat<br />
J et<br />
C<br />
al.<br />
et<br />
(1995)<br />
al. (2004)<br />
Am J<br />
Mahidol<br />
Dent 8(4):<br />
Dent<br />
205-208<br />
J 24(2): 103-111<br />
6<br />
2<br />
Hu<br />
Fine<br />
D For et<br />
DH<br />
al.<br />
et<br />
(2003) healthy<br />
al. (2006)<br />
Compend<br />
J Am Dent<br />
Contin<br />
Assoc<br />
Educ<br />
137:<br />
Dent gums<br />
1406-1413<br />
24 (9 Suppl): 34-41<br />
7<br />
3<br />
Marinho<br />
Panagakos<br />
et al.<br />
FS<br />
The<br />
et al.<br />
Cochrane<br />
(2005) J<br />
Library.<br />
Clin Dent<br />
Issue<br />
16<br />
I.<br />
(Suppl):<br />
John Wiley<br />
S1-S20<br />
& Sons, 2006<br />
4 Garcia-Godoy F et al. (1990) Am J Dent 3 (Spec Issue): S15-26<br />
5 Banoczy and J et al. (1995) teeth Am J Dent 8(4): recommend 205-208 Colgate Total<br />
For healthy gums YOUR PARTNER IN ORAL HEALTH<br />
and teeth recommend Colgate Total<br />
YOUR PARTNER IN ORAL HEALTH<br />
6 Hu D et al. (2003) Compend Contin Educ Dent 24 (9 Suppl): 34-41<br />
7 Marinho et al. The Cochrane Library. Issue I. John Wiley & Sons, 2006<br />
1 Amornchat C et al. (2004) Mahidol Dent J 24(2): 103-111<br />
2 Fine DH et al. (2006) J Am Dent Assoc 137: 1406-1413<br />
3 Panagakos FS et al. (2005) J Clin Dent 16 (Suppl): S1-S20<br />
4 Garcia-Godoy F et al. (1990) Am J Dent 3 (Spec Issue): S15-26<br />
5 Banoczy J et al. (1995) Am J Dent 8(4): 205-208<br />
6 Hu D et al. (2003) Compend Contin Educ Dent 24 (9 Suppl): 34-41<br />
71 Marinho Amornchat et al. C et The al. Cochrane (2004) Mahidol Library. Dent Issue J 24(2): I. John 103-111 Wiley & Sons, 2006<br />
2 Fine DH et al. (2006) J Am Dent Assoc 137: 1406-1413<br />
3 Panagakos FS et al. (2005) J Clin Dent 16 (Suppl): S1-S20<br />
4 Garcia-Godoy F et al. (1990) Am J Dent 3 (Spec Issue): S15-26<br />
5 Banoczy J et al. (1995) Am J Dent 8(4): 205-208<br />
6 Hu D et al. (2003) Compend Contin Educ Dent 24 (9 Suppl): 34-41<br />
71 Marinho Amornchat et al. C et The al. Cochrane (2004) Mahidol Library. Dent Issue J 24(2): I. John 103-111 Wiley & Sons, 2006<br />
2 Fine DH et al. (2006) J Am Dent Assoc 137: 1406-1413<br />
3 Panagakos FS et al. (2005) J Clin Dent 16 (Suppl): S1-S20<br />
4 Garcia-Godoy F et al. (1990) Am J Dent 3 (Spec Issue): S15-26<br />
5 Banoczy J et al. (1995) Am J Dent 8(4): 205-208<br />
6 Hu D et al. (2003) Compend Contin Educ Dent 24 (9 Suppl): 34-41<br />
7 Marinho et al. The Cochrane Library. Issue I. John Wiley & Sons, 2006<br />
YOUR PARTNER IN ORAL HEALTH<br />
YOUR PARTNER IN ORAL HEALTH<br />
www.colgateprofessional.co.uk<br />
www.colgateprofessional.co.uk<br />
www.colgateprofessional.co.uk<br />
YOUR PARTNER IN ORAL HEALTH<br />
www.colgateprofessional.co.uk<br />
www.colgateprofessional.co.uk m
Neutral Zone in Complete Dentures:<br />
Systematic Analysis of Evidence and Technique<br />
• Ahmad A. Jum’ah, BDS(Hons), MSc/PhD (Clin) Student-Second year<br />
Restorative Dentistry Department, Leeds <strong>Dental</strong> Institute, University of Leeds, UK<br />
dnaahj@leeds.ac.uk<br />
• Peter J. Nixon, Senior Consultant in Restorative Dentistry, Leeds <strong>Dental</strong> Hospital,<br />
Leeds Teaching Hospitals Trust (LTHT), England, UK<br />
Abstract<br />
Neutral zone technique is a physiologic and functional approach that is widely and concisely described as a treatment<br />
modality for unstable lower complete denture cases. It serves as a guide of where to set teeth and how to contour the<br />
polished surface of the denture to ensure optimal stability, retention, facial support and aesthetics. In patients with<br />
compromised support and poor denture adaptability, this technique is considered as a valuable tool in the prosthodontist’s<br />
armoury especially where dental implants are contraindicated or unfeasible. The aim of this article is to describe the concept<br />
and technique of neutral zone, discuss rationale, indications and to evaluate this technique from evidence-based perspective.<br />
Abbreviations: NZ: Neutral zone, CD: complete denture, VDO: Vertical dimension at occlusion.<br />
Introduction<br />
Stability of lower CDs is well recognized as a potentially<br />
difficult treatment aim to achieve. Looseness and discomfort<br />
are the most frequent complaints reported by patients and<br />
they are quite often difficult to manage by dentists.<br />
Neuromuscular control is said to be the key determinant<br />
of stability of lower CD as the area available for support is<br />
far less than maxillary support area. Size and position of<br />
prosthetic teeth and the contours of polished surface have<br />
a crucial role in lower CD stability as they are subjected to<br />
destabilizing forces from the tongue, lips and cheeks if they<br />
are placed in hindrance with function of these structures. 1<br />
Throughout time, many concepts and theories emerged<br />
to describe where prosthetic teeth of CD should<br />
be positioned. Some of them adopted mechanical<br />
principles, 2,3 others used biometric guides 4 and a minority<br />
advocated mathematical formulas based on natural teeth<br />
position and dimensions. 5 These dogmatic or arbitrary<br />
approaches have been challenged and found insufficient,<br />
in fact not only by rigorous research, but also by failure<br />
to restore function, aesthetic and comfort in patients with<br />
severely atrophic mandibular ridges (Class V Atwood’s 6 ),<br />
patients with enlarged tongue and cases of marginal or<br />
segmental mandibulectomy. To overcome such problem,<br />
the neutral zone technique was advocated.<br />
The neutral zone, zone of minimal conflict, 7 zone of<br />
equilibrium, 8 potential denture space 9 and the dead<br />
space 10 are all terms used to describe the potential area<br />
where forces generated in an outward direction from the<br />
tongue are being neutralized or balanced by the inward<br />
forces generated by lips and cheeks during functional<br />
activities. Setting teeth and contouring polished surface<br />
of lower CD within this zone, makes the prosthesis less<br />
subjected to dislodging forces and adds more to stability. 11<br />
Analysis of functional forces<br />
Understanding the unique and synergistic interplay<br />
and complex movements of muscles of cheeks, lips<br />
and tongue is the first step in construction of lower<br />
CD that is stabilized rather than being dislodged by<br />
movements of these structures. 11,12 Description of forces<br />
applied to the lower CD purely on the basis of direction<br />
is an oversimplification, yet, it is quite useful for better<br />
understanding of the concept. 12<br />
The outward forces are principally generated by the<br />
tongue and lingual frenum into which, genioglossus<br />
muscle is inserted. Teeth should be set and flanges should<br />
be contoured in harmony with tongue size, position and<br />
shape during rest and function. In rest position, the tongue<br />
rests on lingual cusps of posterior teeth and lingual<br />
flanges posteriorly and anteriorly. The tongue space<br />
determined by position of teeth is far more important<br />
during function. Setting teeth too lingualy will encroach<br />
on this space and the tongue tends to dislodge denture<br />
in function. The height of posterior teeth is of a great<br />
importance in stability of lower CD as well. Having the<br />
tongue resting on lingual cusps will reduce the horizontal<br />
(outward) force and apply force with vertical (downward)<br />
component which enhances stability and retention. 11<br />
Inward forces are generated by cheeks resulting from<br />
contraction of the buccinator muscle that pushes food<br />
bullous on top of occlusal surfaces of posterior teeth.<br />
Flanges contoured and teeth set too buccal are at<br />
increased risk of being dislodged by the action of this<br />
muscle. Anteriorly, lip muscles (mentalis and orbicularis<br />
oris) are the source of inward forces generated during<br />
speaking and swallowing. Contraction of these muscles<br />
to attain seal during these activities can destabilize lower<br />
CD with teeth and flanges placed too far labially. The<br />
modiolus is a knot-like structure found in corners of the<br />
| 8 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011
mouth where several muscles are inserted. Movement of<br />
this structure narrows the space available for flanges and<br />
teeth. The modiolus produces quite strong inward forces<br />
in premolar region. Thus, contouring flanges in harmony<br />
with its’ functional movement is essential. 11,12<br />
Rationale<br />
The rationale of using neutral zone technique is to<br />
fabricate a lower CD that is optimally situated and in<br />
harmony with the structures and forces discussed above.<br />
By doing so, these forces are more likely to be stabilizing<br />
rather than unseating. 11 The need for such a technique<br />
that is based on physiologic concepts is significantly<br />
increasing as emergence of several factors (discussed<br />
below) render a high proportion of conventionally made<br />
lower CDs unsatisfactory.<br />
Increased access to dental care has led to patients losing<br />
their teeth at a later stage of life. 13 Compounded by<br />
increased life expectancy, this has led to the majority<br />
of CD wearers to be elderly and has increased the<br />
proportion of those who have poor neuromuscular<br />
control, poor adaptive capacity, severely atrophic<br />
ridges 14 and atypical denture support area as a result<br />
of surgical interventions, poor planning for transition<br />
from partially dentate to edentulous state, 15 untreated<br />
edentulism for long period of time ,16,17 trauma or<br />
systemic diseases. Occasionally, patients with one or<br />
a combination of these conditions can be successfully<br />
treated by CD constructed by conventional techniques. 11<br />
Indications<br />
• In general, neutral zone technique is indicated when<br />
stability and patient’s acceptance of lower CD are in<br />
question. Searching the literature, this technique is<br />
found to be used in the following clinical situations:<br />
• Severely atrophic mandibular ridge 12,13,18-22 (Atwood’s V).<br />
• Patients with prominent and highly attached mentalis<br />
muscle, lateral spreading of tongue as a result of poor<br />
transition from dentate to edentulous state and severe<br />
resorption. 13<br />
• Patients with diminished neuromuscular control such as<br />
those with a history of stroke, 13 Parkinson’s disease 13,23<br />
or patients with impaired motor innervation to oral and<br />
facial muscles as a result of brain surgery. 18<br />
• Patients with atypical shape or consistency of oral<br />
and perioral structures. For example, patients who<br />
have scleroderma, 13 marginal 21,24 or segmental 25,26<br />
mandibulectomy and partial glossectomy. 27<br />
• NZ technique can be used to locate optimal position<br />
for implants in cases of implant-supported or -retained<br />
overdentures, which enhances the overall outcome of<br />
treatment. 28<br />
Clinical technique<br />
Primary and secondary impressions are taken for<br />
maxillary and mandibular denture bearing areas as in<br />
standard complete denture treatment. Bite registration<br />
is then performed as in conventional treatment. Master<br />
casts with record blocks should be mounted on an<br />
articulator. In the lab, the lower occlusal rim is removed<br />
from baseplate and substituted with a baseplate with<br />
acrylic pillars 29 in the premolar regions and/or wire<br />
loops 13 on the remaining areas of the baseplate. The<br />
pillars preserve the VDO recorded in bite registration<br />
stage. It is essential the the pillars are relatively thin<br />
bucco-lingually and are positioned directly over the<br />
ridge. The base plate is then fitted in the patient’s mouth<br />
and VDO and extensions are checked. Then impression<br />
material such as compound 11 , plaster 22 , wax 30 , silicone 31 ,<br />
polyether 32 or tissue conditioner 13,33 is applied to the<br />
baseplate and retained by the wire loops and/or acrylic<br />
pillars. Before setting of material, patient is asked to<br />
perform functional movement such as, licking lips,<br />
swallowing, pronouncing some words or combination<br />
of these. Care should be taken that the patient should<br />
continue performing functional movements until the full<br />
setting of material; otherwise material might flow back<br />
and give inaccurate recording of the neutral zone. It is<br />
useful if the chosen material has relatively long working<br />
time to allow the required movements to be carried out<br />
before the material becomes rigid. Also, it is worthwhile<br />
to mention that it is better to perform the NZ record<br />
while the upper occlusal rim or finished denture is fitted<br />
in the patient mouth as it may help to control recording<br />
material and prevent it from being displaced in a labioocclusal<br />
direction. 29<br />
In the lab, the baseplate carrying recording material is<br />
fitted on the master cast again and VDO is checked. A<br />
putty or plaster index is made around the NZ record.<br />
Placement of three orientation grooves is recommended<br />
as these help in repositioning the index on the master cast.<br />
Impression material is then removed and replaced<br />
by wax; the use of the index will make sure that wax<br />
replicates the neutral zone record. Subsequently, teeth<br />
should be set and flanges contoured according to the<br />
index that represents NZ.<br />
NZ impression technique has various modifications, not<br />
only in terms of materials used or retention provided by<br />
baseplate, but also in terms of the functional movements<br />
performed and refinement of the procedure. A further<br />
more defined NZ record can also be achieved in try-in<br />
stage. The wax below the teeth and covering the flanges<br />
can be cut back and tissue conditioning material or<br />
medium-bodied silicone applied. The patient is asked<br />
again to perform functional movements. The dentures<br />
are processed as usual. The same procedure has also<br />
(Table 1) Materials Used for NZ Impression<br />
Impression plaster<br />
Impression waxes<br />
Impression compound<br />
Regular bodied silicone<br />
Tissue conditioner<br />
Polyether<br />
Hard relining material<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011| 9 |
(Table 2) Summary of clinical and laboratory stages of NZ<br />
technique<br />
Clinic 1: Upper & lower primary impressions using stock trays<br />
Lab1: Casting primary models and construction of special trays<br />
Clinic 2: Upper & lower secondary impressions<br />
Lab 2: Casting master models and construction of record blocks<br />
Clinic 3: Bite registration<br />
Lab 3: Mounting master casts using CR record on semi-adjustable<br />
or average value articulator. Removal of lower wax rim and fabrication<br />
of baseplate for NZ impression<br />
Clinic 4: NZ impression<br />
Lab 4: NZ impression record mounted on lower master cast, orientation<br />
grooves placed on master cast, putty index adapted around<br />
NZ record and impression material removed and poured in wax<br />
Finally, setting of teeth completed<br />
Clinic 5: Try-in stage. Afterwards, NZ impression refined by tissue<br />
conditioner applied to lower try-in denture<br />
Lab 5: Processing, finishing and polishing<br />
Clinic 6: Insertion of finished dentures<br />
been described after insertion of the denture but using<br />
hard relining material. 27,31<br />
Discussion<br />
Many approaches to set teeth have been advocated and<br />
used in complete denture treatment. 20 However, there<br />
is substantial debate on which of these provide optimal<br />
position in the facio-lingual dimension and guarantee a<br />
favourable outcome in terms of stability, facial support,<br />
chewing efficiency, aesthetics and patient comfort. Some<br />
of these approaches utilized biometric measurements and<br />
location of relatively stable anatomical landmarks to set<br />
teeth; 4 others relied on difference in resorption patterns<br />
to set denture teeth where their natural predecessors<br />
were thought to have been. 34 Some authors adopted a<br />
mechanical concept and advocated setting teeth directly in<br />
the centre of denture support area where the least amount<br />
of leverage is present which in turn enhances the stability<br />
of lower CD. 35 All of these approaches were and are still<br />
being used and each of them proved to have advantages<br />
and disadvantages when compared to others. Furthermore,<br />
these approaches seem to work best when used with<br />
patients who have; their oral and peri-oral musculature<br />
unaltered for any reason, adequate neuromuscular control<br />
and acceptable amount of residual ridge for support.<br />
Unfortunately, the proportion of patients with these features<br />
is dramatically decreasing and so the NZ concept has<br />
become increasingly significant. These observations are<br />
strongly supported by studies investigating the effect of<br />
period of edentulism on position of neutral zone. It has<br />
been found that NZ is closely related to the crest of residual<br />
(Fig. 1) NZ baseplate with<br />
acrylic pillars and wire loop<br />
(Fig. 2) A: NZ impression taken with silicon. B: Putty index<br />
adapted around master cast<br />
ridge in patients who have been edentulous for less than<br />
two years and significantly differs in those who were<br />
edentulous for a period more than that. 16,17<br />
Realizing the importance of the forces generated<br />
by various oral structures on the teeth and polished<br />
surfaces of CDs and their effect on the stability of CD<br />
sheds light on the NZ technique. 1,10 It has been shown<br />
that compromised retention, poor stability, phonetic<br />
problems, inadequate facial support, inefficient<br />
tongue posture/function and increased gagging are<br />
all associated with functionally inappropriate setting of<br />
denture teeth and physiologically inadequate contours<br />
or volume of the denture base. 20<br />
NZ technique has been criticized based on claims that<br />
it is supported by empirical evidence. However, other<br />
authors maintain that this is inaccurate as NZ technique<br />
is based on significant clinical observations on the role<br />
of destabilizing forces the muscles apply to CDs during<br />
functional movements. Furthermore, the large number of<br />
case reports accumulated in a short period of time and<br />
clinical studies conducted by Stromberg & Hickey 36 and<br />
Fahmy & Kharat 37 undermine this criticism and add to<br />
the validity of NZ technique. Stromberg & Hickey 36 found<br />
better patient adaptability to physiologically formed<br />
denture bases when compared to conventional ones.<br />
Fahmy & Kharat 37 found improved comfort and speech<br />
clarity reported by patients upon wearing CD fabricated<br />
using NZ technique when compared to conventional<br />
CD. Moreover, Barrenas and Odman found less post<br />
insertion problems and better patient acceptance in<br />
NZ dentures when compared to conventional ones. 38<br />
(Table 3) Summary of NZ impression clinical technique<br />
Baseplate with acrylic pillars and/or wire loop is fitted in patient’s<br />
mouth and checked for proper extensions and VDO<br />
Baseplate is coated by adhesive and loaded with regular bodied<br />
silicone impression material<br />
While the patient is setting upright and comfortable the baseplate is<br />
inserted in patient’s mouth<br />
Patient is then asked to swallow few time, moisten lips, use tongue to<br />
clear buccal sulci, smile, grin and purse lips<br />
Before final setting of material, patient is asked to read loudly a<br />
vocal passage<br />
Once set, NZ impression removed and inspected for deficiencies<br />
which can be corrected by addition of impression material<br />
Impression disinfected and sent to lab<br />
| 10 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011
(Fig. 3) Setting of teeth according to NZ record. Note the class II<br />
arrangement of teeth<br />
Recently, Raja and Saleem 19 published results of clinical<br />
trial in which they compared patient acceptance of NZ<br />
dentures and conventional dentures in 128 patients. The<br />
authors concluded that there is no significant difference<br />
in terms of patient’s acceptance between the two groups<br />
as far as patients who have been edentulous for less<br />
than two years are concerned. However, in patients who<br />
have been edentulous for more than two years, better<br />
results and patient acceptance were reported with NZ<br />
dentures. Unfortunately, the aforementioned studies can<br />
be criticized in terms of design or information about<br />
blinding and randomization which affects the quality of<br />
evidence taken from these studies.<br />
The principle of the NZ concept has remained the<br />
same since it has been first described by Beresin and<br />
Schiesser. However, the technique has been subjected to<br />
various modifications. Type of retention incorporated in<br />
the baseplate (acrylic pillars or wire loops 13 ), recording<br />
materials used and further refinement to the initial<br />
record are among the variations between clinicians.<br />
The authors’ preference is to use combination of thin<br />
acrylic pillars in premolar region connected by a wire<br />
loop which maintains the VDO and provides maximum<br />
retention at the same time. Medium or regular bodied<br />
silicone impression material used along with adhesive<br />
for the initial record that is refined in the try-in stage by<br />
tissue conditioning material is the personal preference of<br />
the authors for purposes of NZ recording.<br />
(Fig. 4) Refined NZ record using tissue conditioner on try-in denture<br />
The effect of various functional movements patients<br />
perform during recording NZ on the location and<br />
dimensions of NZ has been investigated by Makzoumi 39 .<br />
This investigation concluded that NZ recorded whilst<br />
patients perform a phonetic exercise is significantly<br />
narrower when compared with a NZ record produced<br />
during swallowing. This finding may be of a clinical<br />
significance from two perspectives; first, the author used<br />
modelling compound for the swallowing and used tissue<br />
conditioner for phonetic technique which may indicate<br />
that one of these materials is less reliable than the other<br />
in recording NZ. Second, dentures fabricated utilizing<br />
one functional exercise to shape the NZ may be unstable<br />
during other functions. The authors’ preference is to as<br />
patients to perform multiple tasks including swallowing,<br />
using the tongue to moisten lips and finishing with<br />
reading a speech articulation passage loudly.<br />
From biomechanical perspective, NZ technique has<br />
one disadvantage as teeth may be set far from the<br />
denture support area. For example, in a case of<br />
excessive resorption of the anterior area of the mandible<br />
accompanied by prominent and highly attached mentalis<br />
muscle, this will shift the NZ more lingually away from<br />
the crest of the ridge. This horizontal discrepancy can<br />
increase the leverage forces on the denture and may<br />
destabilize it. 21 However, there is an agreement that<br />
these leverage forces are well counterbalanced by<br />
favourable and seating forces resulting from optimal<br />
placement of teeth and polished surfaces of denture<br />
being in harmony with the tongue, lips and cheeks. 1,11,40<br />
Conclusion<br />
NZ concept is considered as exceptionally important<br />
when considering treatment options for patients<br />
complaining from unstable lower CD particularly<br />
if implant treatment is not feasible. It aims to place<br />
lower CD where forces generated by lips, cheeks and<br />
tongue have a stabilizing rather than dislodging effect.<br />
The principle technique used to record neutral zone<br />
is extensively recorded; yet it needs to be backed up<br />
with high quality clinical trials to push it further up on<br />
the hierarchy of evidence. It is not a widely practiced<br />
procedure while the proportion of patients that may<br />
befit from is significant. This may be attributed to a lack<br />
of experience and exposure to this technique during<br />
undergraduate training and the associated increase in<br />
chair time and laboratory costs.<br />
Acknowledgement<br />
The authors would like to acknowledge with gratitude Dr.<br />
Brian Nattress for his continuous support and cheif dental<br />
technician, Carol Scholfield, for the skilled lab work.<br />
References<br />
1. Fish E. Principles of Full Denture Prosthesis. 7 th Ed. London: Staple<br />
Press,Ltd;1948.<br />
2. Wright Cr, Swartz Wh, Godwin Wc. Mandibular Denture Stability: A New<br />
Concept. Overbeck;1961.<br />
3. Lammie G. Aging Changes and the Complete Lower Denture. J Prosthet<br />
Dent. 1956;6:450-64.<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011| 11 |
Dubai - Abu Dhabi<br />
FIRST INTERNATIONAL POSTGRADUATE<br />
DENTAL INSTITUTION IN THE REGION<br />
"All programs accredited by UAE Ministry of<br />
Higher Education & Scientific Research"<br />
3-YEAR MASTER DEGREE IN ORTHODONTICS<br />
3-YEAR MASTER DEGREE IN ENDODONTICS<br />
Visit<br />
Us<br />
2012 Admissions Currently Open<br />
3-YEAR MASTER DEGREE IN PEDIATRIC DENTISTRY<br />
3-years full time<br />
Clinical, Theoretical & Research<br />
Patient Care, GA Facilities, & Special Needs Care<br />
In Cooperation with Malmo University - Sweden<br />
Clinical, Theoretical & Research<br />
3-years full time<br />
3-years full time<br />
Clinical, Theoretical & Research<br />
Operating Microscope Facilities, Computerized Radiography<br />
1-YEAR HIGH DIPLOMA ORAL IMPLANTOLOGY<br />
In Cooperation with Gothenburg University - Sweden<br />
Clinical, Theoretical & Research<br />
1-year full time<br />
6th intake<br />
2nd intake<br />
2-YEAR DIPLOMA IN ADVANCED EDUCATION IN GENERAL DENTISTRY (AEGD)<br />
3rd intake<br />
6th intake<br />
3rd intake<br />
2-years full time<br />
Clinical & Theoretical<br />
Operating Microscope Facilities, Computerized Radiography<br />
AEEDC DUBAI 2012<br />
31 January - 2 February<br />
Stand No. 18<br />
4. Pound E. Esthetic Dentures and Their Phonetic Values. J Prosthet Dent.<br />
1951;1:98-111.<br />
5. El-Gheriani As. A New Guide for Positioning of Maxillary Posterior Denture<br />
Teeth. <strong>Journal</strong> of Oral Rehabilitation. 1992;19(5):535-8.<br />
6. Atwood Da. Postextraction Changes in the Adult Mandible as Illustrated<br />
by Microradiographs of Midsagittal Sections and Serial Cephalometric<br />
Roentgenograms. The <strong>Journal</strong> of Prosthetic Dentistry. 1963/10//;13(5):810-24.<br />
7. Matthews E. Br Dent J. 1961;111(The Polished Surfaces) :407-11.<br />
8. Grant Aa, Johnson W. An Introduction to Removable Denture Prosthetics. C.<br />
Livingstone; 1983.<br />
9. Roberts A. The Effects of Outline and Form Upon Denture Stability And<br />
Retention. Dent Clin North Am. 1960;4:293-303.<br />
10. Fish E. Using The Muscles To Stabilize The Full Lower Denture. J Am Dent<br />
Assoc. 1933;20:2163-9.<br />
11. Beresin Ve, Schiesser Fj. The Neutral Zone in Complete Dentures. The <strong>Journal</strong><br />
of Prosthetic Dentistry. 1976;36(4):356-67.<br />
12. Gahan Mj, Walmsley Ad. The Neutral Zone Impression Revisited. Br Dent J.<br />
2005;198(5):269-72.<br />
13. C.D Lynch Pfa. Overcoming the Unstable Mandibular Complete Denture: The<br />
Neutral Zone Impression Technique. <strong>Dental</strong> Update. 2006;33:21-6.<br />
14. Miller Wp, Monteith B, Heath Mr. The Effect of Variation of The Lingual Shape<br />
of Mandibular Complete Dentures on Lingual Resistance to Lifting Forces.<br />
Gerodontology. 1998;15(2):113-9.<br />
15. Allen Pf, Wilson Nhf. Teeth for Life for Older Adults. Quintessence;2002.<br />
16. F.M F. The Position of the Neutral Zone in Relation to the Alveolar Ridge. The<br />
<strong>Journal</strong> of Prosthetic Dentistry. 1992;67(6):805-9.<br />
17. Raja Hz Sm. Relationship of Neutral Zone and Alveolar Ridge with Edentulous<br />
Period. J Coll Physicians Surg Pak. 2010;20(6):395-9.<br />
18. Memarian Lsfgsfam. Using Neutral Zone Concept in Prosthodontic Treatment<br />
of a Patient with Brain Surgery: A Clinical Report <strong>Journal</strong> of Prosthodontic<br />
Research. 2011;55(2):117-20.<br />
19. Hina Z. Raja Mns. Neutral Zone Dentures Versus Conventional Dentures in<br />
Diverse Edentulous Periods Biomedic. 2009;25:136-45.<br />
20. Cagna Dr, Massad Jj, Schiesser Fj. The Neutral Zone Revisited: From<br />
Historical Concepts to Modern Application. The <strong>Journal</strong> of Prosthetic Dentistry.<br />
2009;101(6):405-12.<br />
21. Wee Ag, Cwynar Rb, Cheng Ac. Utilization Of The Neutral Zone Technique<br />
For A Maxillofacial Patient. <strong>Journal</strong> of Prosthodontics. 2000;9(1):2-7.<br />
22. Johnson A Ns. The Unstable Lower Full Denture-A Practical and Simple<br />
Solution. Restor Dent. 1989;5:82-90.<br />
23. Makzoume J. Complete Denture Prosthodontics for a Patient with Parkinson’s<br />
Disease Using the Neutral Zone Concept: A Clinical Report. Gen Dent.<br />
2008;56(4):E12-6.<br />
24. G. P, C., Hekimoglu, N., Sahin. Rehabilitation of a Marginal Mandibulectomy<br />
Patient Using a Modified Neutral Zone Technique: A Case Report. Braz Dent J.<br />
2007;18(1):83-6.<br />
25. Pravinkumar G. P. Conventional Complete Denture for a Left Segmental<br />
Mandibulectomy Patient: A Clinical Report. <strong>Journal</strong> of Prosthodontic Research.<br />
2010;54(4):192-7.<br />
26. Kokubo Y, Fukushima S, Sato J, Seto K. Arrangement of Artificial Teeth in the<br />
Neutral Zone after Surgical Reconstruction of the Mandible: A Clinical Report.<br />
The <strong>Journal</strong> of Prosthetic Dentistry. 2002;88(2):125-7.<br />
27. Ohkubo C, Hanatani S, Hosoi T, Mizuno Y. Neutral Zone Approach for<br />
Denture Fabrication for a Partial Glossectomy Patient: A Clinical Report. The<br />
<strong>Journal</strong> of Prosthetic Dentistry. 2000;84(4):390-3.<br />
28. Yasunori Suzuki Coath. Implant Placement for Mandibular Overdentures<br />
Using the Neutral Zone Concept. Prosthodont Res Pract. 2006;5:109-12.<br />
29. Basker Rm, Davenport Jc, Thomason Jm. Prosthetic Treatment of the Edentulous<br />
Patient. John Wiley & Sons; 2011.<br />
30. Lott F, Levin B. Flange Technique: An Anatomic and Physiologic Approach to<br />
Increased Retention, Function, Comfort, and Appearance of Dentures. The<br />
<strong>Journal</strong> of Prosthetic Dentistry. 1966/6//;16(3):394-413.<br />
31. Mccord Jf, Grant Aa. Prosthetics: Impression Making. Br Dent J. [10.1038/<br />
Sj.Bdj.4800516]. 2000;188(9):484-92.<br />
32. Agarwal S, Gangadhar P, Ahmad N, Bhardwaj A. A Simplified Approach<br />
for Recording Neutral Zone. The <strong>Journal</strong> of Indian Prosthodontic Society.<br />
2010;10(2):102-4.<br />
33. P. K, N., Ari, S., Calikkocaoglu. Using Tissue Conditioner Material in Neutral<br />
Zone Technique. N Y State Dent J. 2007;73(1):40-2.<br />
34. David M W. Tooth Positions on Complete Dentures. <strong>Journal</strong> of Dentistry.<br />
1978;6(2):147-60.<br />
35. Sharry Jj. Complete Denture Prosthodontics. Mcgraw-Hill; 1974.<br />
36. Stromberg Wr, Hickey Jc. Comparison of Physiologically and Manually<br />
Formed Denture Bases. The <strong>Journal</strong> Of Prosthetic Dentistry.15(2):213-26.<br />
37. Fahmy Fm, Kharat Du. A Study of the Importance of the Neutral Zone in<br />
Complete Dentures. The <strong>Journal</strong> of Prosthetic Dentistry. 1990;64(4):459-62.<br />
38. Barrenäs L, Ödman P. Myodynamic and Conventional Construction of<br />
Complete Dentures: A Comparative Study of Comfort and Function. <strong>Journal</strong><br />
of Oral Rehabilitation. 1989;16(5):457-65.<br />
39. Makzoume Je. Morphologic Comparison of Two Neutral Zone Impression<br />
Techniques: A Pilot Study. The <strong>Journal</strong> of Prosthetic Dentistry. 2004;92(6):563-8.<br />
40. Gt. Mcdonald H, Larsen. The Neutral Zone Space: A Clue to Denture Stability.<br />
Gen Dent. 1984;32(6):510-1.<br />
+97143624784 candidate@nicolasasp.ae www.dubaipostgraduate.com<br />
| 12 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011
3Shape<br />
<strong>Dental</strong> System<br />
Digitally moving the<br />
world of dentistry<br />
TRIOS ®<br />
3Shape TRIOS ®<br />
NEW<br />
3Shape’s new intraoral digital impression<br />
solution cements lab-dentist relationships<br />
THE FUTURE IS NOW<br />
Projet MP 3000<br />
3D-based manufacturing<br />
Digital Study Models and 3D<br />
treatment plans can be used<br />
directly to creat 3D Physical<br />
Models by rapid prototyping<br />
technology.<br />
Meet us in AEEDC booth 56<br />
MENAPA Distribution<br />
Group of Companies<br />
Victoria Tower - 530, Corniche al Naher - P.O.Box 165 884 Beirut, Lebanon<br />
Tel +961 1 612 216 - Fax +961 1 42 46 42 - info@prodent-me.com - www.prodent-me.com
<strong>Dental</strong> Implants’ Homepages:<br />
Are they Educative?<br />
A Cross-Sectional Study<br />
Layla Abdel-Aziz Abu-Naba’a<br />
BDS, PhD, MFDRCS<br />
• Department of Substitutive<br />
oral sciences, college of<br />
dentistry, Taibah University,<br />
AlMadinah AlMonawwarah<br />
KSA<br />
• Formerly Prosthodontic<br />
Department, Jordan<br />
University of Science and<br />
Technology, Jordan<br />
laylanabaa@hotmail.com<br />
Abstract<br />
<strong>Dental</strong> implant manufacturers’ web pages are presenting more links to educative<br />
material targeting students, dental practitioners, technicians, and patients.<br />
Aim: This cross-sectional study aims to describe the amount of links to educational and<br />
scientific material in comparison with links to information, support services and other<br />
web-based material using a standardized methodology.<br />
Material and methods: A convenient sample of dental manufacturers’ web pages<br />
was chosen. The ADA lists 39 companies in its dental buying guide “ IMPLANTS AND<br />
ACCESSORIES CATEGORY “ in 2010. Icons present in the companies web pages are active<br />
links, which linked the surfer to other web pages. The subsequent webpage was categorized<br />
according to the material presented in it as: Educational and scientific materials,<br />
Information materials, Services and support materials. Target audiences were described.<br />
Results: This study shows that homepages focus on being directories, containing<br />
variable numbers of clickable icons. Clicking them lead the reader to other web pages,<br />
either containing the actual material of interest, or containing another directory of more<br />
clickable icons. Types of material presented by the clickable icons on the homepages<br />
of the sample, included a sum of 93 informative, 64 service related or supportive<br />
and 85 lead to material described as educational. Three homepages represented a<br />
comprehensive directory by including icons leading to all three materials’ categories(one<br />
included a sum of 78 links, the second included 57 and the final had 42 links).<br />
Conclusions: Within the limit of this cross sectional study, it is concluded that<br />
educational material is considered as a major category of material presented by the<br />
homepages of dental implant manufacturers.<br />
Keywords: <strong>Dental</strong> Implants, Education, e-resources, Cross-sectional study, Internet.<br />
Introduction<br />
Internet became a preferred tool for enquiries, information gathering and<br />
communications for many. Clinical skills of health professionals were enhanced by this<br />
new learning behavior that evolved with the expanding use of the net. It helped surfers<br />
to answer patient related questions, pharmaceutical inquiries, and update and follow<br />
clinical developments. 1<br />
However, many experts involved in critical appraisals of internet-disseminated<br />
materials, advocated professionals to perform informed searches and rely on evidence<br />
derived from good research. 2 They disseminated this message by spreading the word<br />
through the internet!<br />
<strong>Dental</strong> bodies also promote evidence-based dentistry and set guides for the learners<br />
on how to judge the hierarchy of evidence. More and more educative material are<br />
distributed by the internet as an instructional method, which proved better than traditional<br />
methods. 3 Now it is accepted to accumulate independent-study points from internet-<br />
| 14 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011
ADA.org: <strong>Dental</strong> Buying Guide<br />
Page 1 of 2<br />
based courses, as for continuation of dental practice<br />
licensure. 4 Teledentistry, dental informatics and dental<br />
portals, are subject which have developed into mature<br />
branches of specialty, revolving around the internet<br />
technology and the delivery of reliable knowledge. 5-8<br />
Implant manufacturers developed their web pages,<br />
accordingly, to become more educative. An increasing<br />
number of homepages contain dedicated sections for<br />
evidence and continual education. Some manufacturers<br />
began investing in educational institutions which<br />
prioritize research. Others have devoted funds, advisors<br />
and publications which would help perform and later,<br />
disseminate results of studies using their implant systems.<br />
Educative material is presented to target a larger audience<br />
of implant service receivers, providers and distributers.<br />
Aim<br />
This cross sectional study aims to develop a standardized<br />
methodology to describe webpage contents in <strong>Dental</strong><br />
Implant manufacturers’ webpages. Links present were<br />
to be categorized to educational (scientific material) in<br />
comparison with links to information, support services<br />
and other web-based material present in. Then a<br />
comparison of a sample of homepages for 12 valid<br />
and current implant manufacturers was done using this<br />
standardized methodology.<br />
Materials and Methods<br />
Bicon Definitions <strong>Dental</strong> Implants<br />
Selection of manufacturers’ homepages<br />
A valid and current manufacturer means; that the<br />
company is consistent in its ownership, still managing<br />
ADA LIBRARY<br />
ADA PUBLICATIONS<br />
About ADA Publishing<br />
ADA News Today<br />
Advertise in<br />
ADA Publications<br />
Advocacy Publications<br />
Buying Guide<br />
Classifieds<br />
E-Publications/E-mail<br />
<strong>Journal</strong> of the ADA<br />
Subscribe<br />
Professional Product<br />
Review<br />
DENTAL CAREERS AND<br />
JOB LISTINGS<br />
EVIDENCE BASED<br />
DENTISTRY<br />
PODCASTS<br />
ADA POLICIES & POSITIONS<br />
STANDARDS<br />
Licensure | Catalog | Member Directory | Contact<br />
DENTAL BUYING GUIDE<br />
Introduction Listing in the Buying Guide<br />
Buying Guide Search Contact the Buying Guide<br />
New Dentist Resources<br />
Product Category Search Results for 'Implants and Accessories'<br />
3i, Palm Beach Garden, FL<br />
Ace Surgical Supply Co Inc., Brockton, MA<br />
AIT <strong>Dental</strong>, Inc, Beverly Hills, CA<br />
Aseptico Inc, Woodinville, WA<br />
Asteto Dent Labs, Maplewood, NJ<br />
Astra Tech, Inc., Lexington, MA<br />
Attachments International, San Mateo, CA<br />
Bicon <strong>Dental</strong> Implants, Boston, MA<br />
Bien Air USA, Irvine, CA<br />
Bio-Lok International, Inc., Deerfield Beach, FL<br />
Butler Company, John O., Chicago, IL<br />
De' Plaque Inc., Victor, NY<br />
<strong>Dental</strong> Arts Laboratories Inc, Peoria, IL<br />
Dentatus USA Ltd., New York, NY<br />
Dentsply International, York, PA<br />
Drake Precision <strong>Dental</strong> Lab, Charlotte, NC<br />
Essential <strong>Dental</strong> Systems, South Hackensack, NJ<br />
EURO DENTAL IMPLANT, Houston, TX<br />
Euro Teknika, Houston, TX<br />
Florida <strong>Dental</strong> & Medical Supply, Miami, FL<br />
G & H <strong>Dental</strong> Arts, Inc., Torrance, CA<br />
Hartzell & Son, G., Concord, CA<br />
Implamed, Attleboro, MA<br />
IMTEC Corp, Ardmore, OK<br />
ITL <strong>Dental</strong>, Santa Ana, CA<br />
Keller Laboratories Inc., St. Louis, MO<br />
Lifecore Biomedical, Chaska, MN<br />
Nobel Biocare USA, Inc., Yorba Linda, CA<br />
Paragon Implant Company, Encino, CA<br />
(Fig. 1) The Sample of study was derived from the ADA <strong>Dental</strong><br />
buying guide, (Implants and Accessories) product category<br />
accessed on the 7 th February 2010<br />
Polymedia Inc., Canton, MA<br />
and maintaining PracticeWares the active <strong>Dental</strong> Supply, website Rancho Cordova, CA related to dental<br />
Procera, Yorba Linda, CA<br />
implants. Homepages Prowest <strong>Dental</strong> Lab, of San these Francisco, CAcompanies are listed by<br />
Recigno Laboratories Inc, Willow Grove, PA<br />
the ADA webpage (fig. 1). Being current means that the<br />
Steri-Oss, Yorba Linda, CA<br />
Sterngold, Attleboro, MA<br />
manufacturer was still distributing the implant system.<br />
The mhtml:file://H:\D\LAYLA\KSA\Research\Implants\D homepage is defined here Jafar-website as the first research-\implant English pop...<br />
internet webpage appearing after<br />
Page<br />
placing<br />
1 of<br />
the<br />
2<br />
simplest<br />
URL address (~.com) and relevant to dental implants.<br />
Once placed in the address bar, the URL address<br />
could either remain the same, or it could automatically<br />
27-Dec-11<br />
Monday, December 26th 2011 3:41PM EST CONTACT US | LAB ONLINE STORE<br />
i<br />
Since 1985 » Simple. Predictable. Profitable.<br />
HOME OVERVIEW PRODUCTS CASES VIDEOS COURSES CALENDAR MANUALS DOWNLOADS NEWS<br />
s<br />
Clinically proven since 1985, Bicon’s unique dental implants and its revolutionary clinical techniques have not only passed the test of time, but also<br />
i<br />
e e<br />
e<br />
continue to lead implant dentistry. We welcome your joining Bicon clinicians from around the world, so that both you and your patients may also<br />
enjoy the many clinical benefits of Bicon implants.<br />
i<br />
s<br />
e<br />
e<br />
Search<br />
UPCOMING COURSES<br />
2/1-3 Surgical and Prosthetic<br />
Principles Course • Boston, MA<br />
2/8 Intro Live Surgery Tutorial<br />
1 • London, UK<br />
2/17 Hands-On Practical Course •<br />
Boston, MA<br />
2/21 Treatment Planning Tutorial<br />
2• Lndon, UK<br />
s<br />
s<br />
i<br />
(Fig. 2)<br />
Sample of one of<br />
the comprehensive<br />
webpages<br />
containing icons<br />
for the three main<br />
categories (e:<br />
educative materials,<br />
i: informative<br />
materials, s: service<br />
provisions). Flashes<br />
and animations<br />
are not active in<br />
this still image nor<br />
are embedded lists<br />
apparent<br />
s<br />
Information for Patients<br />
Since 1985 dentists have been offering patients<br />
the benefits of the Bicon <strong>Dental</strong> Implant System.<br />
With Bicon <strong>Dental</strong> Implants, your dentist has the<br />
ability to provide you with secure implant<br />
restorations often without the need for<br />
additional grafting procedures. The restorations<br />
s<br />
e<br />
e<br />
LATEST VIDEOS<br />
» REGISTER for Upcoming Webcast<br />
» Webcast Replays<br />
» Introductory Videos<br />
» Technique Videos<br />
e<br />
» Case Study Videos<br />
e<br />
i<br />
e<br />
UPCOMING EVENTS<br />
1/26-28 Yankee <strong>Dental</strong><br />
Congress • Boston, MA<br />
2/23-25 Chicago Midwinter<br />
Meeting • Chicago, IL<br />
3/1-3 AO Annual Meeting •<br />
Phoenix, AZ<br />
SHORT® Implants<br />
THE BICON DESIGN is driven by<br />
simplicity. One of the cornerstones of<br />
that simplicity is the innovation of<br />
SHORT® Implants. When the Bicon<br />
system was first introduced in 1985, its<br />
8.0mm length implants were considered<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011| 15 |
edirect to another URL. If the webpage is not relevant to<br />
implants, it becomes mandatory to choose the implant<br />
product line. Then the subsequent page is considered the<br />
homepage. Some webpages mandate the selection of<br />
the region first. Once selected, the subsequent page is<br />
considered the homepage.<br />
Sample selection<br />
A convenient sample of dental manufacturers’<br />
webpages was chosen. The ADA lists 39 companies in<br />
its dental buying guide “IMPLANTS AND ACCESSORIES<br />
CATEGORY”. The list provided, at the time of research,<br />
contains links to subsequent webpages per each company.<br />
Only 12 companies were valid and current implant<br />
manufacturers and their webpages were accessed, while<br />
the rest provided webpages for companies dealing with<br />
implant related materials and devices.<br />
Icon Definition<br />
An icon is defined here as an active link, where a web<br />
component can be clicked by mouse navigation or enter<br />
controls. The webpages provided clickable icons: in the<br />
form of buttons, images, or texts. The total number of<br />
these icons are counted either if directly seen on the home<br />
page or embedded in drop-down lists or in active flashes.<br />
Once clicked, these icons linked the surfer to other<br />
webpages. The labels used on these icons are put in<br />
parenthesis “ “. The subsequent webpage was categorized<br />
according to the material presented in it (fig. 2). Variations<br />
of content are reported in terms of:<br />
Labels and the sum of Educational and scientific<br />
materials provided<br />
Including “SCIENTIFIC ACTIVITIES”, “MATERIALS”,<br />
“CAREER DEVELOPMENT”, “CLINICAL SKILL<br />
DEVELOPMENT”, “DENTAL TECHNICIAN” and “PATIENT<br />
GUIDED INFORMATION”<br />
Labels and the sum of Information materials provided<br />
Including: “INTRODUCTORY”, “DISTRIBUTION”,<br />
“CORPORATION”, “HONORARIES” and “IMPLANTS’<br />
OVERVIEW INFORMATION”<br />
Labels and the sum of Services and support<br />
materials provided<br />
Including “PRODUCTS”, “NETWORK OF USERS”,<br />
“SUPPORT”, “SERVICES”, “COMMUNICATION”, and<br />
“SIGN-UPS”<br />
Target audience<br />
The paper describes the targeted audience besides<br />
conventional users of implant related webpages,<br />
including higher dental specialties, other professions and<br />
other users.<br />
Results<br />
Sample selection<br />
Twelve webpages were accessed from the ADA list of<br />
total 39 companies present in its dental buying guide<br />
“IMPLANTS AND ACCESSORIES CATEGORY”. The list<br />
provided, contains links to subsequent webpages per<br />
each company. These were considered sufficient to<br />
develop a standardized methodology of researching the<br />
contents of home pages.<br />
Seven webpages changed their web content slightly<br />
between two points of search (7 th February 2010, 20 th<br />
march 2010). Changes mainly were in blog areas<br />
called: highlights, news blog, upcoming courses and<br />
upcoming events blogs. One changed a congress<br />
announcement, added a “NEWS” icon and updated its<br />
<strong>copy</strong> right statement. Another announced redistribution<br />
of one of its implants. The next added a “LAB” icon,<br />
updated the flash presenting current events and changed<br />
language names into flags. Finally, one changed some<br />
icons in its footer quick link bar.<br />
Icon Identification on homepage<br />
Results of materials gained by clicking icons are briefed<br />
in table 1, “HOME” is an icon that leads to the homepage<br />
itself. This is useful as the header and footer links are fixed<br />
in subsequent webpages and could help redirect the reader<br />
back to the original webpage. Other material include.<br />
Educational and scientific material: labels and<br />
subjects<br />
Scientific Activities:<br />
“COURSES” and “UPCOMING COURSE” blogs were<br />
the only icons leading to webpages about courses in two<br />
homepages.<br />
Other activities as Meetings, symposia, scientific days,<br />
forums, congresses were announced and linked to, by<br />
labels “NEWS” and “EVENTS” present in homepages as<br />
blog sections or icons.<br />
Recourse Materials<br />
Multiple labels were used, “DOCUMENTATION”,<br />
“ARCHIVES”, “STUDIES”, and “LIBRARY”. One webpage<br />
had “MANUALS”, “DOWNLOADS” and “INTERNATIONAL<br />
DOWNLOADS” for 12 languages. One webpage had<br />
recourse materials reached by icons embedded in a<br />
drop-down list called “CLINICAL RESOURCES”, and<br />
contained “ARTICLES”, “BIBLIOGRAPHY”, “BROCHURES”,<br />
“LITERATURE” and “FAQ” icons.<br />
Professional and career Development<br />
Icons leading to relevant developments were labeled:<br />
“DENTAL PROFESSIONALS”, “PROFESSIONAL<br />
EDUCATION”, “CONTINUING EDUCATION”,<br />
“COURSES”, “CALENDAR” “EDUCATION”,<br />
“EDUCATION CALENDAR”, “EDUCATION AND<br />
EVENTS”, “ONLINE TRAINING”, “CONGRESS” and<br />
“SEMINAR TOURS”.<br />
One webpage had a very rich “CONTINUING<br />
EDUCATION” icon. It contained a drop-down list of<br />
| 16 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011
icons, labeled by name, for 4 seminars, 3 courses, and 2<br />
residencies.<br />
Clinical Skills Development<br />
Icons used were: “VIDEOS”, “MARGINAL BONE<br />
MAINTENANCE”, “CASE PRESENTATION”, and<br />
“IMPLANT ABUTMENT SELECTION GUIDE”. One<br />
webpage provided to icons “DIGITAL DENTISTRY” and<br />
a specific “NAME-IMAGING TECHNIQUE”. Another<br />
had “DIGITAL DENTISTRY” and “INDIVIDUALIZED<br />
PROSTHETICS”. One had country selections in dropdown<br />
lists from “CAD CAM” and “CARE” a specific<br />
service for customized prosthetics.<br />
<strong>Dental</strong> technician guided educative material<br />
Icons used were labeled: “LAB”, “LABORATORIES”,<br />
“TECHNICAL TIPS” and “TECHNICAL BULLETINS” icons.<br />
Patient guided educative material<br />
Icons used were labeled: “PATIENTS”, and “CONSUMER<br />
SITE”. Two webpages had a service, selecting country<br />
and region in a drop-down list, changing the language<br />
for the patients.<br />
Three webpages were rich, providing multiple patient<br />
materials. Icons were listed in sections or in drop-down<br />
lists from a “PATIENTS” icon; “FREQUENTLY ASKED<br />
QUESTIONS” “FIND A DOCTOR, OR DENTIST”, “ALL<br />
ABOUT IMPLANTS”, “TESTIMONIALS”, “PATIENT<br />
STORIES”, ”PATIENTS GUIDE TO IMPLANTS”, ”<br />
HOW IMPLANTS CHANGE YOUR LIFE”, “DENTAL<br />
GLOSSARY”, “PATIENT EDUCATION”, “GUM DISEASE”,<br />
”RESTORATIONS”, “PATIENTS’ SITE”, ” BEFORE AND<br />
AFTER”, and ”PATIENT VIDEOS”.<br />
Information material: labels and subjects<br />
Introductory information<br />
Introductions were in the form of full paragraphs.<br />
This was the only section containing paragraphs.<br />
These paragraphs either described the company, or<br />
their implant system. Some webpages labeled those<br />
paragraphs as “WELCOME NOTES”.<br />
Distribution information<br />
One homepage had a “GLOBAL HOME” icon which<br />
lead to a new webpage with a map asking to locate the<br />
region, in which the reader is living.<br />
One homepage used both labels “GLOBAL WEBSITES”<br />
and “WORLD WIDE”.<br />
Another used “INT’l” and “EUROPE” leading to<br />
webpages describing regional offices.<br />
One webpage had local distributors in a drop-down list<br />
from the icon “PRODUCTS”.<br />
Two webpages announced distributor change for one of<br />
their implants.<br />
Corporation information<br />
Labels expected to be used as synonyms were<br />
“COMPANY”, “CORPORATE”, OR “CORPORATE<br />
HEADQUARTERS”, “INCORPORATION”, “INC” and<br />
“MANUFACTURER”. But some homepages used them as<br />
separate icons, each leading to different material.<br />
One webpage used both “MANUFACTURER” and<br />
“COMPANY”, two webpages used both “HEAD<br />
QUARTERS” and “CORPORATE”, and one used both<br />
“CORPORATE” and “OUR COMPANY”. Each of the<br />
coupled icons, led to a different webpage.<br />
News information<br />
“NEWS” and “EVENTS” are another example of icons<br />
which seem to be equal but were used as separate labels:<br />
One homepage used “EVENTS” icon to lead to a<br />
webpage listing scientific events. The “NEWS” and<br />
“PRESS ROOM” blog were about products.<br />
In another homepage, “NEWS” linked to an e-bulletin<br />
mixing product news, offers, technique resources, and<br />
scientific events. The “CALENDAR” icon led to a list of<br />
scientific events. An icon “SUBSCRIBE TO BULLETIN” was<br />
also present that webpage.<br />
The next homepage had “NEWS AND EVENTS” in one<br />
icon and led to the following: press releases, to sign-in<br />
for an e-newsletter, product news, and scientific events.<br />
Another homepage included labels “NEWS” which linked<br />
to an announcement page, “EVENTS” led to a list of<br />
trade shows and courses.<br />
Icon ”NEWS AND EVENTS” in the next homepage, led to<br />
company and financial news.<br />
The next homepage, “EVENTS” icon led scientific<br />
courses, while “NEWS” led to company news, product<br />
news and tradeshows.<br />
Another homepage had ”CORPORATION ***-NEWS”<br />
linking to corporation events and speaks at multiple forums.<br />
The next homepage had “EDUCATION AND EVENTS”<br />
linked to scientific news, “MEDIA” led to both scientific<br />
and corporate news.<br />
The later had a news blog related to product news and<br />
company activities, and “MEDIA RELATIONS” icon for<br />
referred those seeking news.<br />
The final homepage, had “TRADESHOWS”, “E-NEWS”<br />
icons and an “EDUCATION CALENDAR” were dedicated<br />
to scientific events. Icons “PRESS RELEASE” and “E-NEWS<br />
LINKING” led to webpages about product news and<br />
clinical techniques, while its “HIGHLIGHTS BLOG” was<br />
dedicated to product news and scientific events. Two<br />
webpages had no icons termed “NEWS” or “EVENTS”<br />
Honoraries<br />
One homepage offered a research prize.<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011| 17 |
Information Services and Support Educational and Scientific<br />
Introductory Information Products Activities<br />
Introductory Paragraphs 6 Products 9 Upcoming Courses Blog 1<br />
Welcome Notes 2 On-Line Stores or E-Shop 6 Courses 1<br />
About Us 2 My Cart 1 Materials<br />
General Information 1 My Order 1 Documentation 1<br />
Overview 2 My Account 1 Manuals 1<br />
Prefaces, Who Are We?, What Is …?. 0 Consumer Site 1 International <strong>Download</strong>s 1<br />
Distribution Information Great Offers 1 Archives 1<br />
Regional Offices Store 1 Studies 1<br />
Global Home 2 Other Equipment 1 Library 1<br />
Home 7<br />
Product Catalogs, Online, PDF,<br />
Ordered to Mail or Email Address, 0 Brochures 1<br />
Restricted (Registering or Subscribing)<br />
Global Websites 1 Finding A Network Of Local Users Bibliography 1<br />
World Wide 2 Locate a Doctor or Find a Dentist 2 Literature 1<br />
Int’l 1 Laboratories 1 FAQ 1<br />
Europe 1 Support Articles 1<br />
Distributors 2 Products and Services 1 <strong>Download</strong>s 1<br />
Global Network, Distributors 1<br />
Costumers Support, and Costumers<br />
Services<br />
2 Clinical Resources 1<br />
Representatives, Trade Links, Regional<br />
Homepages, Put on a Map<br />
0 Technical Help and Technical Service 2<br />
Presentation Briefings, Multimedia, Publications,<br />
Abstracts, Case Reports, Books<br />
Corporation Information Engineering Services 1 Professional and Career Development<br />
Manufacturer 1 Advisory Board 1 <strong>Dental</strong> Professionals 2<br />
Company and Our Company 8 Return Policy 1 Calendar 1<br />
Head Quarters 1 Interaction Courses 1<br />
Corporate 3 Comment and Make an Inquiry 2 Education 3<br />
Name- Inc. 1 Help 1 Professional Education 1<br />
Company Logos- Sentence 4 Contact 5 Continuing Education 1<br />
President’s Message 1 Contact Us, 5 Education Calendar 1<br />
Executive Profile 1 Email Us 1 Education and Events 1<br />
Company News 1 Search Boxes 7 Congress 1<br />
Jobs and/or Careers 5 Search 1 Seminar Tours 1<br />
Investors and/or Investor Relation 2 Sitemap 3 Online Training 1<br />
Carriers Regional Sales Managers 1 Signups Name- Residency 2<br />
Company Activities Platinum Name- Course 3<br />
Trade Shows and Appearances 3 Login Name- Seminar 4<br />
Events 3 Extranet Login Clinical Skill Development:<br />
News 4 Signup for an E-Bulletin 1 Videos 2<br />
News and Events 2 E-News Letter 1 Manuals 1<br />
E-News 1 Signup Forms for E-News 2 Cases 1<br />
Sign-In for an E-News Letter 1 Pod Casts 1 Case Presentation<br />
Subscribe to Bulletin 1 Web Casts 1 Digital Dentistry 2<br />
Corporation Name-News 1 Syndications as RSS 0 Name of Imaging Technique 2<br />
Education and Events 1 Individualized Prosthetics 1<br />
Media 1 Implant Abutment Selection Guide 1<br />
Highlights Blog 1 CAD CAM and CARE 1<br />
Press Room Blog 1 On Marginal Bone Maintenance 1<br />
News Blog 1 <strong>Dental</strong> Technician Guided Information<br />
Media Relations 1 Laboratories 2<br />
0<br />
| 18 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011
Information Services and Support Educational and Scientific<br />
Introductory Information Products Activities<br />
Press Release 1 Technical Tips 1<br />
Company History, Corporation Structure,<br />
Staff Info.<br />
0 Technical Bulletins 1<br />
Legal and Webpage Issues Lab 1<br />
Site Requirements 1 Patient Guided Information<br />
Copyright Declarations 10 Patients’ Resource 1<br />
Legal Notices/ Terms/ Information 4 Patients 9<br />
Privacy Policy/ Statement 7 Patients’ Site 1<br />
Disclaimer 1 Patient Education 1<br />
Trade Marks 1 Consumer Site 1<br />
Conditions/Terms of Use 3 Frequently Asked Questions 1<br />
Imprint 1 Find a Doctor, or Dentist 1<br />
Honoraries All About Implants 1<br />
Research Prize 1 Patients Guide to Implants 1<br />
Surveys 3 Patient Videos 1<br />
Honors, Voted, Prizes (Products or<br />
Company) Quality Assurance Approvals,<br />
0 Before and After 1<br />
Polls<br />
Implants’ Overviews <strong>Dental</strong> Glossary 1<br />
Implant History 1 Restorations 1<br />
Image of the Abutment/ Implant 3 Single Tooth Restoration 1<br />
Implant Fixtures 1 Multiple Teeth Restoration 1<br />
Healing Abutments 1 Over Dentures 1<br />
Implants and Abutments 1 Partial Dentures 1<br />
Innovation, Advancements, Latest,<br />
What's Hot, New!<br />
0 Gum Disease 1<br />
Past Products, Deceased Lines, Manufacturing<br />
Process<br />
0 Testimonials 2<br />
Compatibility with Other Implant<br />
Systems<br />
0 Patient Stories 1<br />
How Implants Change Your Life 1<br />
(Table 1) Icons and content numbers are reported, for those included in dental implant manufacturers’ home page.<br />
Note: (“ ”) designate icons labels, (/ )separates possible synonyms, “INT”L” = international, FAQ = frequently asked questions (labels<br />
are quoted exactly as they appear in the webpage), and finally, “name- ******” indicates that the label uses trade names for the<br />
incorporation or a product line in the label. These are not reported here to preserve the identity of webpage. Repeated icon names in<br />
different categories indicate that these icons lead to different webpages addressing each separately, although having the same label.<br />
Surveys<br />
One homepage provided 3 icons to different surveys.<br />
Implants’ overviews<br />
Some of this information was present in subsequent<br />
webpages from “NEWS” and “EVENTS” icons, as<br />
advancements. More information will be displayed in the<br />
“PRODUCTS” icon explained later. Other information<br />
were contained in icons ”IMPLANT FIXTURES” and<br />
“HEALING ABUTMENTS”. One webpage provided an<br />
icon indicating the compatibility of their abutment with<br />
other implant systems.<br />
Services and support material: labels and subjects.<br />
Products: homepages provided information about<br />
products using the label “PRODUCTS” in the form of<br />
icons, flashes, and videos.<br />
Three homepages studied were redirected to implant<br />
webpages, as the first simple (~.com) webpage had no<br />
information on implants but featured other products.<br />
Once reaching the implant related webpage, now<br />
considered the homepage, one of them had a dropdown<br />
list from “PRODUCTS” icon listing 4 implants and<br />
3 implant related materials. The other two listed the<br />
implants and related products on the webpage itself.<br />
Icon “PRODUCTS”, is another example of how a<br />
label is variably used and leads to different webpage<br />
materials. One homepage used the label “PRODUCTS”<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011| 19 |
that led to other products which were not implants or<br />
implant related. Another homepage had a drop-down<br />
list embedded in the “PRODUCTS” icon, hiding further<br />
icons for 8 implant products, 5 prosthetic products, and<br />
11 surgical regenerative materials, related to implant<br />
therapy. One homepage had “PRODUCTS” icon leading<br />
to 2 implant lines and 5 implant related material.<br />
The next description of the label “PRODUCTS” is more<br />
complex as more material lie one click away, even not<br />
related to implant products.<br />
One homepage used “PRODUCTS” icon to lead to<br />
a webpage containing introductory paragraphs and<br />
further icons for implants, implant related materials<br />
and software. It also had icons labeled “MANUALS”,<br />
“PROCEDURES”, “PRODUCT CATALOGUE” and “HOW<br />
TO ORDER”.<br />
A second homepage linked “PRODUCTS” to a<br />
webpage containing images and an overview of one<br />
implant, more icons for “PRODUCT INFORMATION”,<br />
“CASE STUDIES”, “IMPLANTS”, “ABUTMENTS”<br />
“KITS”, “INSTRUMENTATION”, ” GRAFT MATERIAL”,<br />
“TRANSITIONAL IMPLANTS”, ” EDUCATIONAL<br />
MATERIALS”, “REFERENCES”, “FAQ” and “DOWNLOAD<br />
PDF CATALOGUE”.<br />
A third homepage linked “PRODUCTS” to a webpage<br />
containing an overview of one implant then icons<br />
FOR “IMPLANTS”, “REGENERATIVE”, “SURGICAL”,<br />
“RESTORATIVE”, “SHOPPING CART”, “CATALOGUE”,<br />
“SURGICAL MANUAL” and “CLINICAL OVERVIEW”.<br />
A fourth webpage homepage linked “PRODUCTS” to a<br />
webpage containing a list of further icons for “IMPLANT<br />
PRODUCTS” and 6 products not related to dental<br />
implants. It also had the contact address.<br />
The fifth homepage linked “PRODUCTS” to a webpage<br />
containing introductory paragraphs, 5 implants<br />
icons, and icons labeled “NEW PRODUCTS” and<br />
“INSTRUMENTS COMMON TO IMPLANTS”.<br />
The sixth homepage linked “PRODUCTS” to a<br />
webpage containing introductory paragraphs, 7<br />
icons for implants and implant related materials, and<br />
icons labeled “IMPLANT TRAINING”, “CONCEPTS”,<br />
“SOLUTIONS FOR INDICATION”, “CASES AND<br />
SOLUTIONS” “PRODUCTS”, “SCIENTIFIC EVIDENCE”<br />
“INDIVIDUALIZED PROSTHETICS”, “DIGITAL<br />
DENTISTRY”, “ EDUCATION AND EVENTS”, “SCIENCE<br />
AND ENOVATION” “CLINICAL MANUAL”, “SHOP<br />
ONLINE” “PRODUCT QUICK LINKS” and “DIGITAL<br />
PRECISION” ICONS.<br />
The final webpage homepage linked “PRODUCTS” to a<br />
webpage containing an introductory paragraph, a drop<br />
down-list of countries, to locate choose local markets<br />
and one icon leading to “CAD CAM”<br />
Finding a network of local users<br />
Three homepages provided this service by icons labeled<br />
as “LOCATE A DOCTOR” icon in a drop-down list from<br />
“PATIENTS’ RESOURCES”, “FIND A DENTIST” in the drop<br />
down-list from “PATIENTS”, and “LABORATORIES” in the<br />
drop down-list from “PROGRAMS”<br />
Support<br />
Labels used by icons leading to this material were<br />
“PRODUCTS AND SERVICES”, “COSTUMERS SUPPORT”,<br />
“COSTUMERS’ SERVICES”, “TECHNICAL HELP”,<br />
“TECHNICAL SERVICE”, “ENGINEERING SERVICES” icon for<br />
designers, “ADVISORY BOARD” and a “RETURN POLICY”<br />
Interaction<br />
Homepages provided some interaction with the<br />
consumers by asking for Feedback and interaction in<br />
icons labeled “COMMENT” and “MAKE AN INQUIRY”,<br />
“HELP”, and “ADVISED CONTACTS” icons. Search boxes<br />
and Sitemaps helped online interaction with the web<br />
content of subsequent pages.<br />
Signups<br />
Membership applications were present by icons, as<br />
well as “SIGNUP FOR AN E-BULLETIN” and “E-NEWS<br />
LETTER”. One homepage had “POD CASTS” and<br />
multiple “WEB CASTS” to sign up for.<br />
Sum of links per Category<br />
Webpages obtained in this sample, contained a sum of<br />
93 informative icons, 64 services and support icons and<br />
85 educative icons, after excluding the icons related to<br />
legal and <strong>copy</strong>right notes, not relevant to the study.<br />
Three webpages could be described as comprehensive,<br />
including icons leading to all categories under study.<br />
They linked to 78, 57 and 42 different webpages<br />
respectively. One webpage (117 icon links) lacked icons<br />
for the essential educational category on its homepage.<br />
Interested groups which may find relevant material<br />
Patients, general dental practitioners and technicians<br />
could be considered conventional users of these<br />
webpages. They would seem to benefit the most as the<br />
majority of the icons, relevant to the three categories<br />
under study, were directed to this group.<br />
However, some icons and content of the homepages<br />
were found to meet the interest of: Periodontists,<br />
Surgeons, Prosthodontists, CAD CAM users, Esthetic<br />
dentists, and Radiologist. These included a few, highly<br />
specific, line of products or highly specialized techniques.<br />
Other dental professions as researchers, reviewers of<br />
systematic reviews, evidence seekers, academicians and<br />
| 20 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011
students could find a share of the interest, but indirectly; as<br />
there are no dedicated icons addressing their specific needs.<br />
Unusual interests were met, but with a few number<br />
of icons, for the general public, dental administrative<br />
workers, treatment seekers or tourists, investors, the<br />
press, internet link seekers, internet bloggers, web page<br />
developers, designers and inventors.<br />
Discussion<br />
The methodology developed in this study<br />
This study is the first – within the knowledge of the<br />
author- which studies the dental implant manufacturers’<br />
webpages from this angle. The necessity for categorizing<br />
materials linked from the webpages and presenting<br />
this work comes from a previous study where there<br />
was a need to scan all available lists of dental implant<br />
manufacturers to compare implant–abutment interfaces<br />
and its mechanics. The researchers were faced by the<br />
huge variability of webpages and the confusion in the<br />
labels of icons, leading to different materials each time.<br />
Of a total of 150 webpages, the gathered experience<br />
was sufficient to develop the methodology for this study,<br />
and be presented to the reader who will face such<br />
confusion when doing any search for multiple implant<br />
systems for any reason.<br />
Educative material was the focus of this study as<br />
educating possible users increase their confidence and<br />
provide them with sufficient evidence as required for high<br />
quality treatments. This methodology can be repeated to<br />
study any dental or medical product or service providers’<br />
webpages to describe and develop recommendations for<br />
their content.<br />
The role of implant manufacturers’ webpages<br />
Implant manufacturers’ have developed their webpages<br />
to become a rich niche. Attracting the users or potential<br />
users to longer sessions of webpage viewing and surfing<br />
would indirectly help making the implant system familiar<br />
to visual and comprehension senses. These methods<br />
include:<br />
• Developing more interactions by clickable and<br />
navigation-activated icons, makes it less boring.<br />
• Additions of whole page flashes are still limited in the<br />
sample of study, but partial flashes make the webpage<br />
appear lively.<br />
• The addition of larger numbers of icons embedded<br />
in drop-down lists and pop-out windows increase the<br />
chance of including a term, thatmeets an interest or need.<br />
The efficiency of searching sessions in targeting needed<br />
information is reached as more searches are done,<br />
more subsequent webpages are explored and refined<br />
and using correct tools as search boxes and site maps.<br />
It is guided by how the learner is motivated. 9 The use<br />
of a search box, for even the experienced, is the next<br />
immediate option, if the relevant icon of interest is not<br />
perceived directly from the homepage. So having such<br />
tool is essential. Searches usually include an average of<br />
two terms. If well studied, the webpage developers of<br />
the site would annually accumulate these search terms<br />
placed in their search boxes and add or rename their<br />
homepage icons to reflect those terms, most in demand.<br />
Customizing the contents, either to regions, languages,<br />
individual accounts, logins, memberships and icons<br />
labeled “my-*****”, may increase pertinence. Finally,<br />
including multiple links to a single target increases the<br />
chance of clicking an icon.<br />
The previous were general methods used by most<br />
webpages of the study. Three webpages were considered<br />
comprehensive as they used more methods to attract<br />
the surfer. They used multiple icon formats, leading to a<br />
single page as a way of overcoming variability present<br />
in internet experience of surfers. Attracting casual users<br />
by images, flashes, and videos seems logic and was<br />
used. Also including quick link bars in the header,<br />
footer, and the side, would increase the chance of hitting<br />
relevant information. Repeating those quick link bars<br />
in subsequent pages makes the surfer oriented. Having<br />
a site map has also this effect. Assigning sections in<br />
the webpage, for each of the conventional users, and<br />
concentrating their relevant links in that area, are even<br />
more methods used.<br />
Are the implant manufacturers’ webpages informative?<br />
Looking at the homepage only, the direct answer to this,<br />
is no!. There is a very limited number of paragraphs that<br />
could add to the information of the surfer. These are<br />
limited to welcome notes, very short sentences displaying<br />
the company’s logo, or introductory paragraphs either to<br />
the company or implant system used.<br />
But when clicking icons for educative, informative, and<br />
supportive or service providing materials, opening each<br />
single webpage which is present one-click away could<br />
answer some of that need. The action of webpages acting<br />
as good directories should also be balanced with the<br />
limitation that most users have, which is that they click no<br />
more than only two pages away. So it is essential to have<br />
the actual information, one or two-clicks away, at best.<br />
Examples of this suggested confusion were for the<br />
icons “NEWS”, “EVENTS”, “PRESS RELEASE” and<br />
“PRODUCTS”. The subsequent pages were variable.<br />
Some did not include enough information, but only<br />
adding a new list of icons to be searched. Others include<br />
icons which may seem to be essential, but hidden from<br />
the homepage. If taking the classification of categories<br />
used in this study as a reference, some information in the<br />
subsequent pages was under un-expected icons labels,<br />
mixing the needs, and adding to the confusion of surfer.<br />
Opening the subsequent page was essential for another<br />
reason. Many of the terms used in the labels of icons<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011| 21 |
were not clear, and only after opening the next page,<br />
was the meaning explored. Many icon labels, which<br />
seemed to be synonyms, were not used as such. So there<br />
is a need for a standardized labeling method.<br />
Are the implant manufacturers’ webpages educative?<br />
To answer this critical question, levels of education are<br />
separated, in the following discussion.<br />
Patients’ education material<br />
Retention of dental information is enhanced by the net 10<br />
and consumers look for health care information online. 11<br />
using the net by patients was to change dentists,<br />
travel, discuss treatment with their dentists, ask for<br />
more explanations, which may be considered by some<br />
clinicians to be a burden on valuable clinical time. But<br />
this had, in some occasions, led to patients demanding<br />
inappropriate care or more complex treatment, if the<br />
information is not validated. 12<br />
Educating this group is essential, by providing an<br />
abundance of scientifically valid material in reliable<br />
resources, rather than the subjective material, limited<br />
in experience and disseminated in chat rooms and<br />
unspecialized forums.<br />
Implant webpages provide material for patients in many<br />
forms. Introductory into implants, implant treatment<br />
options, what is expected from the treatment and<br />
brochures and leaflets. Customization of the material<br />
is done in a few webpages, where language is selected<br />
by the patient. Services follow, leading patients to<br />
doctors who use their system, testimonials and stories<br />
of who had a chance to get them done, ” BEFORE AND<br />
AFTER” images, and ”PATIENT VIDEOS”. All of these are<br />
minimally educative-informative icons. Better educative<br />
resources are expected in labeled icons: “FREQUENTLY<br />
ASKED QUESTIONS” “DENTAL GLOSSARY”, “PATIENT<br />
EDUCATION”, “GUM DISEASE”, ”RESTORATIONS”,<br />
“PATIENTS’ SITE”, and these are present as icons in<br />
more comprehensive webpages. These were present in a<br />
limited number of webpages.<br />
Undergraduate dental surgeons, hygienists,<br />
assistants, and technician students<br />
For this group, internet is now promoted to be an<br />
education recourse and assistant to conventional methods.<br />
Students had responded by accepting it, retaining<br />
more information by it, and considering it an essential<br />
adjunctive to conventional methods. 13,14 Providing the<br />
material through a central location for e-resources, and<br />
be connected to wider geographical distributions as by<br />
podcasts, significantly increased their interest. 15<br />
Student preferences were then announced by many<br />
studies about what should the material look like on the<br />
net, to consider it educative. Material is preferred to be<br />
accessed off-campus, 16 standardized in terms of labels<br />
and format, outlined in an e-syllabus, 17 and visually<br />
perceived. Illustration methods are preferred in the forms<br />
of “SLIDE GALLERIES”, “SLIDE SERIES” and streaming<br />
videos. High quality images or videos were preferred if<br />
supported by the DSL connection, contained sound and<br />
text subtitles, short, and embedded in the text. 18 Online<br />
quizzes produced variable response. Such inclusions<br />
produced greater interaction, motivation and knowledge<br />
retention. 19-21<br />
As previous experience with online material is confounding<br />
factor to this group, 22 material provided should have simple<br />
interactions to reach needed information.<br />
The introduction of dental implants into the curriculum<br />
of these undergraduate courses has been reliant on<br />
text books and lecture notes. The role of dental implant<br />
webpages in providing educative material to these<br />
groups is anticipated but not met directly as the student<br />
is faced with no icons relevant to their needs. They could<br />
access some of the patient materials, but would not<br />
be able to comprehend all the professional terms and<br />
specialized techniques for technician and professional<br />
sections. Simple terminologies, more illustrated<br />
techniques and well labeled icons could be areas of<br />
further advancement towards being more educative.<br />
Schools that adopt teaching comprehensive treatment<br />
planning and team approach therapies, in final years,<br />
are faced with bit more difficulty. The reliance on<br />
experienced educators increases, to guide the students<br />
through their pile of accumulating study materials. The<br />
level of depth varies, in these approaches, according<br />
to the dental school plans. The educators may face the<br />
problem of introducing the current systems, using any of<br />
the material provided by the implant webpage as they<br />
are insufficiently directed from the homepage icons,<br />
and may lack comparative clinical studies leading to<br />
conclusions from the experience.<br />
<strong>Dental</strong> education<br />
Professional development materials are present in<br />
many dental implant manufacturer webpages. Different<br />
levels of specialty are also present but the problem is<br />
faced where many of the intended material is present<br />
in subsequent webpages, which may not be clear and<br />
explored by the homepage icons. If the item is not<br />
present, then facilities as site maps and search boxes<br />
are the next choice. Some users often go straight to the<br />
search feature on a site when it is present even before<br />
searching the icons of the homepage. 23<br />
This richness meets the definitions of a dental portal but also<br />
the definition of power searching; process of finding good<br />
quality information from the web as quickly and as easily<br />
as possible. 24 But scientific validity and level of evidence<br />
produced in these webpages warrant more research.<br />
| 22 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011
A side missing from these webpages is the retrieval<br />
of implants in cases of failure. 25 Only one webpage<br />
provided a return policy. Presence of such material<br />
or through communication with a suggested list of<br />
experienced clinicians, can aid in reducing the more<br />
stressful aspects of implant dentistry.<br />
Limitations of the study<br />
1. It is a study of only the first homepage as it is<br />
considered here as the first window which should<br />
guide the browser to their specific knowledge needs.<br />
2. The use of synonyms could not be concluded. There<br />
are no references for the number and use synonyms<br />
that may indicate a single subject. These are<br />
collectively added to the lists but those that were felt to<br />
be different were separated.<br />
3. This research should mandatory be repeated, using<br />
this methodology, but studying the webpages one or<br />
two pages away from all homepage icons. This would<br />
give a better insight to the answer of this study’s<br />
question. e.g products may lead to a catalogue,<br />
download material can lead to scientific literature<br />
or catalogues. So even the lack of the icons leading<br />
to some category materials, may not necessarily be<br />
inferring their lack from the whole page.<br />
4. The scientific validity of educative material and the<br />
level of evidence provided by them have not been<br />
verified. The material could be highly reliable if<br />
produced from systematic reviews and randomized<br />
clinical trials, or less reliable if concluded from case<br />
studies, non-controlled short term studies. Better<br />
scientific referencing of information is required.<br />
5. It is recommended for quality assurance bodies to<br />
mark presented materials according to the level of<br />
evidence.<br />
6. There is lack in educative materials for students<br />
although they could share the regular interest on<br />
sections of FAQ or introduction to but labeling a<br />
section for students would seem reasonable.<br />
Conclusions<br />
Richness in the webpages provided by dental implant<br />
manufacturers meets the need for many. However,<br />
scientific validity and level of evidence produced in these<br />
webpages warrant more research. Better referencing<br />
of educative material is required. Student educative<br />
materials are lacking.<br />
Acknowledgement<br />
The author would like to acknowledge the Deanship of<br />
Research in Jordan University of Science and technology<br />
for funding multiple <strong>Dental</strong> Implant researches, from<br />
which the experience had accumulated to perform this<br />
study. And would thank colleagues at the faculty of<br />
Dentistry for in depth discussions and cooperation.<br />
References<br />
1. Mattheos N, Stefanovic N, Apse P, Attstrom R, Buchanan J, Brown P,<br />
et al. Potential of information technology in dental education. Eur J<br />
Dent Educ. 2008;12:85-92.<br />
2. Bufano Ub, Branch-Mays G, Gilliam J, Romberg E. An Online<br />
Multimedia Treatment Planning Tool: Effect On <strong>Dental</strong> Students’<br />
Knowledge In Using Standardized Clinical Data. J Dent Educ.<br />
2010;74:50-7.<br />
3. Cook DA, Levinson AJ, Garside S, Dupras DM, Erwin PJ, Montori<br />
VM. Internet-based learning in the health professions: a metaanalysis.<br />
JAMA. 2008;300:1181-96.<br />
4. Schleyer TK, Dodell D. Ajuwon, Grace A. Continuing dental<br />
education requirements for relicensure in the United States. J Am<br />
Dent Assoc. 2005;136:1450-6.<br />
5. Sanchez Dils E, Lefebvre C, Abeyta K. Teledentistry in the United<br />
States: a new horizon of dental care. Int J Dent Hyg. 2004;2:161-4.<br />
6. Schleyer TK, Corby P, Gregg AL. A preliminary analysis of the dental<br />
informatics literature. Adv Dent Res. 2003;17:20-4.<br />
7. Song M, Spallek H, Polk D, Schleyer T, Wali T. How information<br />
systems should support the information needs of general dentists<br />
in clinical settings: suggestions from a qualitative study. BMC Med<br />
Inform Decis Mak. 2010;10:7.<br />
8. Schleyer T, Spallek H. An evaluation of five dental Internet portals. J<br />
Am Dent Assoc. 2002;133:204-12.<br />
9. Grimes EB. Student perceptions of an online dental terminology<br />
course. J Dent Educ. 2002;66:100-7.<br />
10. Patel JH, Moles DR, Cunningham SJ. Factors affecting information<br />
retention in orthodontic patients. Am J Orthod Dentofacial Orthop.<br />
2008;133:S61-7.<br />
11. Schleyer TK, Spallek H, Torres-Urquidy MH. A profile of current<br />
Internet users in dentistry. J Am Dent Assoc. 1998;129:1748-53.<br />
12. Ní Ríordáin R, McCreary C. <strong>Dental</strong> patients’ use of the Internet. Br<br />
Dent J. 2009;207:583-675.<br />
13. Patel JH, Moles DR, Cunningham SJ. Factors affecting information<br />
retention in orthodontic patients. Am J Orthod Dentofacial Orthop.<br />
2008;133:S61-7.<br />
14. Al-Jewair TS, Azarpazhooh A, Suri S, Shah PS. Computer-assisted<br />
learning in orthodontic education: a systematic review and metaanalysis.<br />
J Dent Educ. 2009;73:730-9.<br />
15. Barley SR. Computer-based distance education: why and why not.<br />
The Educational Digest 1999;65:55-9.<br />
16. Grimes EB. Student perceptions of an online dental terminology<br />
course. J Dent Educ. 2002;66:100-7.<br />
17. McCann AL, Schneiderman ED, Hinton RJ. E-teaching and learning<br />
preferences of dental and dental hygiene students. J Dent Educ.<br />
2010;74:65-78.<br />
18. Boberick KG. Creating a web-enhanced interactive preclinic<br />
technique manual: case report and student response. J Dent Educ.<br />
2004;68:1245-57.<br />
19. Fleming DE, Mauriello SM, McKaig RG, Ludlow JB. A comparison<br />
of slide/audiotape and Web-based instructional formats for<br />
teaching normal intraoral radiographic anatomy. J Dent Hyg.<br />
2003;77:27-35.<br />
20. Pilcher ES. Students’ evaluation of online course materials in fixed<br />
prosthodontics: a case study. Eur J Dent Educ. 2001;5:53-9.<br />
21. Eynon R, Perryer G, Walmsley AD. <strong>Dental</strong> undergraduate<br />
expectations and opinions of Web-based courseware to<br />
supplement traditional teaching methods. Eur J Dent Educ.<br />
2003;7:103-10.<br />
22. Gallagher JE, Dobrosielski-Vergona KA, Wingard RG, Williams<br />
TM.Web-based vs. traditional classroom instruction in gerontology:<br />
a pilot study. J Dent Hyg. 2005;79:7.<br />
23. Ross NCM, Wolfram D. End User Searching on the Internet: An<br />
Analysis of Term air Topics Submitted to the Excite Search Engine. J<br />
Amer Soc Inform Sci. 2000;51:949-58.<br />
24. Spink A, Wolfram D, Jansen MBJ, Saracevic TJ. Searching The<br />
Web: The Public and Their Queries. Amer Soc Inform Sci Tech.<br />
2001;52: 226-34.<br />
25. Toffler M. A dose of implant reality. State Dent J. 1999;65:28-32.<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011| 23 |
CANAD<br />
AN GREEN SOLUTIONS<br />
INC.<br />
Premier provider of cleaning and sanitation equipments utilizing ozone technology<br />
Presents:<br />
FOR THE FIRST TIME IN MIDDLE EAST<br />
WHO USES OPURA?<br />
HEALTHCARE PROFESSIONALS FOOD SERVICE CONSUMERS<br />
• Doctors<br />
• Nurses<br />
• Dentists<br />
• Eldercare care givers<br />
OPURA FACTS<br />
100% GREEN SOLUTION<br />
• Sanitizers without use of harsh<br />
antibacterial soaps and chemicals<br />
• Zero environmental impact<br />
THE BACTERIA TERMINATOR<br />
• OPURA kills 99.99% of bacteria on contact<br />
ozone is nature’s most powerful sanitizer.<br />
• 50 times more powerful than chlorine<br />
• 3,000 times faster acting<br />
PROVEN EFFECTIVE AGAINST:<br />
• e.Coli<br />
• C. difficile<br />
• H1N1 (Swine Flu)<br />
• Hepatitis A, B, C<br />
• Salmonella<br />
• Listeria<br />
... and hundreds of others.<br />
• Food processors<br />
• Restaurants<br />
• Grocery stores<br />
• Homes<br />
• Baby care<br />
• Produce wash<br />
• Hard surface sanitizer
di VILLA<br />
AEEDC 2012<br />
Booth 312<br />
RAFFAELLO<br />
ViVi s.r.L. - Via Dei Lavoratori, 3/K - Buccinasco, Italy<br />
Tel. (+39) 02 45703068 - Fax (+39) 02 45703463<br />
www.vivi-italy.it - vivi@vivi-italy.it<br />
Middle East Area Manager<br />
Mahmoud Lutfi<br />
P.O.Box 641 11941 Amman Jordan<br />
Tel: +962 6 5656404/5<br />
Mobile: +962 7 95536867<br />
Email: vivi@m-lutfi.com
Solving TMJ Problems with Orthodontic<br />
Treatment and Cosmetic Mouth Rehabilitation<br />
Case Series<br />
Leonid Rubinov<br />
DDS, PhD<br />
• Instructor of the International<br />
Association for Orthodontics<br />
• Fellow of the American<br />
Association for Functional<br />
Orthopedics<br />
• Clinical Professor of the<br />
International Department of<br />
NYU’s College of Dentistry,<br />
USA<br />
drrubinov@yahoo.com<br />
Abstract<br />
TMJ disorder is considered a gray area of dentistry. Treatment of these types of<br />
problems with TMJ splints is often a temporary solution. Achieving a permanent<br />
correction is usually difficult, because it requires changing the position of mandibular<br />
condyles inside a TM joint. In many cases this goal is unattainable using only one<br />
treatment modality. The unique treatment philosophy described in this article requires<br />
a multidisciplinary approach. It starts with orthodontic treatment which enhances the<br />
relationship inside the TM joint, alleviates TMJ symptoms and sets the stage for further<br />
full mouth rehabilitation, if necessary. Orthodontic treatment in these cases is performed<br />
with special attention to dentofacial orthopedics. The end result of this treatment<br />
creates improved position of condyles inside TMJ, proper three dimensional orthopedic<br />
relationships between the patient’s jaws and correct occlusion. This produces greatly<br />
improved facial proportions, enhanced facial appearance and youthful look of the<br />
patient while laying the groundwork for more successful restorative procedures.<br />
Keywords: TMJ, Orthodontic treatment, Cosmetic rehabilitation, Dentofacial orthopedics.<br />
Introduction<br />
TMJ disorder is considered a gray area of dentistry. According to LeResche, 1 “Overall,<br />
it is estimated that approximately 10% of population over the age of 18 years have<br />
pain in the TMJ region”. 1 There are a lot of uncertainty and different opinions what<br />
is causing the TMD, how to treat it and even if any treatment required at all. After<br />
reviewing literature Luter, 2 Luter and others 3 did not find enough evidence to support<br />
or refute the use of orthodontic therapy for the treatment of temporomandibular<br />
disorders (TMD). Meanwhile, it has been suggested that an internal derangement and<br />
TMJ symptoms may be caused by the mandible being trapped and retracted behind<br />
maxillary front teeth, forcing the TM disc anteriorly due to the condyles having been<br />
forced posteriorly. 4 Treatment of TMD with different types of TMJ splints is a temporary<br />
solution. It is suggested that a permanent occlusal orthodontic treatment to be used<br />
after a change in the position of the mandible after repositioning-stabilization splints. 5<br />
In his articles Brenkert, 6,7 described different choices for orthodontic treatment for the<br />
anterior repositioned splint stabilized patients following anterior disk (s) displacement.<br />
He outlined of how to properly treat these patients to consistent stabilized occlusion<br />
compatible with the TMJ splint position. DeSteno 8 discussed stabilization and<br />
rehabilitation principles of the therapy of the patients after TMJ splints, emphasizing<br />
prosthodontic and orthodontic perspective.<br />
The goal of this article is to lay out the framework for a unique treatment philosophy.<br />
An interdisciplinary approach, starting with dentofacial orthopedic and orthodontic<br />
treatment, allows the dentist to focus on proper arrangements inside TMJ. Changing<br />
the size of the Maxilla is giving the dentist an opportunity to advance Mandible down<br />
and forward, thus improving position of condyles and alleviating the majority of TMJ<br />
symptoms. It is also is setting up condition for a much better restorative phase of the<br />
treatment and usually improving facial appearance of the patient too.<br />
The cases presented in this article can be seen as an illustration of how the<br />
interdisciplinary approach can help in solving TMJ issues. Orthodontic treatment in<br />
| 26 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011
the beginning, with special attention to dentofacial<br />
orthopedics, will place teeth and jaws in a position that<br />
ensures the improved relationships inside TMJ and the<br />
successful completion of the subsequent prosthetic phase<br />
of the patient’s full mouth rehabilitation and greatly<br />
improve the overall esthetic result.<br />
Case 1<br />
Patient O., 40 years old presented with several concerns<br />
about her smile (figs. 1, 2): her front teeth are too<br />
vertical, gummy smile, cosmetically unpleasant prosthetic<br />
restorations (fig. 3).<br />
She also had numerous TMJ symptoms such as: “tension”<br />
headaches, headaches in right and left temple areas and<br />
back of her head. She had frequent neck aches, difficulty<br />
of opening her mouth wide, clicking sounds in her joints<br />
and ringing sounds in her ears. She was grinding her<br />
teeth at night and had pain in her TM joints.<br />
Clinical and X ray evaluations showed, that patient had<br />
Class II malocclusion, with her front maxillary teeth in<br />
vertical, almost retrusive position, trapping her mandible<br />
distally (fig. 4).<br />
Distally displaced position of the mandible pushed<br />
patient’s condyles into posterior/ superior position, thus<br />
causing abovementioned TMJ symptoms.<br />
(Figs. 1 & 2) Facial view & Natural smile of the patient O.<br />
before treatment<br />
(Fig. 3) Retracted view of the patient smile before treatment<br />
The objective of the treatment plan for this patient<br />
was to advance her mandible down and forward,<br />
thus improving her appearance and eliminating TMJ<br />
problems. Expansion of Maxilla along with protrusion<br />
of maxillary incisors forward was necessary in order to<br />
achieve required advancement of mandible.<br />
These objectives were accomplished in 4 months of<br />
treatment by using 3-Way Sagittal Removable Appliance<br />
(fig. 5).<br />
Upper and lower braces were placed in order to move teeth<br />
into best possible positions for future restorative treatment.<br />
At the end of this stage of the treatment skeletal changes<br />
in patient’s face and jaws were obvious (fig. 6).<br />
Positions of the condyles inside TMJ also changed,<br />
helping alleviate and eliminate most of her TMJ<br />
symptoms (figs. 7, 8).<br />
(Fig. 4) Cephalometric X ray before treatment<br />
Restorative part of the treatment was performed after<br />
completion of orthodontic phase. Zirconia crowns were<br />
placed on teeth #7, #10, #12, #13, #14, #19, #20,<br />
#21, #28 and #29. Porcelain veneers were place on<br />
teeth #4, #5, #6, #8, #9 and #11. (figs 9-11)<br />
The final results of the treatment may be described as<br />
a triple effect:<br />
First: Patient’s TMJ symptoms have completely disappeared,<br />
allowing her pain free and symptoms free existence.<br />
(Fig. 5) Retracted view after treatment with removable appliance<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011| 27 |
Second: Patient’s facial appearance improved<br />
dramatically, providing her with much more balanced,<br />
proportional and youthful look.<br />
Third: Her smile got better with new esthetically pleasing<br />
restorations, better functional occlusion and eliminations<br />
of gummy smile.<br />
Case 2<br />
Patient I., 33 years old, (fig. 12) came to the office with<br />
several TMJ symptoms such as: “tension” headaches,<br />
headaches in front of her head. She had frequent neck<br />
aches, stiff neck, clenched her teeth during day and<br />
night and was grinding her teeth at night.<br />
Clinical evaluation showed, that patient had Class II<br />
malocclusion with deep overbite and large overjet, placing<br />
her condyles in superior/posterior position (figs. 13, 14).<br />
(Fig. 6) Cephalometric X ray after the treatment<br />
The objective of the treatment plan for this patient was, like<br />
with patient in case 1, to advance her mandible down and<br />
forward, thus improving her appearance and eliminating<br />
TMJ problems. Expansion of maxilla was necessary to<br />
achieve required advancement of mandible. This goal<br />
(fig.15) was achieved by using fixed orthopedic appliance.<br />
(Fig. 7) Transcranial X-ray of<br />
left TMJ before treatment<br />
(Fig. 8) Transcranial X-ray of<br />
left TMJ after treatment<br />
Further orthodontic treatment, using braces and<br />
functional appliances, allowed advancing mandible<br />
down and forward, effectively placing condyles in proper<br />
position inside TMJ.<br />
Fabrication of two 3-unit Zirconia bridges to replace<br />
missing first mandibular molars and support newly<br />
established occlusion complete the restorative part of the<br />
treatment.<br />
The final result of the treatment of this patient was<br />
similar to the patient in case 1: Patient’s TMJ symptoms<br />
were eradicated, patient’s facial appearance changed<br />
pretty drastically (fig. 16) and her occlusion improved by<br />
eliminating overbite and overjet (figs. 17, 18).<br />
(Figs. 9 & 10) Facial view & Natural smile after treatment<br />
(Fig. 11) Retracted view of the patient smile after restorative phase<br />
Discussion<br />
The interdisciplinary treatment of the patients with<br />
TMJ problems is difficult to accomplish due to the<br />
complexity of maintaining acquired mandible position,<br />
which is achieved through its anterior reposition. The<br />
prevailing treatment philosophy in general dentistry and<br />
orthodontics is based on assumption of immovability of<br />
the alveolar bone after the development of dentoalveolar<br />
complex is completed and the permanent teeth have<br />
erupted. This kind of approach is making the goal of<br />
permanently repositioning the mandible downward and<br />
forward is impossible to achieve in many TMJ cases due<br />
to size and position of maxilla. To the contrary, the new<br />
treatment philosophy with special attention to dentofacial<br />
orthopedic, described in this article, results in an<br />
accomplishment of above-mentioned reposition of the<br />
mandible. The new orthopedically improved occlusion<br />
| 28 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011
(Fig. 12) Facial view of<br />
patient I. before treatment<br />
(Fig. 16) Facial view of<br />
patient I. after treatment<br />
(Fig. 13) Retracted view before treatment<br />
(Fig. 17) Retracted view after treatment<br />
(Fig. 14) Retracted view<br />
of left side occlusion before<br />
treatment<br />
(Fig. 18) Retracted view<br />
of left side occlusion after<br />
treatment<br />
(Fig. 15) Maxillary models before and after orthodontic phase<br />
of treatment<br />
is creating proper relationships inside TMJ, subsequently<br />
eliminating the majority of TMJ issues.<br />
a dentofacial orthopedics approach regardless of age<br />
of the patient. The changes undergone by patient’s<br />
faces, the size of the jaws and the occlusion and teeth<br />
position cannot be explained by simple tooth movement<br />
but rather by response of the alveolar bone as a<br />
“whole”. Orthopedic changes in patient’s jaws and<br />
their relationships are generally responsible for overall<br />
improvement in facial appearance, correlations of the<br />
condyles and discs inside TMJ and the creation of much<br />
better groundwork for subsequent restorative procedures.<br />
The scientific evidence for the new dentofacial orthopedic<br />
approach is coming from work of Melsen, 9,10 and<br />
Cacciafesta, 11 who advocate that the dentoalveolar<br />
complex is much more malleable than previously believed.<br />
Michael O. Williams and Neal C. Murphy have introduced<br />
the concept of “whole bone” perspective to the alveolar<br />
bone response to continuous low orthopedic force. 12<br />
The cases presented in this article show that the<br />
remodeling and redevelopment of the patient’s facial<br />
and dentoalveolar structures can be performed using<br />
(Fig. 19) Patient’s O. CT scan: maxillary transverse view after<br />
treatment<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011| 29 |
Patient O. from case 1 has undergone CT scan examinations<br />
several months after the completion of the treatment. The<br />
goal of this research was to evaluate the long term effect of<br />
the completed interdisciplinary treatment on the condition<br />
and integrity of the alveolar bone and on the position and<br />
stability of the roots of the teeth within the bone. An image<br />
from this examination can be seen in fig. 19.<br />
The assessments of this and other images for this patient<br />
are consistent with the picture of normal alveolar bone<br />
with roots of the teeth positioned proportionally within<br />
the boundaries of the bone. There is no visible damage,<br />
dehiscences or fenestrations in the buccal alveolar plate and<br />
no bone loss can be observed.<br />
These CT scans illustrate the “whole bone” remodeling<br />
response to successfully performed orthopedic and<br />
orthodontic treatment.<br />
Conclusion<br />
The addition of the orthodontic treatment to interdisciplinary<br />
approach to solve TMD can result in permanent resolution of<br />
the patient’s TMJ issues. The final outcome of this treatment<br />
results in much improved position inside TM joints, significant<br />
enhancement of the patient’s overall facial appearance,<br />
occlusion, function and esthetic aspects of the smile. This<br />
treatment philosophy gives the dentist an opportunity to<br />
assess patients in a different way. The ensuing orthodontic<br />
treatment with special attention paid to dentofacial<br />
orthopedics allows for the remodeling of a patient’s alveolar<br />
bone and whole dentoalveolar complex. The bone movement<br />
creates a proper orthopedic relationship between the jaws<br />
with stable results and healthier TMJ. The implementation<br />
of this phase of the treatment places teeth and jaws in the<br />
position that dramatically improves the dentist’s ability<br />
to perform its restorative part. The overall results of the<br />
treatment are elimination of the majority of TMJ problems,<br />
much improved facial appearance, youthful look and proper<br />
occlusion allowing for better patient’s functional ability and<br />
esthetically attractive smile.<br />
References<br />
1. LeResche L. Epidemiology of temporomandibular disorders: implications for the<br />
investigation of etiologic factors. Crit Rev Oral Biol Med. 1997;8:291-305.<br />
2. Luter F. TMD and occlusion part I. Damned if we do? Occlusion: the interface<br />
of dentistry and orthodontics. British <strong>Dental</strong> <strong>Journal</strong>. 2007;202:E2.<br />
3. Luter F, Layton S, McDonald F. Orthodontics for treating temporomandibular<br />
joint(TMJ) disorders (Review). 2010 The Cochrane Collaboration.<br />
4. Wyatt W.E. Preventing adverse effects on the temporomandibular joint through<br />
orthodontic treatment. Am J Orthod Dentofacial Orthop. 1987;91:493-9.<br />
5. Capurso U, Marni I. Orthodontic treatment of TMJ disc displacement with<br />
pain: an 18 year follow-up. Prog Orthod. 2007;8(2):240-50.<br />
6. Dennis R. Brenkert. Orthodontic treatment for the TMJ patient following splint<br />
therapy to stabilize a displaced disk(s): a systemized approach. Part I, TMJ<br />
orthodontic diagnosis. Cranio: The <strong>Journal</strong> of Craniomandibular Practice.<br />
28.3 (July 2010) p.193.<br />
7. Dennis R. Brenkert. Orthodontic treatment for the TMJ patient following<br />
splint therapy to stabilize a displaced disk(s): a systemized approach. Part II.<br />
Cranio: The <strong>Journal</strong> of Craniomandibular Practice. 28.4 (Oct. 2010) p.260.<br />
8. Desteno C V, et al.: Phase II rehabilitation of the temporomandibular joint<br />
dysfunction patient. Clin Prey Dent. 1989; 11(5):29-32.<br />
9. Birte Melsen. Biological reaction of alveolar bone to orthodontic tooth<br />
movement. The Angle orthodontist. 1999;69(2):151-6.<br />
10. Birte Melsen. Tissue reaction to orthodontic tooth movement - a new<br />
paradigm. European <strong>Journal</strong> of Orthodontics. 2001;23:671-81.<br />
11. Cacciafesta V. Dr. Birte Melsen on adult orthodontic treatment. J Clin<br />
Orthod. 2006;12:703-16.<br />
12. Michael O. Williams and Neal C. Murphy. Beyond the Ligament: A Whole-<br />
Bone Periodontal View of Dentofacial Orthopedics and Falsification of<br />
Universal Alveolar Immutability. Seminars in Orthodontics, Vol. 14, No 4<br />
(December), 2008;246-59.<br />
| 30 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011
Behind every successful<br />
implantologist is an Implantmed<br />
With the new Implantmed you perform implant procedures with<br />
maximum precision. The unit is easy to operate and guarantees longer<br />
working without fatigue – thanks to the light, yet powerful motor and the<br />
ergonomically-shaped contra-angle handpiece. And the integrated<br />
thread-tapping function helps you with especially hard bone.<br />
wh.com
Outcomes Following Zygomatic<br />
Complex Fractures<br />
A Retrospective Study<br />
Majed Hani Khreisat<br />
BDS, MSc, JBO<br />
• MSc UK<br />
• JBO in Oral & Maxillofacial<br />
surgery, Amman - Jordan<br />
majed_khreisat@hotmail.com<br />
Abstract<br />
Purpose: This is a descriptive analytic study evaluated the cause, type, incidence,<br />
complications and treatment modality of zygomatic complex fractures at Manchester<br />
Royal Infirmary in Manchester, United Kingdom over a period of six months from 10-1-<br />
2005 to 20-7-2005.<br />
Patients and Methods: This study was undertaken to investigate the outcomes following<br />
zygomatic complex fractures in the unit of Oral and Maxillofacial Surgery at Manchester<br />
Royal Infirmary, over a six month period. Information for the study was gathered from<br />
patient records and a self-administrated patient questionnaire over a period of six months<br />
from 10-1-2005 to 20-7-2005. Fifty patients, who had sustained zygomatic-complex<br />
fractures were examined clinically, radiographicaly, and also underwent orthoptic<br />
investigations. Ethical approval was gained from the local research ethics committee.<br />
Results: The age of the patients ranged from 17 to 75 years. Seventy six percent of<br />
patients were male, and the mean and median ages were (32.3; 30.5) for males,<br />
and (33.4; 30.5) for females respectively. The male to female ratio was 3:1. Assault<br />
was the major cause of zygomatic complex fractures, (35 patients [70%]), followed by<br />
sport (8 patients [16%]). The majority of assault cases were in the 24-28 age groups.<br />
The vast majority of patients (68.0%) with zygomatic complex injuries presented within<br />
24 of their injury to the Accident & Emergency department, 15 cases (30%) presented<br />
between 1-3 days, and only one case (2%) attended between 4-7 days. Patients<br />
presented with circum-orbital ecchymosis as the most common sign, which was evident<br />
in 41 patients (82%). Infra-orbital paraesthesia was present in 38 patients (76%). Subconjunctival<br />
haemorrhage was seen in 33 patients (66%). Flattening of the cheek was<br />
present in 28 patients (56%). Epistaxis occurred in 23 (46%) of patients. Step deformity<br />
of the infra-orbital rim and deformity at Z-F suture were present in 36%, and 38%<br />
of patients, respectively. Thirty-six percent of patients had limitation of mandibular<br />
movements. Nine cases out of fifty (18%) presented with diplopia. Surgical treatment<br />
was provided for 36 patients (72%). Fourteen (28%) of patient were observed and<br />
treated conservatively. Closed reduction was performed for 42% of the treatment group<br />
and 19 fractures were reduced by the Gillies temporal approach and 2 fractures via a<br />
buccal approach; 30% of the fractures were reduced by open reduction and internal<br />
fixation and the orbital floor was investigated in 15 patients. Ten patients required<br />
orbital floor reconstruction and the preferred alloplastic material in this patient group<br />
was Vicryl mesh (40%). The most common incision to explore the orbital floor is the<br />
subciliary incision which was utilised in 9 patients the lateral brow incision was utilised<br />
in 4 patients (27%). And two patients (11.8%) had the trans-conjunctival approach.<br />
Statistically analysis revealed a significant difference between assault as the aetiology<br />
and the types of zygoma fracture (p
Introduction<br />
Zygomatic or Malar bone fractures are (2 nd most<br />
common) after nasal bone fractures among facial<br />
skeletal Injures. 1,2 The high incidence of these fractures<br />
may probably be attributed to the fact that Zygoma’s<br />
occupy an anatomically prominent position within the<br />
facial skeleton which frequently exposes it to traumatic<br />
forces. The prominent convex shape of the zygoma<br />
makes it vulnerable to traumatic injury. Even minimally<br />
displaced zygomatic-complex fractures can result in<br />
functional and aesthetic deformities. All traumas to the<br />
face, particularly above the level of the mouth, require<br />
a careful ocular examination including an estimation<br />
of visual acuity of each eye, and zygomatic-complex<br />
fractures are frequently complicated by injury to the orbit<br />
and eye adnexae, which are the most serious negative<br />
outcomes of zygomatic complex fractures. 3<br />
Patients and Methods<br />
Information for the study was gathered from patient<br />
records and a self-administrated patient questionnaire<br />
over a period of six months from 10-1-2005 to 20-<br />
7-2005. Fifty patients, who had sustained zygomaticcomplex<br />
fractures were examined clinically, radiographicaly,<br />
and also underwent orthoptic investigations.<br />
A written informed consent was obtained from the<br />
patient or attendant. The treatment of fractures was done<br />
by standard methods of reduction and fixation. Data<br />
was analyzed in statistical program for social sciences<br />
(SPSS) version 11.0. The frequency and percentage<br />
was computed for qualitative variables, like gender,<br />
etiologies, pattern and management modalities. Mean±<br />
standard deviation was computed for qualitative<br />
Variables, like age. Ethical approval was gained from the<br />
local research ethics.<br />
Results<br />
The results of this study were described in sequence of<br />
the objectives. Detailed description of separate results is<br />
shown in figures and tables.<br />
Discussion<br />
The zygomatic complex gives the cheek prominence, and<br />
it is the second most common mid-facial bone fractured<br />
after the nasal bone and, overall, represents 13% of<br />
craniofacial fractures. 4 Zygomatic complex fractures are<br />
almost always associated with fractures of the floor of the<br />
orbit. Typically, a fracture line extends from the inferior<br />
orbital fissure antero-medially along the orbital process<br />
of the maxilla, toward the infra-orbital rim.<br />
Fifty patients attended with zygomatic complex fractures<br />
over a six months period. The age of the patients ranged<br />
from 17 to 75 years. Seventy six percent of patients were<br />
male, and the mean and median ages were (32.3; 30.5)<br />
for males, and (33.4; 30.5) for females respectively. The<br />
male to female ratio was 3:1 as shown in table 1.<br />
Age<br />
Range<br />
Number<br />
of patient<br />
Male Female Total<br />
%<br />
Number<br />
of patient<br />
Assault was the major cause of zygomatic complex<br />
fractures, (35 patients [70%]), and the second most<br />
common cause was sport (8 patients [16%]). The<br />
majority of assault cases were in the 24-28 age groups.<br />
This corresponds with results in comparable studies 5-8 as<br />
shown in figure 1.<br />
Of the patients who required surgical intervention,<br />
8 (16%) were treated within 4-7 days and 19 (38%)<br />
in 8-13 days. In 23 patients (46%) surgery was not<br />
undertaken until 14 days. The reasons for this may<br />
include allowing the oedema and ecchymosis to settle<br />
and for the general condition of the patients to improve 9<br />
as shown in figure 2.<br />
We also evaluated the site of injury to whether it was<br />
left-side or right, and compared this to aetiology of the<br />
fracture. There was a statistically significant difference<br />
between aetiologies and sites of injuries with left side<br />
%<br />
Total<br />
number of<br />
patient<br />
14-18 4 8 0 0 4 8<br />
19-23 2 4 2 4 4 8<br />
24-28 12 24 4 8 16 32<br />
29-33 5 10 1 2 6 12<br />
34-38 6 12 2 4 8 16<br />
39-43 4 8 1 2 5 10<br />
44-48 3 6 0 0 3 6<br />
Over<br />
48<br />
2 4 2 4 4 8<br />
Total 38 76 12 24 50 100<br />
(Table 1) Age and sex of study group<br />
16<br />
14<br />
12<br />
10<br />
8<br />
6<br />
4<br />
2<br />
0<br />
14-18<br />
19-23<br />
24-28<br />
29-33<br />
34-38<br />
39-43<br />
(Fig. 1) Aetiology by age distribution<br />
44-48<br />
Over 48<br />
%<br />
Total<br />
Others<br />
Industrial<br />
Road Trafic<br />
Accident<br />
Sport<br />
Fall<br />
Assault<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011| 33 |
Time from presentation to treatment<br />
4-7 days<br />
8-13 days<br />
14+ days<br />
8-13 days<br />
38.00%<br />
n=19<br />
Number of cases<br />
20<br />
18<br />
16<br />
14<br />
12<br />
10<br />
8<br />
6<br />
4-7 days<br />
16.00%<br />
n=8<br />
14+<br />
days<br />
46.00%<br />
n=23<br />
4<br />
2<br />
0<br />
Fracture of zygomatt<br />
No significant displ<br />
Comminuted fractures<br />
Orbital wall fracture<br />
Displacement en bloc<br />
Rotation around Ion<br />
Rotation around vert<br />
(Fig. 2) Time from presentation to treatment (Time of Surgical<br />
intervention)<br />
(Fig. 4) Types of zygomatic-complex fractures<br />
40<br />
50<br />
45<br />
30<br />
32<br />
40<br />
35<br />
Number of of cases<br />
20<br />
10<br />
5<br />
0 3 3 3 2<br />
Assault Fall Sport RTA Other<br />
Aetiology<br />
Site of the fracture<br />
Site of the fracture<br />
Left<br />
Right<br />
Aetiology<br />
(Fig. 3) Site of zygomatic complex fracture according to aetiology<br />
Frequency<br />
30<br />
25<br />
20<br />
15<br />
10<br />
5<br />
0<br />
Oedema<br />
Circum-orbital ecchymosis<br />
Subconjunctival haemorrhage<br />
Flattening of the cheek<br />
Limitation of mandibular<br />
movement<br />
Step deformity (infra-orbital<br />
rim)<br />
Deformity of Z-F suture<br />
Infra-orbital paraesthesia<br />
Diplopia<br />
Limitation of Orbial movement<br />
Epistaxis<br />
being commonly injured due to assault (32 patients,<br />
64%) (p
25<br />
20<br />
Orbital floor exploration<br />
Subciliary incision<br />
Transconjuctival incision<br />
Lateral brow incision<br />
15<br />
10<br />
No Treatment<br />
Lateral Brow Incision<br />
Transconjunctival Approach<br />
Subciliary Approach<br />
Both Treatments (IOR & ZFS)<br />
Zygomatico-Frontal Suture<br />
Infra-orbital Rim<br />
Buccal Sulcus Approach<br />
Gillis Temporal Approach<br />
Lateral brow<br />
incision<br />
27%<br />
n=4<br />
Subciliary<br />
incision<br />
0<br />
Closed Reduction<br />
Open Reduction<br />
& Internal fixation<br />
Orbital floor<br />
Explanation<br />
Waiting & Observation<br />
Transconjuctival<br />
incision 13%<br />
n=2<br />
60%<br />
n=9<br />
(Fig. 6) Surgical approaches to zygomatic-complex fractures<br />
(IOR: Infra-Orbital rim; ZFS: Zygomatic-frontal Suture)<br />
reported by. 19 Thirty-six percent of patients had limitation<br />
of mandibular movements, which is similar to finding<br />
in other comparable studies. Nine cases out of fifty<br />
(18%) presented with diplo. 20 Studies in the literature<br />
report similar figures. 21,22 Some studies reported a lower<br />
incidence 23 as shown in figure 5.<br />
The treatment of zygomatic-complex fractures varies from<br />
surgeon to surgeon and depends on the type of fracture<br />
and given circumstance. Surgical treatment was provided<br />
for 36 patients (72%). Fourteen (28%) of patient were<br />
observed and treated conservatively. Forty-two percent of<br />
patients underwent closed reduction by both extra oral<br />
(Gillies temporal approach) and intra-oral approach<br />
(Buccal sulcus approach). This surgical approach is<br />
comparable and well reported in several studies. 24<br />
Orbital floor exploration was undertaken in 15 (30%) of<br />
patient and our figures compared well with 25,26 who have<br />
relatively similar figures of 41.2% and 43.6% respectively.<br />
Open reduction and internal fixation was undertaken in<br />
15 cases (30%). Previously wiring at the infra-orbital rim<br />
and zygomatico-frontal suture was undertaken but with<br />
advent of plating, the majority of fractures are now with<br />
titanium plates as shown in figure 6.<br />
It was stated that adequate soft tissue access is of<br />
paramount importance for orbital floor exploration,<br />
and exposure of the fracture to stable bone for proper<br />
anatomic reduction. 27 The most common incision to<br />
explore the orbital floor is the subciliary incision which<br />
was utilised in 9 patients (60%). 28, 29 stated similar figures<br />
of 42% and 47% respectively. Some surgeons prefer the<br />
lateral brow incision as this avoid fixation at the infraorbital<br />
rim which is thin and sometimes less suitable<br />
for plating. The lateral brow incision is utilised to plate<br />
at the zygomatic-frontal suture and also for orbital<br />
floor exploration. In our study group the lateral brow<br />
incision was utilised in 4 patients (27%). Two patients<br />
(11.8%) had the trans-conjunctival approach. The most<br />
commonly stated criticism of this technique is the lack of<br />
(Fig. 7) Orbital floor exploration in zygomatic complex fracture<br />
Type of fixation<br />
PDS<br />
Medpore<br />
Vicrly mesh<br />
None<br />
None<br />
33%<br />
n=5<br />
(Fig. 8) Repair of orbital floor defects<br />
PDS<br />
20%<br />
n=3<br />
Medpore<br />
7%<br />
n=1<br />
Vicrly mesh<br />
40%<br />
n=6<br />
access to the operative field, although it provides good<br />
cosmetic results with no visible scar but can carry a low<br />
incidence of postoperative ectropion. 30 None of the<br />
patients presented with early complication as a result of<br />
the surgical approaches utilised as shown in figure 7.<br />
Several of materials have been employed by<br />
the surgeons in Manchester Royal Infirmary for<br />
reconstruction of orbital floor defects. The convenience,<br />
stability, lack of donor site morbidity, and reduced<br />
anaesthetic and operating time has persuaded many<br />
surgeons to use alloplastic materials for reconstruction<br />
of orbital floor defects. The following materials were<br />
utilised for reconstruction of the orbital floor: Vicryl mesh<br />
(6 patients, 40%): PDS was utilised in 3 patients (20%)<br />
and one patient had Medpore placed in the defect (7%).<br />
For 5 patients (33%), the orbital defect was not repaired<br />
following exploration. The early or late complications of<br />
alloplastic implant materials include infection, extrusion,<br />
migration, residual diplopia, lower eyelid oedema,<br />
ectropion and tissue reaction. 31 None of the latter<br />
complications were noted in patients in this study as<br />
shown in figure 8.<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011| 35 |
60<br />
55<br />
50<br />
45<br />
40<br />
35<br />
30<br />
Frequency 25<br />
Percentage 20<br />
15<br />
10<br />
5<br />
0<br />
Asymmetry<br />
(Cheek Flattening)<br />
Limitation mandibular<br />
movement<br />
Deformity of<br />
orbital rim<br />
Deformity of<br />
Z-F Suture<br />
Infra-orbital<br />
paraesthesia<br />
(Fig. 9) Persistent complications of zygomatic-complex fractures<br />
The most frequent complication of zygomatic complex<br />
fractures was infra-orbital paraesthesia in 27 cases<br />
(54%). This was followed by 3 cases (6%) in asymmetry<br />
(cheek flattening). Two cases (4%) had limitation of<br />
mandibular movement. Persistent diplopia and changes<br />
of visual acuity was seen in one case (2%) (fig. 9).<br />
Conclusion<br />
This study presents information that can be<br />
valuable in describing the pattern and spectrum<br />
of zygomaticomaxillary complex fractures in local<br />
population. Since the assault, the leading cause of facial<br />
trauma, are usually associated with greater severity of<br />
injuries, treatment approach needs to be comparatively<br />
aggressive e.g. exposure of fracture sites and internal<br />
fixations, for better aesthetic and functional restoration.<br />
However, the four most important considerations<br />
in treating zygomatic complex fractures are proper<br />
reduction, adequate stabilization, adequate orbital<br />
floor reconstruction (when necessary), and adequate<br />
handling/positioning of periorbital soft tissue which will<br />
provides the most accurate and satisfactory postoperative<br />
results. Variance in treatment may exist because therapy<br />
depends upon the type and severity of fracture, the time<br />
since injury, and the surgeon’s personal experience. The<br />
prognosis of zygomatic complex fractures is influenced<br />
by delay between time of injury and treatment. The<br />
timing of surgery is dependent on the general health<br />
of the patient and the presenting signs and symptoms.<br />
Ideally management of zygomatic complex injuries<br />
should be undertaken after residual oedema has<br />
subsided and a thorough pre-operative ophthalmic<br />
assessment has been performed. As revealed in this<br />
study, only 72% of patients received surgical intervention<br />
to treat their injury.<br />
References<br />
1. Hollows P, D’Sa A, McAndrew PG. Life-threatening heamorrhage<br />
after elevation of a fractured zygoma. Br J Oral Maxillofac Surg.<br />
1999;37:448-50.<br />
2. Israr N, Shah AA. Retrospective study of zygomatic complex<br />
fractures in Sheffield England. Pak Oral Dent J. 2001;21:50-9.<br />
Diplopia<br />
Loss of<br />
Visual Acuity<br />
3. Mackinnon CA, David DJ, Cooter RD. Blindness and sever visual<br />
impairment in facial fractures: An 11-year review. Br J Plast Surg.<br />
2002;55:1-7.<br />
4. Tadji Armin MB, Kimble Frank W. Fractured Zygomas. ANS. J. Surg.<br />
2003;73:49-54.<br />
5. Rowe, N.L, Killey, H.C. Fractures of the facial skeleton. Edinburgh,<br />
E & S. Livingston. Ed.1. 1955;328-59.<br />
6. Haider Z. Fractures of the zygomatic complex in the south-east<br />
region of Scotland. Br. J. Oral. Surg. 1977;15:265-7.<br />
7. Balle V, Christensen PH, Greisen O, Jorgensen PS. Treatment<br />
of zygomatic fractures: a follow-up study of 105 patients.<br />
Otolaryngolog. 1982;7:411-6.<br />
8. Telfer MR, Jones GM, Shepherd JP (1991).Trends in the aetiology of<br />
maxillofacial fractures in United Kingdom. (1977-1987). British. J.<br />
Oral & Max-Fac. Surg. 1982;29:250-5.<br />
9. Ogden GR. The Gillies method for fractured zygoma: an analysis<br />
of 105 cases. J. Oral. Max-Fac.Surg. 1991;49:23-5.<br />
10. Ellis E 3rd, el-Attar A, Moos KF. An analysis of 2,067 cases<br />
of zygomatic orbital fractures. J. Oral Max-Fac. Surg.<br />
1985;43(6):417-28.<br />
11. Cramer, L.Tooze, F., Lerman, S. Blow-out fractures of orbit. Br. J.<br />
Plast. Surg. 1965;18:171-9.<br />
12. Kristeensen S, Tvetrs K. Zygomati Fractures: Classsification and<br />
Complications. Clin. Otolarng. 1986;11:123-9.<br />
13. Larsen OD, Thomsen M (): Zygomatic Fractures. II. A Followup<br />
study of 137 patients. Scand. J. Plast. Reconstr. Surg.<br />
1978;12(1):59-63.<br />
14. Hollier, Larry H, M.D, Thornton James, M.D; Pazimiono, Pat M.D.;<br />
Stal, Samuel M.D. The Management of Orbito-zygomatic fractures.<br />
Plast Reconstr. Surgery. 2003;111(7):2386-93.<br />
15. Wiesenbaugh Josph M. Diagnostic evaluation of zygomatic<br />
complex fractures. <strong>Journal</strong> of oral surgery. 1970;28:204-8.<br />
16. Kaasted E, Freng A.Zygomatico-maxillary fractures. J.<br />
Craniomaxillo-facial Surgery. 1989;17:210.<br />
17. Carr RM, Mathog RH. Early and delayed repair of orbito-zygomatic<br />
fractures. J. Oral. Max-Fac. Surg. 1997;55:253-9.<br />
18. Zachariades N, Papavassiliou D, Papadenetrion I. The alteration<br />
in sensitivity of the infraorbital nerve following of the zygomatic<br />
maxillary complex. <strong>Journal</strong> Cranio-Max-Fac. Surg, 18:315-318.<br />
19. Kovacs and M. Ghahremani (2001). Minimization of zygomatic<br />
complex fracture treatment. Int <strong>Journal</strong>. Oral Max-Fac Surgery.<br />
1990;30(5):380-3.<br />
20. Covington DS, Wainwright. DJ, Teichgraeber JF et al. Changing<br />
patterns in the epidemiology and treatment of zygoma fractures:<br />
10-year review. <strong>Journal</strong> of Trauma. 1994;37:243.<br />
21. Knight, J.S. & North, J.F. The classification of Malar Fractures: An<br />
analysis of Displacement as a Guide to Treatment. Br. J. Plast Surg.<br />
1961;13:325-39.<br />
22. Folkestad Lena, MD, Granstrom Gosta, MD. A prospective study of<br />
orbital fracture squeals after change of surgical routines. J. Oral.<br />
Max-Fac, Surg. 2003;61:1038-44.<br />
23. Barclay TL. Diplopia in association with fractures involving the<br />
zygomatic bone. Br. J. Plast Surg. 1958;11:47.<br />
24. Zing M, Laedrach K, Chen J et al. Classification and treatment of<br />
zygomatic fractures: A review of 1,025 cases. J. Oral. Max-Fac.<br />
Surg. 1992;50:778.<br />
25. Chen CT. Chen YR. Endoscopically assisted repair of orbital floor<br />
fractures. Plast Reconstr. Surg. 2001;108:2011-8.<br />
26. Manson PN, Iliff N, Bradely R. Trapdoor fractures of the orbit in<br />
pediatric population. Plast Reconstr. Surg. 2002;109:490-5.<br />
27. Manolidis S, Weeks BH, Kirby M, M. Hollier. Classification and<br />
surgical management of orbital fractures: Experience with 111<br />
orbital reconstru- ctions. J. Craniofacial Surg. 2002;13: 726-37.<br />
28. Wray RC, Holtman B, Ribaudo JM, et al. A comparisons of<br />
conjunctival and subciliary incisions for orbital fractures.Br. J. Plast.<br />
Surg. 1977;30(2):142-5.<br />
29. Pospisil OA, Fernando TD (1984). Review of the lower<br />
blepharoplasty incision as a surgical approach to zygomaticoorbital<br />
fractures Br. N J. Oral. Max-Fac.<br />
30. Holtman B, Wray RC, Little G. A randomized comparison of four<br />
incisions for orbital fractures. Plast Reconstr. Surg. 1981;67:731-5.<br />
31. Jordan DR, Allen LH, White J, Harvey J, Pashby R, Esmaeli B.<br />
Intervention within days for some orbital floor fractures: the whiteeyed<br />
blow-out. Opthal. Plast Reconstr Surg. 1998;14:379-90.<br />
| 36 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011
TM<br />
TREATMENT PROGRAM<br />
Finally, instant * sensitivity relief<br />
patients can take home.<br />
A breakthrough: Pro-Argin TM Technology<br />
The results are revolutionary<br />
BEFORE 1<br />
AFTER 1<br />
Instant relief achieved with direct application<br />
of toothpaste massaged on sensitive tooth for<br />
one minute and continued relief with subsequent<br />
twice-daily brushing 3<br />
In Vitro SEM photograph of untreated<br />
dentin surface.<br />
The tubules that lead to<br />
sensitivity are open<br />
In Vitro SEM photograph of dentin<br />
surface after application.<br />
The tubules are plugged<br />
for instant, lasting relief<br />
With Pro-Argin Technology, you can finally provide instant*<br />
and lasting relief from dentin hypersensitivity using the<br />
Colgate® Sensitive Pro-Relief Treatment Program:<br />
• In-office desensitizing paste<br />
• At-home everyday toothpaste<br />
Air blast sensitivity score<br />
3<br />
2<br />
1<br />
0<br />
Baseline<br />
60%<br />
Immediate<br />
70%<br />
improvement<br />
3-day<br />
Sensitivity relief<br />
When applied directly<br />
to the sensitive tooth<br />
with a fingertip and<br />
gently massaged for<br />
1 minute, Colgate ®<br />
Sensitive Pro-Relief<br />
Toothpaste provides<br />
instant sensitivity<br />
relief compared to the<br />
positive and negative<br />
controls. The relief was<br />
maintained after 3 days<br />
of twice-daily brushing.<br />
Pro-Argin Technology works through a natural process of<br />
dentin tubule occlusion that attracts arginine and calcium<br />
carbonate to the dentin surface to form a protective seal<br />
that provides instant relief. 2<br />
Colgate ® Sensitive Pro-Relief Toothpaste<br />
Positive control:<br />
Toothpaste with 2% potassium ion<br />
Negative control:<br />
Toothpaste with<br />
1450 ppm<br />
fluoride only<br />
* Instant relief is achieved with direct application of toothpaste massaged on<br />
sensitive tooth for 1 minute.<br />
Scientific works cited: 1. Petrou I et al. J Clin Dent. 2009;20(Spec Iss):23-31. 2. Cummins D et al. J Clin Dent. 2009;20(Spec Iss):1-9.<br />
3. Nathoo S et al. J Clin Dent. 2009;20(Spec Iss):123-130.<br />
Visit www.colgateprofessional.com to learn more<br />
about how instant relief from dentin hypersensitivity<br />
can impact your practice.<br />
YOUR PARTNER IN ORAL HEALTH
TOTAL CAMOUFLAGE!<br />
• Refills available for each product<br />
• Smart consistency, for an easier job<br />
• Smart performance, multipurpose<br />
& micro-hybrid formula<br />
zmack ® system<br />
HIGH QUALITY<br />
FA IR P RI C E<br />
zmack ® comp zmack ® etch zmack ® bond<br />
Available in the following shades: A1;<br />
A2; A3; A3.5; A2-O; A3.5-O; B1; B2; B3; C3<br />
The first step for a quick, controllable<br />
& effective application<br />
Effective on humid or dry* dentine<br />
(*up to 10 sec.)<br />
Zmack kits contain: Zmack comp syringes* (6x4 g), Zmack bond bottle 5 ml, Zmack etch syringe 3 ml, Flocked applicators (50 pcs), Applicator needles (25 pcs)<br />
*For shades composition in the two zmack kits, contact your local dealer or visit www.zhermack.com<br />
YOUR SMART CHOICE TO CREATE SMILES<br />
Zhermack presents zmack ® system, the new universal<br />
light-cured composites line for conservative restoration<br />
that has been studied to solve everyday needs of dental<br />
practitioners and patients of any age. Born today, as the<br />
result of our laboratory experience and know how.<br />
Specially designed to mimetically blend with the<br />
surrounding tooth structure, zmack ® comp shades<br />
become imperceptible, for very natural, aesthetic and<br />
lasting results.<br />
Tel. +39 - 0425 597611 - Fax +39 - 0425 597645<br />
comm.expo@zhermack.com - www.zhermack.com
The Diagnosis and Management of<br />
Impacted Maxillary Canines<br />
Eyas Abuhijleh<br />
BDS, PhD<br />
• Specialist Orthodontist and<br />
Assistant Professor, Tawam<br />
Hospital, <strong>Dental</strong> Center<br />
Al Ain - UAE<br />
eabuhijleh@tawamhospital.ae<br />
Dalal Masri<br />
BDS<br />
• General <strong>Dental</strong> Practitioner<br />
Tawam Hospital, <strong>Dental</strong><br />
Center, Al Ain - UAE<br />
dmasri@tawamhospital.ae<br />
Nadia Farawana<br />
MDSc<br />
• German Board of<br />
Orthodontics, Tawam<br />
Hospital <strong>Dental</strong> Center,<br />
Al Ain - UAE<br />
nfarawana@tawamhospital.ae<br />
Mariam Nmari<br />
DDS<br />
• General <strong>Dental</strong> Practitioner<br />
Yas Medical Center<br />
Al Buraimi - Oman<br />
mariam.nmari@yahoo.com<br />
Abstract<br />
General dental practitioners and orthodontists will commonly encounter this problem<br />
(impacted maxillary canines) and need to be fully aware of managing this situation.<br />
Failure to diagnose and manage the ectopic upper canine efficiently can result in more<br />
complex remedial treatment becoming necessary, which would be costly in terms of<br />
clinical time for both the practitioner and patient. There is also the risk of damage to<br />
the adjacent teeth which may lead to their loss and eventually to costly litigation claims.<br />
The aims of this article are to:<br />
1. Present evidence based recommendations to assist <strong>Dental</strong> Clinicians (<strong>Dental</strong><br />
Surgeon, Orthodontist, Pediatric <strong>Dental</strong> Specialist, Oral Surgeon) in the timely<br />
detection and management of the ectopic maxillary canine.<br />
2. Detect and manage impacted maxillary canines early.<br />
3. Learn the complications associated with an impacted maxillary canine.<br />
Keywords: Impacted canines, Surgical exposure, Orthodontic treatment.<br />
Introduction<br />
Canines play a vital role in facial appearance, dental esthetics, arch development and<br />
functional occlusion. Canine impaction is a common occurrence, because it develops<br />
deep within the maxilla and has the longest path to travel compared with any other tooth<br />
in the oral cavity. It is only with interdisciplinary care of general dentists and specialists by<br />
early detection, timely interception, and well-managed surgical and orthodontic treatment<br />
that impacted maxillary canines can be erupted and guided to an appropriate location in<br />
the dental arch. 2<br />
Diagnosis<br />
Clinical signs<br />
• Over-retention of the primary canine. 2<br />
• Delayed eruption of the permanent canine. 2<br />
• Absence of a labial bulge in a 10- or 11- year-old patient. 2,3<br />
• Presence of a palatal bulge. 2<br />
• Distal crown tipping of the lateral incisor. 2,3<br />
Radiographic investigation<br />
The examination usually involves taking two radiographs and using the principle of<br />
horizontal or vertical parallax, the horizontal parallax technique being the more reliable<br />
in localizing impacted canines: 1<br />
1. Horizontal parallax involves taking either:<br />
• Two periapicals with different angulations and follow the (SLOB = same lingual<br />
opposite buccal) rule 1-4 or<br />
• An upper occlusal and a periapical.<br />
| 40 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011
Flow chart of the sequence of management of impacted maxillary canines<br />
Clinical Examination at Age 10<br />
Absence of Buccal Bulge and Presence of Palatal Bulge<br />
Radiographic Localization<br />
Line of Arch<br />
Buccally Ectopic<br />
Palatally Ectopic<br />
Monitor Eruption<br />
of Canine / Space<br />
Creation<br />
Monitor Eruption of Canine<br />
Extract Deciduous Canines / Space Creation<br />
Canine not Erupting in 1 year<br />
Radiographic Localization: Beneficial Change in Position<br />
YES<br />
NO<br />
Canine Buccally or Palatally Impacted<br />
Surgical Exposure & Orthodontic Alignment<br />
NO<br />
Surgical Removal or Auto-Transplantation<br />
NO<br />
No Treatment and continuous Monitoring<br />
2. Vertical parallax involves taking either:<br />
• An upper occlusal (70–75°) and an<br />
orthopantomogram (OPG) or<br />
• A periapical and an orthopantomogram (OPG). 1,4<br />
3. Advanced three-dimensional (3D) imaging<br />
techniques: Cone-beam computed tomography<br />
(CBCT) 1-4<br />
Radiographic features<br />
• Either non-vertical or no resorption of the deciduous<br />
canine root. 3<br />
• Canine crown overlapping adjacent incisor roots. 3<br />
• Resorption of adjacent incisor roots. 2,3<br />
• Magnification of the permanent maxillary canine<br />
crown on a panoramic radiograph. 3<br />
Management<br />
Interceptive treatment by extraction of the<br />
deciduous canine<br />
• The patient should be aged between 10-13 years. 1,4<br />
• Better results are achieved in the absence of<br />
crowding. 1,4<br />
• Position of the canine in the dental arch and in<br />
its relationship to the adjacent lateral decides the<br />
outcome of the interceptive treatment. 1,4<br />
• The need to maintain space (or even create additional<br />
space) requires consideration. 1,4<br />
• If radiographic examination reveals no improvement<br />
in the impacted canine’s position 12 months after<br />
extraction of the deciduous canine, alternative<br />
treatment should be considered. 1,4<br />
Surgical exposure and orthodontic alignment<br />
• The patient should be well motivated and willing to<br />
wear fixed orthodontic appliances. 1,4<br />
• The patient should have good medical and oral health,<br />
and maintain proper oral hygiene. 1,4<br />
• The patient is considered to be unsuitable for<br />
interceptive treatment. 1,4<br />
• The degree of malposition of the impacted canine<br />
should not be too great to preclude orthodontic<br />
alignment. 1,4<br />
• Exposure and alignment of the impacted canine is<br />
indicated in cases when severe root resorption of an<br />
incisor tooth has occurred necessitating its extraction. 4<br />
• The optimal time for surgical exposure and orthodontic<br />
alignment is during adolescence. 4<br />
• Open communication between the orthodontist and<br />
oral surgeon is essential for the choice of appropriate<br />
surgical techniques.<br />
• Careful selection of surgical and orthodontic<br />
techniques is essential for the successful alignment of<br />
impacted maxillary canines.<br />
• Measured orthodontic forces in a favorable direction<br />
leads to successful alignment.<br />
Surgical removal of the palatally impacted<br />
permanent canine<br />
• This treatment option should be considered if the<br />
patient declines active treatment and/or is happy with<br />
their dental appearance. 1,4<br />
• Surgical removal of the impacted canine should be<br />
considered if there is radiographic evidence of early<br />
root resorption of the adjacent incisor. 1,4<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011| 41 |
TOOLS TO KEEP SMILING<br />
No less than ...<br />
...4 launches !<br />
Mechanical scouting sequence<br />
10/.02<br />
www.d-race.ch<br />
15/.02<br />
Desobturation made easy<br />
Discover the other novelties on<br />
www.fkg.ch<br />
20/.02<br />
• The best results are achieved if there is good contact<br />
between the lateral incisor and first premolar. 1,4<br />
• It is indicated in patients willing to undergo<br />
orthodontic treatment to substitute the first premolar<br />
for the canine. 1,4<br />
• The possible risk of damaging the roots of adjacent<br />
teeth during the surgical removal of the impacted<br />
canine should be assessed and discussed with the<br />
patient. 1<br />
Auto-transplantation<br />
• This treatment option should be considered<br />
if the patient is unwilling to wear orthodontic<br />
appliances. 1,4<br />
• Transplantation is indicated where interceptive<br />
extraction of the deciduous canine has failed or<br />
is unsuitable, and exposure and alignment of the<br />
impacted canine is not possible. 1,4<br />
• There should be adequate space available for the<br />
canine and sufficient alveolar bone to accept the<br />
transplanted tooth. 1,4<br />
• The prognosis should be good if the canine to be<br />
transplanted shows no evidence of ankylosis. 1<br />
• The best results are achieved if the impacted canine<br />
can be removed atraumatically. 1,4<br />
• Depending on the stage of root formation (more<br />
than 3/4 of the root formed) the transplanted canine<br />
may require root canal therapy to be commenced<br />
within ten days following transplantation. 1<br />
No treatment and continuous monitoring<br />
• The patient does not want treatment or is happy with<br />
their dental appearance. 1,4<br />
• There should be no evidence of root resorption of<br />
adjacent teeth or other pathology. 1<br />
• There should be good contact between the lateral<br />
incisor and first premolar or the deciduous canine<br />
should have a good prognosis. 1,4<br />
• Severely displaced palatally impacted canines with no<br />
evidence of pathology may be left in-situ, particularly if<br />
the canine is remote from the dentition. 1<br />
• Impacted canines left in-situ necessitate<br />
radiographic monitoring to check for cystic changes<br />
or root resorption. 1,4<br />
• Regular review to ensure that the impacted canine<br />
does not pose any risk to the adjacent structures. 1,4<br />
References<br />
1. Management of the palatally ectopic maxillary canine, Husain<br />
J. et al., Publication of the Royal College of Surgeons, Faculty of<br />
<strong>Dental</strong> Surgery, online publication, updated March 2010.<br />
2. A review of the diagnosis and management of impacted<br />
maxillary canines, Bedoya M. and Park J., The <strong>Journal</strong> of the<br />
American <strong>Dental</strong> association (JADA). 2009;140:12:1485-93.<br />
3. Managing the maxillary canine: 1. Diagnosis, localization<br />
and interceptive treatment, McIntyre G., Orthodontic Update,<br />
January 2008;1:7-15.<br />
4. Clinical Practice Guidelines, The management of the palatally<br />
ectopic canine, Ministry of Health Malaysia, September 2004.<br />
• Crêt-du-Locle 4 • CH-2304 La Chaux-de-Fonds • Switzerland •<br />
• Tél.: +41 (0)32 924 22 44 • Fax: +41 (0)32 924 22 55 • info@fkg.ch • www.fkg.ch •<br />
| 42 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011
TM<br />
The Evolution of Floss<br />
Visit us at AEEDC<br />
Piro Trading International<br />
206-212 & 221-227<br />
Easier and More Effective<br />
Than String Floss!<br />
Waterpik ® Water Flossers continue to outperform traditional floss<br />
in study after study. And now your patients can get this superior<br />
Waterpik ® performance in a smaller, space-saving model that is<br />
perfect for smaller bathrooms and travel.<br />
Water flossing is simple and easy, with none of the mess or<br />
hassle of string. And your patients will love that it only<br />
takes a minute a day.<br />
So make an evolutionary step in your practice. Find out more<br />
about our new space-saving design. Contact: Call 1-XXX-XXX-XXXX<br />
Piro Trading International<br />
Middle for Professional East Representative Trial Offers. 209-667-7204<br />
Nano<br />
Ultra<br />
REMOVES<br />
99.9<br />
%<br />
OF PLAQUE<br />
2X<br />
AS EFFECTIVE<br />
AS STRING<br />
FLOSS<br />
14<br />
in just<br />
HEALTHIER GUMS<br />
DAYS<br />
G U A R A N T E E D<br />
Join the conversation at<br />
and<br />
waterpik.com<br />
Independent clinical study. Go to www.waterpik.com for details. © 2011.
THE THOUGHT<br />
OF THE DENTIST<br />
BRINGS A<br />
BROAD SMILE.<br />
AEEDC 2012<br />
Booth 303<br />
Middle East Area Manager<br />
Mahmoud Lutfi<br />
Tel: +962 6 5656404/5<br />
Fax: +962 6 5656402<br />
Mob: +962 7 95536867<br />
E-mail: mlutfi@go.com.jo
CMA<br />
®<br />
CORONAL • MEDIAN • APICAL<br />
Only one<br />
sequence<br />
for treatment<br />
and retreatment
Adhesion of Candida Albicans to Denture<br />
Base and Denture Liners with Different<br />
Surface Roughness<br />
An In-vitro Study<br />
Zahraa Nazar Al-Wahab<br />
BDS, MSc<br />
• Lecturer, Department of<br />
<strong>Dental</strong> Technologies, College<br />
of Health and Medical<br />
Technologies, Foundation of<br />
Technical Education<br />
Baghdad, Iraq<br />
zahraawahab@yahoo.com<br />
Abstract<br />
This study investigated adherence of Candida albicans to denture base acrylic resins<br />
and denture soft liners with varying surface roughness.<br />
Materials and Methods: Two denture base acrylic resins (heat cured resin and cold<br />
cured resin) and two commercial soft liners (one is heat polymerized acrylic resin<br />
based and one is room temperature polymerized silicon based) having dimensions of<br />
10X10X1.5mm for each specimen. Each material was divided into two groups: one is<br />
processed against glass slide surface and the other is processed against dental stone<br />
(10 samples for each group). Surface roughness measurements were made using a<br />
profilometer where a stylus traverses across the layer of the surface. Human saliva<br />
was collected from volunteers and the specimens were stored in human saliva which<br />
was contaminated with yeast suspension of approximately 106 Candida albicans per<br />
milliliter and incubated for 24hrs at 37C˚. After incubation, fixation of the attached<br />
cells was done by treating the specimens with 100% ethanol for 3s and left to dry in<br />
sterile plates. Specimens were stained using sterilized, fixated Methylene Blue stain for<br />
1min and subsequently evaluated under optical microscope (Olympus, Japan) at X400<br />
magnification. Visible measurement field was calculated in mm 2 and the obtained data<br />
were expressed in cell/mm 2 .<br />
Results: The materials processed against glass surface showed a very high significant<br />
difference in surface roughness values than those processed against dental stone<br />
surface (student t – test, P
(Table 1) Materials used in this study<br />
Type of Material Trade Name Manufacturer Batch Number<br />
Heat polymerized denture base acrylic resin Major base 2 (HC) Italy<br />
ISO 1567, type I class I ADA<br />
no.12<br />
Room temperature polymerized denture base acrylic resin Major repair 2 (CC) Italy<br />
ISO 1567, type II class I ADA<br />
no.12<br />
Heat-polymerized acrylic resin-based resilient liner<br />
Vertex Soft (V)<br />
Vertex-<strong>Dental</strong> BV, Zeist,<br />
The Netherlands<br />
100001<br />
Room temperature polymerized silicone-based resilient liner Mollosil (M)<br />
Detax, GmbH & Co. KG,<br />
Germany<br />
03008<br />
The presence of Candida albicans on the upper fitting<br />
surface of the denture is a major causative factor<br />
in denture-associated chronic atrophic candidosis<br />
(denture stomatitis), the most common form of oral<br />
candidosis. 2 Candida albicans is a dimorphic fungus that<br />
is commensal in the gastrointestinal and reproductive<br />
tracts of healthy individuals. Under certain predisposing<br />
conditions, Candida albicans can convert into a<br />
pathogen capable of causing a variety of oral infections<br />
including pseudomembranous candidiasis, erythematous<br />
candidiasis and hyperplastic candidiasis, as well as<br />
Candida-associated denture stomatitis, Candida<br />
associated angular cheilitis, rhomboid glossitis and<br />
chronic mucocutaneous candidiasis. 4<br />
Denture stomatitis is an erythematous pathogenic<br />
condition of the denture bearing mucosa and is mainly<br />
caused by microbial factors, especially Candida albicans. 5<br />
The etiology is multifactorial consisting of either ill-fitting<br />
prostheses leading to mechanical irritation or poor<br />
hygiene leading to chronic infection, regardless of the<br />
initiating process Candida ablicans is the main cause of<br />
fungal origin in denture stomatitis. 6<br />
The first step implicated in denture stomatitis is adherence<br />
of Candida to acrylic or to salivary pellicles adsorbed on<br />
the surface of dental prosthesis. This is considered the<br />
most important event in the ability of Candida albicans to<br />
colonize dentures in the mouth. 4 The aim of this study is<br />
to assess the ability of Candida albicans adherence to two<br />
types of acrylic resin and two types of soft lining materials<br />
with different surface roughness.<br />
Materials and Methods<br />
Two commercially available denture base acrylic resins<br />
were used, one is heat cured (HC) and the other is<br />
cold cured (CC). Two liners were used, one is heat<br />
polymerized acrylic resin based (V) and the other is room<br />
temperature polymerized silicone based (M). All of these<br />
materials were listed in Table 1.<br />
Preparation of the specimens<br />
Pink modeling wax forms (10X10X1.5) mm were<br />
punched from a sheet of wax. Stone was mixed<br />
according to the manufacturer’s instruction in the lower<br />
half of the flask. Two types of mold were prepared in<br />
such a manner that in the first type, one part of the mold<br />
was dental stone and the other is glass surface, while<br />
in the second type, both parts of the mold were dental<br />
stone. To produce the specimens against the glass,<br />
a glass microscope slide was pressed onto the stone<br />
mixture in the lower part of the flask. After the stone has<br />
set, wax specimens were placed on the top of the glass<br />
slide surface. The upper part of the flask was placed in<br />
position and the dental stone was poured over the wax<br />
specimens. The flasks were separated and boiled out,<br />
and the cover glass was degreased with liquid detergent.<br />
The surface of the investing dental stone was lubricated<br />
with separating media before packing of the materials.<br />
All the tested materials were processed according to the<br />
manufacturer’s instructions.<br />
Sample grouping<br />
HC1: Heat cured denture base acrylic resin processed<br />
against glass<br />
CC1: Cold cured denture base acrylic resin processed<br />
against glass<br />
V1: Heat polymerized acrylic resin-based resilient liner<br />
processed against glass<br />
M1: Room temperature polymerized silicone-based<br />
resilient liner processed against glass<br />
HC2: Heat cured denture base acrylic resin processed<br />
against dental stone<br />
CC2: Cold cured denture base acrylic resin processed<br />
against dental stone<br />
V2: Heat polymerized acrylic resin-based resilient liner<br />
processed against dental stone<br />
M2: Room temperature polymerized silicone-based<br />
resilient liner processed against dental stone<br />
Estimation of surface roughness of the specimens<br />
The surface roughness of the specimens was measured<br />
with profilometer (Talysurf 4, Taylor Hasbon, UK), where<br />
a stylus traverses across the layer of the surface. Three<br />
readings were taken for every specimens and the<br />
average was calculated. The average surface roughness<br />
values for all tested specimens are presented in Table 2.<br />
Methods of saliva collection<br />
Whole unstimulated saliva samples were collected and<br />
pooled from 5 healthy male volunteers to eliminate<br />
sample variation, 4 aged 18 – 22, (mean 20 years). The<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011| 47 |
(Table 2) Mean surface roughness values (Ra) and standard<br />
deviation (SD) of all tested groups (in µm)<br />
Mean and SD Group Mean ± SD Group<br />
2.5±0.253 HC2 1.31 ± 0.166 HC1<br />
5.59± 0.272 CC2 1.57±0.125 CC1<br />
4.11±0.272 V2 1.4±0.221 V1<br />
7.48±0.345 M2 1.5±0.290 M1<br />
(Table 3) Mean and Standard deviation of Candida albicans<br />
adhesion to all groups in cells/mm 2<br />
Mean and SD Group Mean ± SD Group<br />
3426.7 ±118.3 HC2<br />
5371.8±223.45 CC2<br />
5189.9±127.87 V2<br />
7916.5±306.68 M2<br />
1273.7±<br />
220.82<br />
1580.8<br />
±117.46<br />
1588.77 ±<br />
152.12<br />
1590.36 ±<br />
452.17<br />
HC1<br />
CC1<br />
(Table 4) Student–test comparing the mean surface roughness<br />
values for each material according to the type of surface processing<br />
Groups t – value P – value Group<br />
saliva was collected between 9.00 and 10.00 am and<br />
the volunteers had not eaten that morning. They were<br />
not taking any drugs or medications known to affect<br />
saliva production, composition, or flow within the last<br />
three months. They were not taking any antibiotics or<br />
antifungal agents. 8,7,4 Saliva was centrifuged at 14000g<br />
for 15min and then it was used immediately. 8<br />
Obtaining Candida albicans<br />
Candida albicans strain ATCC 2091 was obtained as a<br />
stock culture (from Pathological Analysis Department of the<br />
College of Health and Medical Technologies, Baghdad,<br />
Iraq), and incubated on Sabouraud dextrose agar slope<br />
at 37°C for 48 h . Standard amounts of this culture were<br />
inoculated into 2ml of liquid Sabouraud dextrose agar<br />
and incubated at 37°C for 24 h . The culture was then<br />
centrifuged (Function Line, Labofuge 400 R, Hereaus<br />
V1<br />
M1<br />
HC1 & HC2 2.9748 P
(Table 6) One-way ANOVA test comparing Candida albicans<br />
adhesion among materials processed against dental stone surface<br />
Significance P-value F-value Group<br />
VHS P
adhesion on hydrophobic material was low. This result<br />
also agrees with 16 and 19 , these studies stated that silicon<br />
soft liner are more susceptible to Candida albicans<br />
adhesion than acrylic resin since surface porosity, texture<br />
and biologic and physical / chemical affinity between the<br />
materials and microbial cells may be an important factor.<br />
The results of the present study showed that molosil<br />
soft liner processed against dental stone showed<br />
significantly higher adhesion than vertex soft liner and<br />
this agrees with 20 , a study stated that heat polymerized<br />
soft liner showed lower adhesion than room temperature<br />
polymerized soft liner. This finding is in agreement with 3 ,<br />
a study which explained this result due to the presence<br />
of porosities inside the matrix of the room temperature<br />
polymerized material which facilitates the penetration<br />
of blastospores. This finding agrees with 5,3 and 19 .<br />
This finding also agrees with 9 , a study found that the<br />
adherence of Candida albicans on room temperature<br />
polymerized surfaces is related to the polymerization<br />
method of the material tested.<br />
In this study, there was no statistically significant<br />
difference in Candida albicans adhesion between<br />
cold cured denture base acrylic resin (CC2) and heat<br />
polymerized acrylic resin based liner (V2) polymerized<br />
against dental stone surface. This is because the<br />
chemical composition of (V2) is similar to that of the<br />
polymethyl methacrylate of cold cured denture base<br />
acrylic resin polymer. 21<br />
Conclusion<br />
Rough surfaces of the denture base and soft liner<br />
promote the adhesion of Candida albicans in vitro and<br />
the surfaces that are as smooth as possible are more<br />
desirable in terms of cleanability and prevention of<br />
fungal disease. The selection of appropriate material<br />
for a given function and their fabrication may affect the<br />
performance of the material.<br />
References<br />
1. Radford DR, Watson TF, Walter JD Stephen J. Challacombe SJ. The<br />
effects of surface machining on heat cured acrylic resin and two soft<br />
denture base materials: a scanning electron microscope and confocal<br />
microscope evaluation. J Prosthet Dent. 1997;78(2):200-8.<br />
2. Waters MGJ, Williams DW, Jagger RG, Lewis MAO. Adherence of<br />
Candida albicans to experimental denture soft lining materials. J<br />
Prosthet Dent. 1997;77(3):306-12.<br />
3. Bulad K, Taylor R, Verran J, Mc Cord F. Colonization and penetration<br />
and denture doft lining materials by cardida. albicans Dent Mater.<br />
2004;20:167-75.<br />
4. Elguezabell N, Maza JL, Dorronsoro S, Pontou J. Whole saliva has a<br />
dual role on the adherence and C. albicans to polyethyl methacrylate.<br />
The open Dentistry J. 2008;2:1-4.<br />
5. Nikawa H, Jintc Hamad A, Smak RA, Kumage H, Murat H. The<br />
interactions between thermal cycled resilient denture lining materials<br />
salivary and serum pellicles and Candida albicans in vitro: part II<br />
Effects on fungal colonization. J Oral Rehab. 2000;27:124-30.<br />
6. Kulak – Ozkan Y, Kazazoglu E, Arikan A. Oral hygiene habits,<br />
denture cleanliness, presence and yeasts and stomatitis in elderly<br />
people. J Oral Rehabel. 2002;29(3):300-4.<br />
7. Moura JS, da Silva WJ, Pereira T, Bel Cury AAD, Rodrigues Garcia<br />
RCM. Influence of acrylic resin polymerization methods and<br />
saliva on the adherence of four Candida species. J Prosthet Dent.<br />
2006;96:205-11.<br />
8. Radford DR, Sweet SP, Challacombe SJ, WalterJD. Adherence of<br />
Candida albicans to denture-base materials with different surface<br />
finishes. <strong>Journal</strong> of Dentistry. 1998;26:577-83.<br />
9. Vurual C, Ozdemir G, Kurtulmus H, Kumbuloglu O, Ozcan M.<br />
Comparative effects of two different artificial body fluids on<br />
Candida albicans adhesion to soft lining materials. Dent Mater J.<br />
2010;29(2):206-12.<br />
10. Douglass LJ. Candida biofilm and their role in infection. Trends<br />
Microbiol. 2003;11:30-6.<br />
11. Grubb BR, Chadburn JL, Boucher CR. Cr. In vitro microdialysis<br />
for determination and nasal liquid composition, Am J Physiol.<br />
2002;282:1423-31.<br />
12. Nevzatoğlu EU, Özcan M, Kulak-Ozkan Y, Kadir T. Adherence<br />
of Candida albicans to denture base acrylics and silicone-based<br />
resilient liner materials with different surface finishes. Clin Oral<br />
Invest. 2007;11:231-6.<br />
13. Verran J Maryan CJ. Retention of Candida abicans on acrylic resins<br />
and silicon and different surface topography. J Prosthet Dent.<br />
1997;77:535-9.<br />
14. Taylor R, Maryan CH, Verran J. Retention of oral microorganisms<br />
on cobalt – chromium and dental acrylic resin with different surface<br />
finishes. J Prosthet Dent. 1998;80(5):592-7.<br />
15. Henriques M, Azeredo J, Oliveira R. Adhesion of Candida albicans<br />
and Candida dubliniensis to acrylic and hydroxyapatite. Colloids<br />
and Surfaces B:Biointerffaces. 2004;33(3-4):235-41.<br />
16. Pereira T, Cury AADB, Cenci Ms, Rodrigues – Garcia RCM. In vitro<br />
Candida colonization on acrylic resins and denture linors: Influence<br />
and surface frequencu, roughness, saliva and adhering bacteria. Int<br />
J prosthodnt. 2007;20:308-10.<br />
17. Hammoudi IM. Evaluation of the effect of polishing techniques on<br />
surface roughness and adhesion of Candida albicans to the acrylic<br />
complete denture. A thesis submitted to the College of Dentistry<br />
in partial fulfillment of the requirements of Master of Science in<br />
Prosthodontics, 2006.<br />
18. Periera – Cenci T, Del bdcury A, Crielard W Tencate JM.<br />
Development and Candida – associated denture stomtitis: New in<br />
sights. J App Oral sci. 2008;16(2):86-94.<br />
19. Bal BT, Yavuzyilmaz H, Yucel M. A pilot study to evaluate the<br />
adhesion oral microorganisms to temporary soft lining materials. J<br />
Oral Sci. 2008;50(1):1-8.<br />
20. Gedik H, Ozkan YK. The effect of surface roughness of siliconebased<br />
resilient liner materials on the adherence of Candida albicans<br />
and inhibition of Candida albicans with different disinfectants.Oral<br />
Health Prev Dent. 2009;7(4):347-53.<br />
21. Mese A, Guzel KG. Effect of storage duration on the hardness and<br />
tensile bond strength of silicone- and acrylic resin-based resilient<br />
denture liners to a processed denture base acrylic resin. J Prosthet<br />
Dent. 2008;99:153-9.<br />
8 th Gulf <strong>Dental</strong> Association Conference<br />
& 2 nd Qatar Internationl <strong>Dental</strong> Association Conference<br />
| 50 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011<br />
12 - 13 April 2012<br />
Sharq Village<br />
&<br />
Spa Hotel<br />
Doha - Qatar
Assurance<br />
Invest in reliability. Focus on the patient.<br />
Express your style. From the people<br />
who build the most dependable dental<br />
equipment in the world, A-dec 200<br />
provides you with a complete system to<br />
secure a successful future.<br />
visit A-dec<br />
at AEEDC<br />
stand 230<br />
Discover how you can gain assurance with<br />
A-dec 200. Contact your authorised<br />
A-dec dealer today.<br />
Discover A-dec 200. Contact your local dealer.<br />
A-dec Inc.<br />
2601 Crestview Drive, Newberg, Oregon 97132 USA<br />
www.a-dec.com
December Expert Panel<br />
Hassan Maghaireh<br />
BDS, MFDS, MSc<br />
• BDS, Cairo University<br />
• MFDS, RCS Edinburgh<br />
• MSc Implants University of<br />
Manchester<br />
• Honorary Clinical Teacher,<br />
University of Manchester<br />
• Editorial Board; European<br />
<strong>Journal</strong> of Oral Implantology<br />
• Implant Referral Practice,<br />
Leeds - UK<br />
• maghaireh@smile-mag.com<br />
Wesam Aleid<br />
• BDS, MBBS, MRCSEd<br />
(Surgery-in-General),<br />
FFDRCSI (OSOM), FRCSEd<br />
(OMFS)<br />
• Oral, Maxillofacial, and<br />
Head & Neck Surgeon, UK<br />
• eidwisam@yahoo.com<br />
Alexandre Khairallah<br />
BDS, PGD<br />
• PGD, Oral and Maxillo- facial<br />
Imaging, Lebanese Univ.<br />
• Fellow of the European<br />
Academy of Maxillo-Facial<br />
Radiologist<br />
• Chef de Service, Oral and<br />
Maxillo-facial Imaging Dept,<br />
<strong>Dental</strong> School, Lebanese Univ.<br />
• Founder and owner of<br />
CLIR, Centre de Lecture et<br />
d’Interpretation Radiologique<br />
• alexandrekhairallah@<br />
hotmail.com<br />
Ali Abu Nema<br />
BDS, NDB, MSc<br />
• BDS, Jordan University of<br />
Science and Technology<br />
• NDB, American <strong>Dental</strong><br />
Association<br />
• MSc, Endodontics University<br />
of Manchester, UK<br />
• Private Endoodontic Referral<br />
Practice, Amman-Jordan<br />
• abunema_ali@hotmail.com<br />
What is the up to date<br />
evidence comparing flapless<br />
implant placement to<br />
conventional placement with<br />
flap elevation ?<br />
Answer: Dr. Hassan Maghaireh<br />
Flapless implant surgery is<br />
considered by some clinical reports<br />
to offer advantages over the<br />
traditional flap access approach.<br />
Clinicians supporting this view<br />
claim that flapless implants offer<br />
minimized bleeding, decreased<br />
surgical times and minimal<br />
patient discomfort, other less<br />
supported reports also claim that<br />
with flapless placement, you can<br />
get less marginal bone loss and<br />
better aesthetics. On the other<br />
hand, the view supporting open<br />
flap implant placement argue that<br />
with conventional flaps, clinicians<br />
will have better visualization for<br />
the adjacent vital structures, bone<br />
fenestratins and dehiscences,<br />
adjacent teeth and soft tissue<br />
thickness, making it easier for<br />
the clinicians to place the dental<br />
implant(s) in the optimum way, in<br />
addition to allowing the clinician to<br />
carry out guided bone regeneration<br />
procesure simultaneously with<br />
implant placement which in return<br />
allows for better aesthetic results.<br />
While the dental literature is full<br />
of descriptive studies and clinical<br />
case reports promoting flapless<br />
implant placement as a modern<br />
technique, there is very little properly<br />
conducted random controlled<br />
clinical studies comparing flapless<br />
placement with conventional flaps<br />
in implant dentistry. The systematic<br />
review conducted by Esposito et al.<br />
(2007) has only managed to identify<br />
five well conducted trials on this<br />
topic and has concluded that while<br />
flapless implant placement is feasible<br />
and has been shown to reduce<br />
patient postoperative discomfort<br />
in adequately selected patients, no<br />
effect was found on marginal bone<br />
level or final aesthetic results.<br />
| 54 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011
A recent well conducted random<br />
controlled trial by Cannizzaro et<br />
al. (2010), compared flapless<br />
versus open flap implant surgery<br />
in partially edentulous patients,<br />
in a split mouth design involving<br />
40 patients and 143 implants,<br />
reported no statistically significant<br />
difference between the two groups<br />
when looking into implants and<br />
prosthetic success and post operative<br />
complications. However, the same<br />
study reported that placement of<br />
flapless implants required statistically<br />
significant less time than placement<br />
after flap elevation with their patients<br />
reporting less post operative swelling<br />
and requiring less analgesics.<br />
However, what’s interesting is that<br />
this well conducted study which was<br />
the first to look in to the effect of<br />
flapless implants on marginal bone<br />
levels in comparison to open flap<br />
surgery, has reported no statistically<br />
significant differences between the<br />
two groups at baseline and 1 year<br />
after loading.<br />
To conclude, Flapless implant<br />
placement is becoming a popular<br />
topic in implant dentistry, and<br />
with the evolution in radiological<br />
imaging and introduction of new<br />
techniques like the Nobel Guide<br />
protocol, it became a more precise<br />
and predictable procedure in<br />
well selected patients. We should,<br />
however, be aware that flapless<br />
surgery does not automatically<br />
contribute to a better direct<br />
postoperative quality of life or better<br />
aesthetics.<br />
Recommended reading list:<br />
• Interventions for replacing missing<br />
teeth: management of soft tissues for<br />
dental implants, Esposito M, Grusovin<br />
MG, Maghaireh H, Coulthard P,<br />
Worthington HV. Chichester, UK:<br />
Cochrane Database of Systematic<br />
Reviews 2007 John Wiley & Sons, Ltd.<br />
• Flapless versus open flap implant<br />
surgery in partially edentulous<br />
patients subjected to immediate<br />
loading: one-year results from a splitmouth<br />
randomised controlled trial.<br />
Cannizzaro G, Esposito M, EJOI 2011.<br />
• A comparison of two implant<br />
techniques on patient-based outcome<br />
measures: a report of flapless<br />
vs. conventional flapped implant<br />
placement, Jerome A. Lindeboom,<br />
Arjen J. van Wijk, Clin. Oral Impl. Res.<br />
21, 2010.<br />
In condylar Fractures,<br />
is open reduction and<br />
internal fixation better than<br />
functional intermaxillary<br />
fixation?<br />
Answer: Dr. Wesam Aleid<br />
Background<br />
Treatment of condylar fractures<br />
has always been and continues to<br />
be an area of hot debate, as to<br />
whether conservative treatment with<br />
Functional intermaxillary fixation<br />
(IMF) is as good as the open<br />
reduction and internal fixation (ORIF).<br />
Several classification systems<br />
emerged e.g. Spiessel and Schroll,<br />
Neff, and SORG. The most widely<br />
used classification in the United<br />
Kingdom is the one described by<br />
Richard Loukota in 2005 1 which was<br />
revised in 2009. 2<br />
Evidence<br />
Several clinical trials have been<br />
conducted over the past two decades<br />
to objectively measure the difference<br />
in outcome between IMF and ORIF.<br />
In 1998 JOOS compared the<br />
outcome in a group of 122 patients<br />
with 138 fractures, he concluded<br />
that simple conservative treatment<br />
had comparable results to ORIF<br />
and therefore should be first line<br />
management.<br />
In 2003 Luc treated 60 patients<br />
with 71 fractures conservatively<br />
and despite that 35% of his patients<br />
developed symptoms of TMJ<br />
dysfunction, he still concluded that<br />
it is reasonable to manage condylar<br />
fractures conservatively unless the<br />
overlap between fragments is more<br />
than 8mm, which is an indication for<br />
ORIF in his view.<br />
In 2006 Eckelt and Loukota 3<br />
published a prospective randomised<br />
multi-centre study which they refined<br />
in 2008. 4 The study included 66<br />
patients with 79 fractures, which<br />
has shown a significantly improved<br />
outcome for patients treated with<br />
ORIF when the Fracture angulation<br />
was more than 10 degrees, when<br />
the ramus shortening (overlap)<br />
was more than 2mm, or when the<br />
fracture was bilateral.<br />
Confusion<br />
What about growing children?<br />
How I do it:<br />
At any age if no malocclusion is<br />
present then treatment is only with<br />
soft diet. Even minimal malocclusion<br />
should be allowed a week before<br />
any intervention as it may be a<br />
consequence of joint effusion,<br />
tissue oedema or pain rather than<br />
displacement of the fracture (Fig. 1).<br />
(Fig. 1) Right side of a PA mandible showing<br />
minimally displaced right condylar fracture.<br />
In Adults, the absolute indications<br />
for ORIF are:<br />
• Inability to obtain adequate<br />
occlusion by closed treatment<br />
• Lateral extracapsular displacement<br />
of the condyle<br />
• Displacement of the condyle into<br />
the external auditory meatus or the<br />
middle cranial fossa<br />
• Presence of foreign body or gross<br />
contamination of the joint<br />
Relative indications for ORIF:<br />
• Bilateral condylar fractures in<br />
edentulous Jaw<br />
• Bilateral condylar fracture in<br />
presence of midface comminution<br />
• IMF contraindicated for medical<br />
reasons (like COPD, Epilepsy, etc...)<br />
• Ramus shortening (fragment<br />
overlap) of more than 2mm (Figs.<br />
2-4)<br />
• Fragments angulation of more than<br />
10 degrees (Figs. 2-4)<br />
Children less than 12 years old:<br />
Always IMF as first line, starting with<br />
rigid fixation for seven to ten days<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011| 55 |
(Fig. 2) Coronal CT of left condylar fracture<br />
with comminution angulation, and overlap<br />
the mandibular condylar process–a<br />
prospective randomized multi-centre<br />
study. <strong>Journal</strong> of Cranio-Maxillofacial<br />
Surgery. 2006;34:306-14.<br />
4. Matthias Schneider et al. Open<br />
Reduction and Internal Fixation<br />
Versus Closed Treatment and<br />
Mandibulomaxillary Fixation of<br />
Fractures of the Mandibular Condylar<br />
Process: A Randomized, Prospective,<br />
Multicentre Study With Special<br />
Evaluation of Fracture Level. J Oral<br />
Maxillofac Surg. 2008;66:2537-44.<br />
(Fig. 1) Drawing of the line<br />
What are the causes<br />
of differences in height<br />
between measurements on<br />
para axial cuts issued from<br />
a Dentascan and the clinical<br />
reality?<br />
(Fig. 2)<br />
Cut for choosing<br />
implant<br />
(Fig. 3) PA mandible of left condylar fracture<br />
(same patient in figure1)<br />
(Fig. 4) PA mandible of left condylar fracture<br />
following ORIF (same patient in figure1)<br />
followed by functional (elastics) IMF<br />
for three to four weeks due to risk of<br />
ankylosis of the joint.<br />
Children 12 to 17 years old:<br />
Treat with IMF for two to three<br />
weeks. If Malocclusion persists<br />
consider ORIF.<br />
References<br />
1. Loukota RA et al. Subclassification<br />
of fractures of the condylar process<br />
of the mandible. British <strong>Journal</strong><br />
of Oral and Maxillofacial Surgery.<br />
2005;43:72-3.<br />
2. Loukota R.A. et al. Nomenclature/<br />
classification of fractures of the<br />
mandibular condylar head. British<br />
<strong>Journal</strong> of Oral and Maxillofacial<br />
Surgery. 2010; 48:477-8.<br />
3. ECKELT U et al. Open versus<br />
closed treatment of fractures of<br />
Answer: Dr. Alexandre Khairallah<br />
The dentascan exam consists of a<br />
series of axial acquisitions parallel<br />
to the palate in the upper jaw and<br />
the inferior border of the mandible<br />
in the lower jaw; these are fixed<br />
teeth free references. After choosing<br />
a specific axial cut (fig. 1) passing<br />
by the apices of teeth for instance<br />
or parallel to the inferior alveolar<br />
nerve,or the floor of the sinus,the<br />
operator will draw a line with his<br />
mouse on this particular cut.<br />
The computer will automatically<br />
generate a series of para axial<br />
cuts perpendicular to this specific<br />
line.Usually all measurements are<br />
done on para axial cuts in order to<br />
choose the exact implant’s length<br />
and width (fig. 2). As mentioned<br />
above, para axial cuts are<br />
perpendicular to the line and not<br />
to the maxilla or mandible (fig. 1).<br />
Special attention must be drawn in<br />
designing this specific line, it must<br />
be parallel to the outer aspect of<br />
the mandible or maxilla in order to<br />
get theexact length and width of the<br />
remaining bone (fig. 3); otherwise<br />
measurements are calculated on<br />
an oblique cut (fig. 4) and usually<br />
this will lead to overestimated<br />
measurements since the hypotenuse<br />
of a rectangular triangle is bigger<br />
than the adjacent segments<br />
according to the Pythagoras theorem<br />
in trigonometry (c2=a2+b2).<br />
(Fig. 3) Parallel line will give exact measurements<br />
(Fig. 4) Non parallel line will give wrong<br />
measurements<br />
For further informations you may<br />
consult these references:<br />
• Liang-Kuang C, Cheng-Tau Su,<br />
Yuh-Feng T. Spiral <strong>Dental</strong> CT: Use in<br />
Evaluating <strong>Dental</strong>Implantation. Chin J<br />
Radiol. 2006;26:209-14.<br />
• Danforth R, Dus I, Mah J. 3-D Volume<br />
Imaging for Dentistry: A New Dimension.<br />
CDA <strong>Journal</strong>. 2003;31:817-23.<br />
• Covino SW, Mitnick RJ, Shprintzen<br />
RJ, Cisneros GJ. The accuracy of<br />
measurements of three-dimensional<br />
computed tomography reconstructions. J<br />
Oral MaxillofacSurg. 1996;54:982-90.<br />
C<br />
M<br />
Y<br />
CM<br />
MY<br />
CY<br />
CMY<br />
K<br />
| 56 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011
What are the advatnages<br />
and disadvantages of using<br />
Chlorhexidine as a root<br />
canal irrigant?<br />
Answer: Dr. Ali Abu Nema<br />
Bacteria and their<br />
byproducts are<br />
considered to be one of<br />
the main causes of root<br />
canal treatment failure.<br />
Hence, a major objective<br />
in root canal treatment is<br />
to disinfect the entire root<br />
canal system.<br />
Chlorhexidine digluconate<br />
(CHX) is widely used in<br />
disinfection because of<br />
its excellent antimicrobial<br />
activity. Its cationic structure<br />
provides a unique property<br />
named substantivity;<br />
however, it lacks tissue<br />
dissolving ability.<br />
CHX<br />
Mechanism of action<br />
CHX is a positively charged<br />
hydrophobic-lipophilic molecule<br />
that interacts with phospholipids<br />
and lipopolysaccharides on the<br />
cell membrane of bacteria and<br />
enters the cell through some type<br />
of active or passive transport<br />
mechanism. Its efficacy is due to the<br />
interaction of the positive charge<br />
of the molecule with the negatively<br />
charged phosphate groups on<br />
C<br />
microbial cell walls, which alters<br />
M<br />
the cells osmotic equilibrium. This<br />
Y<br />
CM<br />
(Fig. 1)<br />
d) Cell Lysis<br />
increases the permeability of the cell<br />
wall, allowing the CHX molecule to<br />
penetrate into the bacteria (fig. 1).<br />
Antibacterial activity<br />
2% CHX was found to be the<br />
only solution able to eliminate<br />
Actinomyces israelii. Oncag et al.<br />
evaluated the antibacterial properties<br />
against Enterococcus faecalis of<br />
5.25% NaOCl and 2% CHX. The 2%<br />
CHX was significantly more effective<br />
against E faecalis. Also it has shown<br />
Mechanisms of CHX<br />
Active (or) Positive<br />
Transport Mechanism<br />
a) +ve Charged CHX Molecules<br />
b) -ve charged phoshate<br />
groups on microbial cell wall<br />
c) CHX interacts with phosphate group of<br />
microbial cell which after the cells osmotic equilibrium<br />
to be that 2% CHX is very effective<br />
against Staphylococcus aureus and<br />
Candida albicans.<br />
Substantivity<br />
The antimicrobial substantivity of a<br />
2% CHX solution as an endodontic<br />
irrigant was reported to be 72<br />
hours. It has been found that 5 min<br />
application of 2% CHX solution<br />
induced substantivity for up to 4<br />
weeks. Another study found that the<br />
substantivity of 2% CHX solution for<br />
10 min application was for 12 weeks.<br />
Leakage of<br />
adenosine tri<br />
phosphate<br />
Nucleic Acid<br />
(Fig. 2)<br />
Interaction between CHX<br />
and NaOCl<br />
A suggested clinical<br />
protocol consists of<br />
irrigation with NaOCl<br />
to dissolve the organic<br />
components, irrigation<br />
with EDTA to eliminate the<br />
smear layer and irrigation<br />
with CHX to increase the<br />
antimicrobial activity and<br />
to induce substantivity. Such<br />
a combination of irrigants<br />
may enhance the overall<br />
antimicrobial effectiveness,<br />
however, some studies have<br />
reported the occurrence<br />
of color change and<br />
precipitation when NaOCl<br />
and CHX are combined<br />
and shown to be toxic. Furthermore,<br />
the color change may have some<br />
clinical relevance because of staining<br />
and that the precipitate might interfere<br />
with the seal of the root filling (fig. 2).<br />
Please find below two recommended<br />
articles discussing the above topic:<br />
• Mohammadi Z, Abbott PV. The<br />
properties and applications of<br />
chlorhexidine in endodontics. Int Endod<br />
J. 2009;42(4):288-302.<br />
• Kanisavaran ZM. Chlorhexidine<br />
gluconate in endodontics: an update<br />
review. Int Dent J. 2008;58(5):247-57.<br />
MY<br />
CY<br />
IDA<br />
CMY<br />
K<br />
Annual Conference 2012<br />
30 - 31 March 2012<br />
Saad Palace, Erbil - Iraq<br />
2 nd Iraqi <strong>Dental</strong> Reunion<br />
“Breaking New Opportunities”<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011| 57 |
DO YOU SUFFER FROM<br />
BLEEDING GUMS?<br />
BLEEDING GUMS CAN BE THE FIRST SIGN OF GUM DISEASE,<br />
WHICH IS THE NO. 1 CAUSE OF TOOTH LOSS.<br />
HELPS STOP BLEEDING GUMS<br />
A DAILY TOOTHPASTE WITH MINERAL SALTS AND 6 NATURAL HERB EXTRACTS
AEEDC 2012<br />
Booth 312<br />
SISTEMA DIGITALE (DR) PER<br />
L’ACQUISIZIONE E L’ELABORAZIONE<br />
DI IMMAGINI INTRAORALI<br />
INTRAORAL IMAGES ACQUISITION AND<br />
PROCESSING DIGITAL SYSTEM (DR)<br />
SISTEMA INTRAORALE ALTA FREQUENZA<br />
HIGH FREQUENCY INTRAORAL SYSTEM<br />
DIAGNOSTICA DIGITALE DENTALE<br />
DENTAL DIGITAL DIAGNOSTIC<br />
ViVi s.r.L. - Via Dei Lavoratori, 3/K - Buccinasco Italy - Tel. (+39) 02 45703068 - Fax (+39) 02 45703463 - www.vivi-italy.it - vivi@vivi-italy.it
Summarized & Presented by:<br />
Hani Abudiak<br />
BDS, MFDS RCSFRCD, PhD Paediatric Dentistry, Leeds University<br />
• Canadian Fellowship in Paediatric Dentistry<br />
• Senior <strong>Dental</strong> Officer in Paediatric, Bradford Teaching Hospital, England<br />
• Private Paediatric Referral Practice, Leeds, England, UK<br />
hani@clarendondentalspa.co.uk<br />
Endodontic or <strong>Dental</strong> Implant Therapy<br />
The Factors Affecting Treatment Planning<br />
JADA, Vol. 13, July 2006<br />
Mahmoud Torabinejad, DMD, MSD, PhD; Charles J. Goodacre, DDS, MSD<br />
Background<br />
For decades, all disciplines of dentistry have strived to prevent and treat caries and periodontal disease, as well<br />
as to restore function and esthetics to patients affected by oral diseases or traumatic injuries. Despite these efforts,<br />
many non-restorable teeth and teeth with severe periodontal involvement have been extracted, and traditionally<br />
they have been replaced with fixed or removable prostheses. Advances in implant dentistry have provided<br />
thousands of completely and partially edentulous patients with a more functional and attractive alternative to fixed<br />
and removable prostheses.<br />
Nowadays, clinicians are confronted with difficult choices regarding whether a tooth with pulpal and/or periapical<br />
disease should be saved through endodontic treatment or be extracted and replaced with an implant.<br />
Methods<br />
The authors examined publications (research, literature reviews and systematic reviews) related to the factors<br />
affecting decision making for patients who have oral diseases or traumatic injuries.<br />
Results<br />
The factors to be considered included patient-related issues (systemic and oral health, as well as comfort and<br />
treatment perceptions), tooth- and periodontium-related factors (pulpal and periodontal conditions, color<br />
characteristics of the teeth, quantity and quality of bone, and soft-tissue anatomy) and treatment-related factors (the<br />
potential for procedural complications, required adjunctive procedures and treatment outcomes).<br />
Conclusions<br />
The decision by the clinician and patient to retain or remove teeth should be based on a thorough assessment of<br />
information related to risk factors affecting the long-term prognosis for endodontic and dental implant treatment.<br />
The clinician should consider several factors when determining whether to save a tooth through endodontic therapy<br />
or extract it and place an implant. These factors pertain to the patient’s health status, the condition of the tooth and<br />
periodontium, and treatment-related considerations.<br />
Patient-related factors include systemic and oral health, as well as patients’ comfort and perceptions about<br />
treatment. Tooth- and periodontium-related factors include pulpal and periodontal conditions, biological<br />
environmental considerations, color characteristics of the teeth, quantity and quality of bone, and soft-tissue<br />
anatomy. Treatment-related factors include an assessment of potential procedural complications, required<br />
adjunctive procedures and treatment outcomes data.<br />
The British Academy in Implant Dentistry (BAID)<br />
is Delighted to Announce<br />
the 2012 Dates for the Diploma Examination<br />
BAID Diploma<br />
Exam : Part 1<br />
Jordan Setting UK Setting<br />
Date 22 July 2012 10 August 2012<br />
Location Amman London<br />
Fee £360 £360<br />
Closing date 28 May 2012 25 June 2012<br />
| 60 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011<br />
BAID Diploma<br />
Exam : Part 2<br />
UK Setting<br />
Iraq Setting<br />
Date 10-11 August 2012 24-25 September 2012<br />
Location London Erbil<br />
Fee £950 £950<br />
Closing date 30 June 2012 30 July 2012<br />
For more information: BAID@live.co.uk, www.baid.org.uk
Effect of Teeth with Periradicular Lesions<br />
on Adjacent <strong>Dental</strong> Implants<br />
Shabahang S., Bohsali K, Boyne P., Caplanis N., Lozada J., Torabinejad M. September 2003<br />
Oral Surg - Oral Med - Oral Pathol - Oral Radiol - Endod. Vol. 96 No. 3 pp 321-326<br />
Introduction<br />
There are a number of factors that may cause areas of inflammation in the bone surrounding a root form implant,<br />
such as overheating the bone during surgery, fenestration of the osteotomy site, remaining root particles or foreign<br />
bodies and contamination of the implant surface with saliva or bacterial plaque during insertion. Whilst these factors<br />
can largely be avoided, with the increased use of implants placed amongst a natural dentition there is an increased<br />
risk of periradicular infections that may come into close contact with an adjacent implant. If such a lesion is capable of<br />
contaminating the implant surface with endotoxins then decontamination or biological repair, particularly of roughened<br />
surfaces, may be difficult and therefore osseointegration may be compromised along with long-term success.<br />
It was the purpose of this study to determine in a animal model the effect of periradicular lesions on the<br />
osseointegration of dental implants with or without treatment of the adjacent root and implant surface.<br />
Materials and Methods<br />
The second and third maxillary and mandibular premolars were extracted bilaterally in five adult beagle dogs and<br />
a total of 40 implants placed at an angle with their apices in close proximity (1-2mm separation) to the root apices<br />
of the remaining 1st and 4th premolars. The implants were Calcitek solid core or HA-coated with dimensions of<br />
3.75mm x 10mm. After a healing interval of 2 months, the implants were randomly allo cated to one of four groups<br />
each comprising 10 implants at which time they were surgically exposed and healing abutments placed. Each<br />
animal received weekly chlorhexidine applica tion and monthly prophylaxis during the experimental period in order<br />
to maintain healthy periimplant tissues. In group A the adjacent teeth were left untouched to serve as a negative<br />
control. In group B and C periradicular lesions were induced by opening the teeth to the oral environment for 7 days<br />
and then sealing the cavity for a further 8 weeks. The induced lesions were considered complete when there was no<br />
evidence of bone radiographically between the root and the implant apices. Each of the lesions group B and C were<br />
treated with conventional 2-visit endodontic procedures with intermediate calcium hydroxide dressings, however for<br />
group C the periradicular lesions were also surgically debrided and the implant surface cleaned with an air/powder<br />
abrasive unit (Prophy Jet, Dentsply) for 30 seconds and completed with a further 60 seconds of supersaturated citric<br />
acid application. The premolar teeth forming group D had periradicular lesions induced in the same manner as<br />
groups B and C, 5.5 months after implant placement. All animals were sacrificed at 7.5 months for histology. This<br />
was carried out blind and involved analysis of the apical 4mm of each opposing implant or tooth surface for the<br />
percentage osseointegration. Differences in the amount of osseointegration between groups, jaws and animals was<br />
evaluated using one-way analysis of variance (ANOVA) and the Pearson correlation coefficient to determine any<br />
significant differences between any of the various tooth and implants sites.<br />
Results<br />
Only one implant was lost to the study after an early failure. The average percentage integration for the groups was<br />
54%(A), 74%(B), 56%(C) and 68%(D). ANOVA revealed no differences between the four groups (P=0.518). After root<br />
treatment of the adja cent premolar the group B implants showed resolution of the bony defect in 87% of the sites<br />
whilst the surgical debridement group C this was reduced to 68%. No healing was observed in group D which had<br />
formed the positive controls.<br />
Discussion and Conclusions<br />
Within the limitations of this prospective study and the relatively small sample size, the surgically debrided sites<br />
appeared to do slightly less well than those only receiving conventional orthograde endodontics, the differences<br />
however were clinically insignificant with no tangible benefits from the detoxification process. Future studies could also<br />
determine whether or not bacterial contamination or endotoxins are present in the lesions adjacent to the implants.<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011| 61 |
The Effects of Smoking on Fracture Healing<br />
Sloan A., Hussein I., Maqsood M., Eremin O., El-Sheemy M. April 2010<br />
The Surgeon, Vol. 8 No. 2 pp 111-116<br />
Apart from premature death; smoking has been implicated in increased morbidity and can affect the dynamics of<br />
bone healing from a surgical viewpoint. The harmful effects of tobacco smoke would appear to be dose-related<br />
and smoking cessation has been recommended to reverse the damaging nature of the habit. This current review<br />
assesses the role of tobacco smoking in cellular activity and bone repair.<br />
Whether or not smoke is inhaled or released into the surrounding air, 95% of it is made up of volatile acids. Around<br />
500 gases are released including carbon monoxide, carbon dioxide, ammonia, hydrogen cyanide and benzene.<br />
The particulate phase accounts for the remaining 5% and approximately 3500 chemicals are produced including<br />
nicotine, anatabine and anabasine. The particulate phase also consists of tar, which contains the carcinogens.<br />
Depending on brand, around 2-3mg of nicotine and 20-30ml of carbon monoxide are inhaled from each<br />
cigarette. Nicotine is thought to be the addictive component in tobacco and causes increased platelet aggregation,<br />
decreased microvascular protacyclin levels and inhibition of the biological function of fibroblasts. The peripheral<br />
vasoconstriction caused by nicotine leads to decreased blood flow to the extremities and the chemical also has<br />
effects on plasma hormone levels with vasopressin, B-endorphin, adenocorticotrophic hormone (ACTH) and cortisol,<br />
all showing raised levels. Carbon monoxide arises from incomplete paper and tobacco combustion and displays<br />
a greater affinity (200-fold) for hemoglobin binding when compared to oxygen. The ensuing carboxyhemoglobin<br />
formed leads to hypoxia with 10 minutes of smoking leading to tissue-hypoxia for about 1 hour.<br />
Smoking is thought to affect the fracture healing process due to a reduced blood supply to the injury site although<br />
many theories exist relating to the role of free radicals, antioxidants and the attenuating effects of nicotine.<br />
High doses of nicotine have also been shown to be toxic to osteoblasts and calcitonin. In addition it is thought<br />
that other components in cigarette smoke can possess osteoblast-damaging properties. Clinical studies have<br />
highlighted the negative effects of smoking on lumbar fusion procedures and the union of open tibial fractures<br />
to a statistically significant degree. Surgical fixation has also been recommended for all fractures that are not<br />
amenable to closed reduction.<br />
Perioperative smoking cessation is generally advised although guidelines are vague, ranging from 1-28 days<br />
pre-operatively and 5-28 days post-operatively. A minimum of 12 hours cessation pre-operatively is necessary for<br />
the time required to clear CO levels from the human body. Although it is claimed that smoking causes irreversible<br />
systemic and local tissue damage, surgical treatment should not be denied to those who do not stop smoking,<br />
since cessation in itself cannot reverse all of the negative effects.<br />
Discussion and Conclusions<br />
This review suggests that many human and animal studies have demonstrated the negative effects of smoking on<br />
wound and fracture healing. It is thought that the effects are mediated by the vasoconstrictive, platelet-activating<br />
and aggregating properties of nicotine. In addition, at the cellular level, carbon monoxide has a hypoxic effect<br />
and hydrogen cyanide inhibits oxidative metabolism. Tobacco smoking has been strongly implicated in delayed<br />
healing and non-union of fractures. An evaluation of smoking history and cessation prior to surgery are advised<br />
so that the risks, complications and harmful effects of the habit can be suitably discussed and addressed.<br />
thth CAD/CAM & Computerized Dentistry<br />
International Conference<br />
6 thth<br />
CAD/CAM & Computerized Dentistry<br />
| 62 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011<br />
3 - 4 May 2012<br />
The Ritz-Carlton Hotel<br />
Dubai, UAE<br />
Dubai International<br />
Financial Center
www.aedsc.org
Meet us at<br />
AEEDC 2012<br />
Booth Booth 389+390 303<br />
mlutfi@m-lutfi.com
British Academy of Implant Dentistry in Iraq<br />
The British Academy of Implant Dentistry (BAID) has launched its scientific activities in the Middle East by starting the one year implant<br />
course “Comprehensive Evidence Based and Clinical Implantology Course” in Iraq. This course came to light following the hard work<br />
and great co-operation between BAID and the Iraqi <strong>Dental</strong> Association. Dr. Aljobory, the president of the dental association confirmed<br />
that this intensive eight module clinical implant course (six academic modules & two<br />
clinical modules) has been recognized by the Ministry of Health in Iraq as one of<br />
the post graduate diplomas, the Iraqi dentists can register as one of their degrees.<br />
On the other side, Dr. Maghaireh; the head of the international section in BAID has<br />
confirmed that this well structured implant course meets the General <strong>Dental</strong> Council-<br />
UK requirement in implant training in Britain and qualifies the course delegates to gain<br />
accredited CPD hours by the British Academy of Implant Dentistry upon finishing the<br />
course academic and clinical requirements and passing the course written exam.<br />
This course will also exempt the successful delegates from the first part of the Diploma<br />
in Implant Dentistry exams by the British Academy Of Implant Dentistry, and qualifies<br />
them to apply for the 2 nd and final part of these exams, which are run by a group<br />
of eminent implant clinicians and researchers such as Dr. Ibsy Hussain; the current<br />
president of the British Academy of Implant Dentistry and Prof. Marco Esposito, who is<br />
an internationally renowned researcher in implant dentistry.<br />
This course in its first version attracted 108 dentists from all<br />
around Iraq and was hosted in Erbil, the quiet but fascinating<br />
city who is famous with its very friendly and helpful people.<br />
The first module which took place on 25 th and 26 th November,<br />
featured prominent speakers from the University of<br />
Manchester, Nottingham Medical Centre and Eastman <strong>Dental</strong><br />
Institute and focused on the importance of treatment planning<br />
in implant dentistry, role of medical screening for implant<br />
patients and principled of surgical planning in implant therapy.<br />
Finally, it is worth mentioning that this course has received<br />
a very positive feedback from all of the delegates as well as<br />
the Ministry of Health observers, who commended the British<br />
academy of Implant Dentistry for delivering lectures high<br />
standard lectures.<br />
| 66 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011
EPTA: CRITIC’s TEST<br />
You could look at Epta for hours and still not unveil the secrets<br />
invisibly and mysteriously concealed in its faultless details.<br />
Meticulous design and simply beautiful materials.<br />
A brilliant confl uence of technology and art that enhances your<br />
talent and elevates your constant striving for perfection.<br />
Epta. Technology and design. Beyond semblance.<br />
AEEDC 2012<br />
Booth 308 - 311<br />
EPTA: THE ORIGINAL<br />
dentalArt_ love of details<br />
dentalArt spa<br />
Montecchio Precalcino<br />
Vicenza . Italy<br />
tel. +39 0445 802000<br />
www.dental-art.it<br />
Visit the “<strong>Dental</strong> Art Installations” on our<br />
website and discover latest Epta line<br />
compositions<br />
Middle East Area Manager<br />
Mahmoud Lutfi<br />
P.O.Box 641 11941 Amman Jordan<br />
Tel: +962 6 5656404/5<br />
Mobile: +962 7 95536867<br />
Email: mlutfi@m-lutfi.com
Richa <strong>Dental</strong> Store<br />
Organizes its 3 rd Implantology<br />
training trip to Milan, Italy<br />
From 15 th till 18 th of December 2011 RICHA DENTAL<br />
STORE have organized a trip to NOVAXA LEADER<br />
Course Center, Milano, Italy for 12 dentists from<br />
Lebanon accompanied by Dr. Chadi Richa where a<br />
large number of participants gathered from different<br />
countries to attend this course.<br />
The advanced course was held by Dr. Stefano Palmieri<br />
with the participation of our guest Dr. Mohamad<br />
Sartawi; well-known speaker and opinion leader in the<br />
Middle East Area.<br />
The Dentists who participated in this trip were:<br />
Dr. Pascale Habr, Dr. Georges Hallage, Dr. Rosy Brax,<br />
Dr. August Badawi, Dr. Alexandre Khairallah, Dr. Joseph<br />
Abi Nasr, Dr. Houssam Abou Hamdan, Dr. Mohamad<br />
El Masri, Dr. Jihad El Husseiny, Dr. Imad Mahfouz, Dr.<br />
Machhour Moumneh and Dr. Abed El Salam Baalbacky.<br />
The group also spent an enjoyable time discovering<br />
different Italian cities such as Milan, Venice and Rome.<br />
www.richadental.com<br />
MYDENT International<br />
Introduces New Ortho Boxes<br />
Mydent International has introduced Retainer and Denture<br />
Ortho Boxes, the latest in its line of DEFEND products.<br />
DEFEND Retainer Boxes, #OB-2000, are crush proof<br />
and feature a solid locking mechanism. These boxes<br />
are easy to clean and come in 5 assorted colors. The<br />
dimensions of these Retainer Boxes are 3” x 2½“ x 1”<br />
deep. They are packed 12 per box.<br />
Skema 8 – the Hallmark of<br />
Excellence<br />
Skema 8 is the complete Castellini treatment centre.<br />
Equipped with a selection of integrated specialist instruments<br />
and exclusive technologies, the unit offers both the freedom<br />
and flexibility of an all-inclusive concept and the solid values<br />
of Castellini design.<br />
Whatever the specialisation, from conservative dentistry<br />
to oral surgery, dental surgeons can turn to Skema 8 for<br />
immediate answers: a brushless micromotor capable of<br />
extensive torque values, the LAEC system for maximum<br />
efficiency and clinical safety in endodontic treatments,<br />
Autosteril for total hygiene and the latest Castellini surgical<br />
ultrasound handpiece.<br />
In terms of comfort and ergonomics, the hydraulic patient<br />
chair is an unrivalled example of design excellence, ensuring<br />
far more than simply synchronised movements. In all clinical<br />
situations, Skema 8 represents the peak of quality, working<br />
comfort and advanced performance - a thoroughbred.<br />
The Skema range of treatment centres, to which Skema<br />
8 belongs, is the result of innovation aimed at constantly<br />
raising the standards and quality of the unit to the advantage<br />
of the dental professional. Practicality is crucial in making<br />
advanced technologies immediately accessible. Each part of<br />
the Skema unit demonstrates Castellini’s ability to provide<br />
the surgeon with cutting-edge technology to ensure solutions<br />
which are as advanced as they are highly practical.<br />
Visit us at AEEDC Dubai 2012 / Booth 364 -Hall 7<br />
www.castellini.com<br />
DEFEND Denture Boxes, #OB-1000, feature high-impact plastic, 1 piece construction and contoured corners for ease of<br />
cleaning. The tight fitting lid holds 1 or 2 dentures, with dimensions of 3” x 2½” x 2” deep. DEFEND Denture Boxes are<br />
packed 12 per box in 4 assorted colors.<br />
These high quality DEFEND Ortho Boxes close completely and securely, have a durable hinge and keep contents safe. They<br />
are available through most dental dealers.<br />
Mydent International is dedicated to fully maintaining its brand promise: "To provide the healthcare professional with the<br />
highest quality infection control products, disposables, preventatives and impression material systems at affordable prices,<br />
supported by superior service and 100% Customer Satisfaction." DEFEND: Works Better. Lasts Longer. Costs Less.<br />
www.defend.com<br />
| 70 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011
Don’t miss the<br />
SOARIC at AEEDC<br />
Hall 6<br />
Booth 178,179, 202, 203
Silfradent Optimizes Tissue<br />
Regeneration<br />
Platelets: a Reservoir of<br />
Endogenous Growth Factors<br />
C.G.F.: Concentrated Growth Factors<br />
L.F. Rodella , M. Labanca, R. Rezzani<br />
An interesting clinical<br />
option for optimizing tissue<br />
regeneration is the use of<br />
platelet concentrate. Platelets,<br />
in fact, contain high quantities<br />
of growth factors, such as<br />
platelet-derived growth factor<br />
(PDGF), transforming growth<br />
factor TGF-ß1 and TGF-ß2,<br />
fibroblast growth factor (FGF),<br />
vascular endothelial growth<br />
factor (VEGF) and insulin-like<br />
growth factor (IGF), which<br />
stimulate cell proliferation,<br />
matrix remodeling and<br />
angiogenic processes during<br />
tissue regeneration.<br />
To date, numerous<br />
techniques using platelet<br />
concentrate have been<br />
developed in order to obtain<br />
different ratios of platelets,<br />
growth factors and fibrin<br />
matrix, among these PRP<br />
(Platelet Rich Plasma), PRF<br />
(Platelet Rich Fibrin) and<br />
CGF (Concentrated Growth<br />
Factors).<br />
CGF is an innovative<br />
method for producing a new<br />
generation of platelet concentrates that is characterized by a<br />
high concentration of autologous growth factors.<br />
It is produced by processing blood samples with a special<br />
blood phase separator (Medifuge MF200, Silfradent srl,<br />
Forlì, Italy) without the addition of anticoagulant factors. In<br />
particular, the potential of CGF is a solid consistency: in fact,<br />
it is a rich and dense fibrin matrix in which multiple platelet<br />
cell elements were “trapped” and some growth factors,<br />
i.e. TGF-ß1 and VEGF, were expressed. Moreover, it seems<br />
to be a potential source of CD34 positive cells, which are<br />
known to be recruited from blood to injured tissue and play<br />
a role in vascular maintenance, neovascularisation and<br />
angiogenesis.<br />
Regarding its applications, CGF was reported to have a<br />
good regenerative capacity and a high versatility on sinus<br />
and alveolar ridge augmentation. Nevertheless, these<br />
characteristics make CGF functional for different clinical<br />
applications in the field of tissue regeneration.<br />
www.silfradent.com<br />
| 72 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011
Brings simplicity to Endodontics<br />
WaveOne, from DENTSPLY Maillefer, is the new<br />
endodontic system designed to provide simplicity and<br />
efficiency to the root canal shaping procedure.<br />
The WaveOne motor works in a reciprocating mode with<br />
a large rotating angle in the cutting direction providing<br />
high efficiency, whereas a smaller angle in the reverse<br />
direction allows the WaveOne file to safely progress<br />
along the canal path, respecting the root canal anatomy.<br />
The optimised angles also reduce the risk of a screwing<br />
effect and file breakage.<br />
Single file technique<br />
The reciprocating technique makes it possible to shape<br />
most root canals using only one single WaveOne<br />
Nickel-Titanium (NiTi) file. No time is wasted changing<br />
NiTi instruments during the root canal shaping procedure<br />
and the global shaping time is decreased by up to 40%<br />
versus a traditional continuous rotary technique, whilst still<br />
providing premium quality root canal treatments.<br />
The WaveOne file geometry was conceived specifically to<br />
benefit from the optimised pre-programmed reciprocating<br />
movement of the WaveOne motor. The proprietary<br />
DENTSPLY M-Wire Nickel-Titanium technology provides<br />
additional flexibility and greater resistance to cyclic fatigue,<br />
the leading cause of file separation.<br />
Single patient use<br />
DENTSPLY Maillefer advocates single patient use as a<br />
new standard of care, by proposing the WaveOne<br />
reciprocating NiTi files exclusively in presterilized blister<br />
packs and fitted with a non autoclavable handle. The<br />
advantages are:<br />
• Simplicity<br />
• No risk of cross contamination<br />
• Optimal cutting efficiency<br />
• Better control of file breakage<br />
www.dentsplymea.com<br />
TIXOS: Manufactured by Direct<br />
Laser Metal Forming Technique<br />
TIxos implants line has been developed after years of<br />
research in cooperation with important National and<br />
International Universities and Research Centers. Tixos<br />
implants, manufactured through the exclusive and original<br />
technique of Direct Laser Metal Forming, are designed<br />
in 3D: around a very compact core an isoelastic surface<br />
is created, which replicates the bone spongy geometry;<br />
such a structure is highly mimetic, thus accelerating<br />
bone healing and enhancing faster osseointegration,<br />
as demonstrated by different in vitro and in vivo human<br />
studies*. The tridimensional geometry constituted by<br />
micro and macro-cavities of well defined sizes and form,<br />
interconnected by micro-pores, promotes bone formation.<br />
* References available on www.leaderitalia.it<br />
New Procedures for the<br />
Construction of the Implant Tunnel<br />
using the new PEC Piezo<br />
Expansion-Crest technique<br />
Luca Lancieri, freelancer in Genoa -Italy<br />
In recent years, the imperative of modern<br />
surgery has become minimal invasiveness and<br />
low biological impact. Piezo-electric surgical techniques fall<br />
perfectly into this category. In developing these procedures, I<br />
have devised a personal manoeuvre, which can be identified<br />
using the acronym PEC, Piezo Expansion-Crest. With this<br />
procedure, in one surgical session, it is possible to achieve<br />
the bone thickness necessary in order to insert one or more<br />
implants in crests which are atrophied due to post-extraction or<br />
post-traumatic infections.<br />
Today, patients are coming to our surgeries with two priority<br />
needs: dental reconstruction with a high level of aesthetic<br />
importance and the rapid morphological and functional<br />
restoration of missing teeth. It is obvious that it becomes a<br />
priority to have surgical procedures that make it possible to<br />
replace missing teeth with implants. For this purpose, it is<br />
possible to use piezo expansion-crest procedures.<br />
Let us now analyse this technique in detail: the expansion-crest<br />
makes it possible to create a permanent dilation suitable for<br />
accepting the implants, thereby making the surgical intervention<br />
quicker and more predictable. It is very important not to confuse<br />
the expansion-crest with the split-crest, two procedures which<br />
are apparently similar but totally different in terms of substance<br />
and results. The split-crest is performed by opening a partialthickness<br />
flap and using greenstick fracture of the crest and elastic<br />
deformation under tension of the disjointed bone gaps. The<br />
expansion-crest, however, is performed with a full-thickness flap and<br />
takes advantage of the viscoelastic properties of the bone, allowing<br />
a gradual separation of bone segments with permanent dilation<br />
and plastic deformation devoid of tension. The lack of tension on the<br />
implants is the key feature that makes it easier to stabilise the bone,<br />
reducing the risk of absorption and allowing a more predictable<br />
therapeutic outcome in the short, medium and long term.<br />
Operational difficulties in the execution of the separation of bone<br />
segments, especially in the jaw, are easily overcome by using the<br />
new PEC technique. As a matter of fact, the inserts that I have<br />
developed in cooperation with Silfradent, which provided the<br />
technical support necessary for their creation, make it possible<br />
to create the appropriate plastic dilation with minimum effort in<br />
the progression in depth and with the maximum preservation<br />
of the adjoining bone walls. The result is a kind of new implant<br />
tunnel site that is both a passive stabilisation and active bone<br />
proliferation site, extremely vibrant from a biological point of view<br />
for the construction of the new implant site.<br />
To this end, I have made a kit consisting of piezoelectric inserts<br />
with increasing diameter, calibrated for the most common implant<br />
procedures, with a non-working apex in order to avoid iatrogenic<br />
fenestrations and at the same time enable the tips to behave in<br />
a self-centring manner. The clinical case presented highlights the<br />
easy management of this procedure which, even in extremely<br />
critical clinical conditions, allows less experienced operators to<br />
easily insert fixtures in crests with marked atrophy which, with the<br />
usual procedures, would first require bone increase and then, at a<br />
later date, the implant could be performed.<br />
Today, using mini PEC procedures, it is possible to create<br />
implant tunnels without rotary cutters, creating biological<br />
conditions which are conducive to faster and more effective<br />
healing from both an aesthetic and functional point of view,<br />
improving the quality of the intra-operative stage and its course,<br />
satisfying today’s contextual demand for minimally invasive<br />
surgery with low biological impact.<br />
www.silfradent.com<br />
| 74 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011
HIGH PERFORMANCE<br />
REMARKABLE BALANCE<br />
Hu-Friedy’s outstanding combination of advanced technology<br />
and innovative design gives practitioners clinical precision and<br />
efficiency for a flawless performance, every time.<br />
Hu-Friedy’s superior standards for instrument quality and<br />
ongoing partnerships with industry thought leaders result in<br />
specialized instruments that help the endodontist perform with<br />
ever- increasing precision, efficiency and efficacy.<br />
INSTRUMENT<br />
MANAGEMENT<br />
ENDODONTIC<br />
INSTRUMENTS<br />
RUBBERDAM<br />
CLAMPS<br />
Hygiene must be the top priority<br />
in your practice for the health of<br />
your patients and assistants.<br />
Our seamless and traceable<br />
hygienic chain prevents infection<br />
and protects both your assistants<br />
and your patients by cleaning<br />
instruments safely in the Hu-Friedy<br />
instrument cassette. Unnecessary<br />
handling is now in the past.<br />
Hu-Friedy products are<br />
individually handcrafted for high<br />
performance and remarkable<br />
balance.<br />
Made from a specially blended<br />
steel alloy for maximum durability<br />
and resiliency, our instruments<br />
have uniform tapers for smooth<br />
condensing and spreading action<br />
and exceptional strength throughout<br />
the working ends.<br />
Matte-finish Satin Steel clamps<br />
reduce glare and improve field of<br />
vision.<br />
Our Satin Steel rubber dam clamps<br />
are created with a very bright<br />
beginning - each one is carefully<br />
designed and handcrafted for<br />
superior strength and corrosion<br />
resistance. The dull, matte-finish<br />
comes next.<br />
For more information on our products please<br />
visit our website WWW.HU-FRIEDY.EU<br />
or contact us by e-mail: INFO@HU-FRIEDY.EU<br />
How the best perform<br />
©2011 Hu-Friedy Mfg. Co., LLC. All rights reserved.
Denar ® Mark 300<br />
Series Articulators<br />
Whip Mix Restorative<br />
Oral Health Division is<br />
pleased to announce the<br />
introduction of the next<br />
generation articulators,<br />
the Denar ® Mark 300<br />
Series Articulators. The<br />
Mark 300 Series offers<br />
interchangeability among this<br />
series of instruments and are<br />
factory set to within 20 microns of accuracy. The Mark<br />
300 Series is comprised of the Mark 330, Mark 320 and<br />
Mark 310 articulators.<br />
The features of these new articulators include:<br />
• Mark 330 is semi-adjustable with adjustable condylar<br />
inclination, progressive side shift, and immediate side shift<br />
• Mark 320 is semi-adjustable with adjustable condylar<br />
inclination and fixed progressive side shift<br />
• Mark 310 is fixed settings for condylar inclination and<br />
progressive side shift<br />
• All are compatible with the DenarSlidematicfacebow<br />
• All have positive centric latch that allows the upper and<br />
lower members to be separated or positively locked<br />
together in centric relation<br />
• All have built-in magnetic mounting system<br />
• All have unobstructed lingual access<br />
www.pirotrading.com<br />
Jet Carbides<br />
from Beavers<br />
For over 100 years Beavers <strong>Dental</strong> has been providing the<br />
quality and performance you’ve come to expect. All Jet<br />
Carbides are manufactured using a high grade Tungsten<br />
Carbide with the tolerance on each shank adjusted to ensure<br />
a positive non-slip fit into any handpiece. Jet Carbides are<br />
produced in our Rotary Technology Innovation Center using<br />
the very latest in equipment and are subjected to vigorous<br />
quality control to comply to the most exacting standards. The<br />
unique blade geometry of the Jet Carbide means you’ll get a<br />
smoother cut and cleaner preparation every time!<br />
www.pirotrading.com<br />
Whitening Lamp 2<br />
from WHITEsmile<br />
The new WHITEsmile ® Whitening<br />
LAMP is designed for even more<br />
advanced in-office tooth whitening. The Blue<br />
LED technology with high intensity spectrum<br />
light 465nm wavelength and an output of<br />
30.000 mW/cm² (3 LED’s, total of 30 W)<br />
allows safe and effective tooth whitening<br />
treatments. No harmful ultraviolet light and<br />
heat development ensures patient safety and<br />
comfort and therefore decreases the risk of<br />
developing tooth sensitivity.<br />
www.pirotrading.com<br />
CrosstexSecureFit<br />
CrosstexSecureFit masks meet FDA requirements for ASTM*<br />
F2100-11 Performance Class Specifications. ASTM material<br />
testing standards include mask performance requirements for<br />
fluid resistance, filtration value, breathability and flammability<br />
of mask materials. ASTM classifications include three levels of<br />
protection, with each level relating to the ability of the material<br />
to provide fluid resistance and barrier protection for the wearer.<br />
Crosstex offers a wide variety of mask designs, fit and filtration<br />
to match the protection needs for each procedure or risk level,<br />
including ASTM Level 1 (Isofluid ® ), Level 2 (Procedural) and<br />
Level 3 (Ultra). All Crosstex ASTM rated masks are fluidresistant,<br />
odorless, latex-free, fiberglass-free, with comfortable<br />
outside attached earloops, downward pleated outer folds, and<br />
offer a soft tear-resistant white inner layer.<br />
G-Files <br />
NEW rotary NiTi glide path<br />
instrumentation!<br />
www.pirotrading.com<br />
Glide path development is an essential but time-consuming<br />
step in endodontic treatment.<br />
G-Files are based on an innovative design to help the<br />
clinician safely save time in endodontic procedures. The<br />
superior cross-section of the G-Files combines efficiency<br />
and innovation. Along the length of the instrument, the<br />
G-File has cutting edges on three different radiuses leaving<br />
a large and efficient area for upward debris removal.<br />
Used after hand files have measured working length,<br />
G-Files safely enlarge the glide path in preparation for RCT<br />
with rotary instrumentation system.<br />
Avantages:<br />
• Superior flexibility due to their small instrument diameters<br />
(n° 12 and n° 17) and their slight .03 taper<br />
• Non-working (safety) tip<br />
• Electro-polished to optimize their efficiency in apical<br />
progression while aiding in upward debris removal.<br />
• Enhanced circulation of the irrigation solution beginning<br />
from the initial phase of treatment<br />
• Quickly and safely enlarge the canal passageway to the apex<br />
www.micro-mega.com<br />
| 76 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011
IRAQ<br />
www.lacalut.info<br />
Oral Care System from Germany<br />
Special protection against:<br />
• Bleeding gums<br />
• Gum problems<br />
• Periodontal disease<br />
LABORATOIRE<br />
O<br />
Pro Health Line<br />
Iraq - Erbil City<br />
Dr. Raman M. Asad<br />
+964 (0) 750 454 4479<br />
Raman.Jaff@prohealthline.com<br />
Emirates Scientific Drug Bureau<br />
Iraq - Baghdad City<br />
Dr. Mustafa Abdul Rasool<br />
+964 (0) 771 33 1978<br />
Mustafa.wayyes@prohealthline.com
Two Minutes with<br />
Prof. M. Sherine<br />
Elattar<br />
Mohamed Sherine Ibrahim Elattar was born in Alexandria Egypt, April 18 th ,<br />
1955. He went to the British boys school, followed by Ramleh secondary school,<br />
then the Faculty of Dentistry at Alexandria University. Prof. Elattar has only one<br />
brother; Shamel. His late father was the first graduate from Alexandria <strong>Dental</strong><br />
School, where the class at that time comprised of only two students. He saw in his<br />
late father an inspiration and always wanted to accomplish what he didn’t do as<br />
a dentist. He was appointed as a clinical instructor at Alexandria <strong>Dental</strong> School,<br />
and then got married to his wife Nermine, while going through his master’s<br />
degree. He believed that each of us should try his utmost to be unique in his field;<br />
therefore he went further to gain higher clinical training program in Pittsburgh,<br />
PA, USA. Nowadays, he is in the process of putting the final fine touches on his<br />
new book : “ HOW TO BECOME A UNIQUE DENTIST” which includes lots of<br />
inspirational tips & hints to young dentists in addition to sharing his clinical up to<br />
Profile<br />
date experience skills with the readers<br />
Prof. Mohamed Sherine Ibrahim Elattar<br />
BDS, MSc, PhD Prosthodontics<br />
• President of AOIA<br />
• Diplomat, ICOI, Section Manager, ICOI Middle-East<br />
• Ex-Dean, Faculty of Dentistry, Pharos University<br />
• Chapter Author: <strong>Dental</strong> Implantation and<br />
Technology, Nova Publishers, USA, 2009<br />
Why did you choose to be an implant dentist?<br />
I fell in love with implants, while doing my first case at my<br />
school in Pittsburgh…I saw how much implants changed<br />
my patient’s life<br />
What are the best/worst aspects of your job?<br />
Stress, as you do your best to satisfy your patients, and try<br />
to do a perfect job all the time. It’s never easy to reach<br />
perfection, and it would be great if you are close<br />
Where do you live?<br />
Alexandria, Egypt<br />
What do you drive?<br />
A beautiful (and I mean it) Chinese car<br />
What drives you?<br />
Love to all my surroundings<br />
What’s your favorite food?<br />
kofta<br />
What’s your hobby?<br />
Dentistry and football<br />
What’s your favorite film?<br />
Mr. Bean (going for a holiday)<br />
Favorite holiday destination?<br />
Elgona, hurgada, Egypt<br />
What inspires you?<br />
A real smile of appreciation from a student, colleague or<br />
a patient<br />
What really annoys you?<br />
A bad case that I did leading to an unsatisfied patient<br />
What keeps you awake at night?<br />
A treatment plan for a tough case<br />
What makes you smile?<br />
A family gathering with my wife, daughters and their husbands<br />
What is your best characteristic?<br />
My mother always tells me that I am an unusual person. I take<br />
the best part of everybody and everything, ignoring the bad<br />
parts… easily satisfied<br />
Worst fault?<br />
Worrying too much about other people<br />
Can you describe yourself in three words?<br />
Simple, loving and sincere<br />
What do you do to relax?<br />
Stay alone, watch a funny movie<br />
If you weren’t a dentist, what would you have liked to<br />
have been?<br />
Restaurant owner<br />
Do you read and recommend <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong><br />
regularly?<br />
II honestly SMILE when I receive each new edition<br />
What would be your motto in life?<br />
Don’t look for money, just do your work and money will look for<br />
you<br />
| 78 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011
Getting to the root of the problem.<br />
As a world leader in the micro-design of Endo instruments, precision is our business. Our<br />
Revo-S NiTi rotary system takes precision to new levels. With an easy 1-2-3 sequence,<br />
the Revo-S NiTi system features a finely crafted, asymmetrical cross-section for increased<br />
flexibility. The snake-like movement of the instrument within the canal reduces the stress<br />
on the file and minimizes the risk of separation. Easy, effective and unlike anything else.<br />
MICRO-MEGA ® Revo-S <br />
Join the REVOlution at www.revo-s.com<br />
Revo-S is a registered trademark and “Your Endo Specialist” is a trademark of MIcro-Mega Ltd.
21 - 24 September 2011 | Dbayeh, Lebanon<br />
BIDM & DGZI 2011<br />
Prepared by Dr. Ronald Younes<br />
The Beirut International <strong>Dental</strong> Meeting 2011 (21<br />
st Annual<br />
Scientific Congress of the Lebanese <strong>Dental</strong> Association) was<br />
held in Beirut, Lebanon at the Congress Palace – Dbayeh<br />
from 21 till 24 September 2011. The LDA also collaborated<br />
with the German Association of <strong>Dental</strong> Implantology (DGZI)<br />
for this global congress and merged the 8th Arab-German<br />
Implantology meeting with the BIDM 2011, therefore<br />
holding it simultaneously in the same venue.<br />
The BIDM 2011 featured more than 120 scientific sessions<br />
facilitated by nearly 100 speakers, hailing from American,<br />
European and Arab countries, in addition to Lebanese<br />
lecturers, covering a wide array of specialized subjects<br />
within the numerous dental disciplines.<br />
The four-day Scientific Program, entitled<br />
“Exploring the<br />
evidence”, focused on treatment planning as a means<br />
of addressing the challenges commonly faced by dental<br />
clinicians – how to reach<br />
“a patient’s wish” and “the perfect<br />
result”. The world-renowned speakers offered pragmatic<br />
solutions and shed light on state-of-the-art techniques for<br />
issues ranging from simple day-to-day clinical obstacles to<br />
complex specialized demanding cases, making this congress<br />
the most scientifically advanced in the Middle-East.<br />
8 Pre-congress ‘step-by-step’ courses and hands-on<br />
workshops took place on Wednesday September 21 st at<br />
the Congress Palace during which the participants got to<br />
experience first-hand some of the latest innovations in the<br />
world of dentistry.<br />
More than 2300 delegates and 4.000 visitors from around<br />
the world attended the 2011 Beirut International <strong>Dental</strong><br />
Meeting, benefiting from 4 parallel ongoing conferences in 4<br />
different halls at any given time, a wide range of attractions<br />
including multiple oral sessions, 4 live video transmissions,<br />
research sessions in Clinical and Basic Research, a young<br />
podium where post-grad students got to present their cases.<br />
More than 200 international and local exhibitors occupied<br />
a commercial exhibition space of more than 3000 square<br />
meters in total throughout the period of the congress with<br />
products covering most of the dentists’ needs.<br />
| 80 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011
The LDA announced the dates for the BIDM<br />
2012 (very promising scientific program),<br />
which will be held in collaboration with the<br />
French <strong>Dental</strong> Association and the FDI World<br />
<strong>Dental</strong> Federation from the 19 th till the 22 nd<br />
of September 2012 at the Congress Palace –<br />
Dbayeh, Beirut, LEBANON<br />
For more info, please visit the BIDM official<br />
website: www.bidm-lda.com<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011| 81 |
Come visit us at AEEDC 2012 at our Piro Trading booth # 206 - 212 & 221 - 227
CHOICE 2 Veneer Cement<br />
Choice 2 is a light-cured veneer luting cement designed<br />
specifically for superior color stability and esthetics.<br />
the only color stable system available on the market<br />
highly filled to enhance the strength of the restoration<br />
offered in a range of shades which mimics the natural dentition<br />
THE FIRST<br />
DEDICATED<br />
PRIMER FOR<br />
ZIRCONIA<br />
The Choice 2 system provides all the necessary materials to build a<br />
solid restorative foundation from the bottom up and provide optimal<br />
esthetics from the top down.<br />
Z-PRIME PLUS<br />
Zirconia - Alumnia -Metal Primer<br />
Z-PRIME Plus significantly enhances<br />
bond strengths to Zirconia, Alumina,<br />
and Metal substrates more than any<br />
other surface primer on the market!<br />
For more information email intl@bisco.com or visit www.bisco.com<br />
Building <strong>Smile</strong>s From The Bottom Up
27 October 2011 | Dubai, UAE<br />
2011<br />
3<br />
rd Aesthetic Dentistry<br />
MENA Awards<br />
The Aesthetic Dentistry MENA Awards 2011 is one unique completion in which dentists from 12 countries compete<br />
with their professional treatment achievements. 96 clinical cases have been submitted and judged by independent Jury<br />
panel form 6 countries.<br />
Dr. Ajay Juneja from UAE won two categories as best case in Cosmetic Aesthetic and Multidisciplinary, while Dr.<br />
Thamer Theeb of Jordan won the “I Love My Dentist” award, this award was chosen by the public out of six finalists<br />
from a total of 222 dentists representing 21 countries. The six finalists were chosen by the public who casted 5,800 votes.<br />
“These awards are the highlights of the work of the dental profession in the Middle East and other countries,” explained<br />
CAPP managing director Dr. Dobrina Mollova, organizer of the 3rd <strong>Dental</strong>-Facial Cosmetic International Conference.<br />
Dr. Aisha Sultan, head of the <strong>Dental</strong> Department of the Ministry of Health and president of Emirates <strong>Dental</strong> Society,<br />
commented: “The MENA award is the first award in the region and the world that aims to appreciate and recognize<br />
the skills of dental practitioners. Today and for the third year in a row, this award has become a very well known event<br />
amongst dentists in Asia, Africa and the Middle East.”
28 - 29 October 2011 | Dubai, UAE<br />
3232<br />
rd nd <strong>Dental</strong> - Facial Cosmetic<br />
International Conference<br />
The organizers, CAPP and Emirates <strong>Dental</strong> Society achieved for the 3<br />
rd time great record of attendance during the DFCIC 2011, and<br />
established a reputation as the industry’s leading international conference. Jumeirah Beach Hotel hosted 756 participants in an elegant<br />
atmosphere.<br />
Bringing together industrial leaders and professional practitioners, the conference not only delivered extensive scientific knowledge<br />
from across the globe but gave way for an excellent opportunity to present the latest advancements and developments within the Facial<br />
Cosmetics practice.<br />
The 3<br />
rd dental Facial not only opens the door to discussion and learning for this knowledge hungry region but allows the participants<br />
to build their skills and use the opportunity for networking and sharing experiences in the application of technology throughout the<br />
learning cycle - from primary and secondary education through to professional development and lifelong learning.<br />
The international event brought together the best experts, speakers and specialists in the different fields of dental and facial cosmetic<br />
from Middle East, UK, France, Germany, Switzerland, Italy, Norway and Austria. Participants were extremely happy with an excellent<br />
program and highly reputable speakers. This was proven from participants’ feedback that the sessions they attended were greatly<br />
appreciated. This was based on the evaluation forms from all participants, showing an average score of 4.1 out of 5 for informative<br />
program and Lectures.<br />
A <strong>Dental</strong> Technician Parallel Session was organized at the same time of the conference, where 47 participants joined the conference<br />
from the Lebanese <strong>Dental</strong> Laboratories Association.<br />
The conference hosted as well the first “Arab <strong>Dental</strong> Laboratory Union” Meeting to discuss future plans.
AUSGABE 1.2010<br />
Meet us at AEEDC<br />
Hall 7 booth 56<br />
Bovine Bone<br />
Straight Implant<br />
SLS-Straight Implant<br />
Synthetic Bone<br />
Tapered Implant<br />
Pericardium Membrane<br />
Sinus-Lift Implant<br />
Collagen Membrane<br />
Soft-Bone Implant<br />
Soft Tissue Graft<br />
<strong>Dental</strong> implants<br />
Collagen Fleece<br />
Collagen Cone<br />
Regeneratives<br />
Connecting the pieces<br />
Looking for<br />
Distributors in Middle East<br />
Dentegris Deutschland GmbH<br />
Grafschafter Straße 136 | DE-47199 Duisburg<br />
Mail: info@dentegris.de | www.dentegris.de
D.T. LIGHT-POST ® X-RO ®<br />
ILLUSION <br />
Translucent quartz fiber<br />
COLOR ON DEMAND FIBER POST<br />
The smartest post you could envision<br />
RADIOPAQUE +<br />
ANATOMICAL<br />
RELIABLE<br />
AESTHETIC<br />
EASY TO USE<br />
D.T. LIGHT-POST X-RO Radiopacity<br />
Courtesy of Dr Cheleux University of Toulouse<br />
X-RO ®<br />
50 % more radiopaque<br />
20 % stronger<br />
30 % more retentive
The first and unique dental implant<br />
in the world fabricated with<br />
Direct Laser Metal Forming technique<br />
by fusion of titanium microparticles !<br />
Laser forming methods allow the<br />
fabrication of implants with a very<br />
compact core and an isoelastic<br />
surface, which replicates the bone<br />
spongy geometry.<br />
The tridimensional network<br />
of the surface, constituted by<br />
interconnected cavities, promotes<br />
faster bone formation*.<br />
*References available upon request<br />
The 16 th UAE International <strong>Dental</strong> Conference<br />
& Arab <strong>Dental</strong> Exhibition<br />
See you in Dubai<br />
booth n. 318<br />
Jan 31 st – Feb 2 nd 2012<br />
Dubai International Convention & Exhibition Centre (DICEC)<br />
LEADER ITALIA srl via Aquileja 49, 20092 Cinisello B. MI ITALY<br />
ph +39 (0)2 618651 - fax +39 (0)2 61290676<br />
www.leaderitalia.it - export@leaderitalia.it
25 - 28 October 2011, Cairo - Egypt<br />
15<br />
th<br />
International<br />
EDA Congress<br />
The 15<br />
th International EDA Congress has ended on a very high note. It has exceeded all<br />
our expectations and reached a very high level of participation and attendance with over<br />
120 Lecturers and over 6200 attendants.<br />
This being the first <strong>Dental</strong> Congress to be held after the Egyptian revolution last January,<br />
and amidst the turbulent and unsettled atmosphere prevailing since, it was feared<br />
that many participants would be reluctant to make the trip and take the risk in such<br />
circumstances, but fortunately, this has proved not to be the case, and those who came<br />
never regretted making the trip.<br />
All 17 workshops, pre-congress, during the congress and post-congress were fully booked<br />
and attended. The attendants were fully satisfied and full of praise for the organizing teams.<br />
For the first time in Egyptian <strong>Dental</strong> Congresses, there has been a live transmission<br />
Via Satellite of a surgical operation in the Main Hall, which was highly attended and<br />
enthusiastically received.<br />
The accompanying trade exhibition was again a very successful one, and the exhibition<br />
area in the Intercontinental City Stars Hotel (3800m<br />
2 ) was a very spacious one and<br />
enabled all traders to be with us.<br />
The next EDA International <strong>Dental</strong> Congress will be held on the 6<br />
th of November 2013,<br />
when we hope to see you all again as well as many more who did not attend this<br />
Congress. Thank you all very much indeed, and see you in two years time.
17 November 2011, Amman - Jordan<br />
1<br />
st <strong>Smile</strong> <strong>Dental</strong> Symposium<br />
“<strong>Dental</strong> Implants: Is Quicker Always Better?”<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> in co-operation with the scientific committee in the Jordan <strong>Dental</strong> Association launched its<br />
1 st <strong>Smile</strong> <strong>Dental</strong> Symposium on Thursday 17<br />
th November 2011 in Amman-Jordan. This symposium aimed to look<br />
into one of the advanced topics in dental implantology: The Ttiming in Implant Dentistry. This scientific event hosted<br />
a group of prominent implant speakers with each of them presenting the up-to-date evidence based and clinical<br />
tips and hints on implant placement in post extractive sockets and timing of loading dental implants; Dr. Hassan<br />
Maghaireh from the University of Manchester, Prof. Marco Esposito, the Editor-in-Chief of The European <strong>Journal</strong><br />
of Oral Implantology, Prof. Alexandre Khairallah from the Lebanese University and Prof. M. Sherine Elattar, the<br />
President of The Alexandria Oral Implantology Association.<br />
This one-day event featured a high-quality scientific program along with an up-to-date and advanced dental show.<br />
91% of delegates rated the symposium ‘excellent’, 97% of delegates agreed that this symposium had provided them<br />
with evidence based and clinical tips which they can apply in their day to day dental implant practice. All of the<br />
delegates confirmed that they would recommend this symposium to their friends and colleagues.<br />
The day started with Dr. Maghaireh<br />
who highlighted different clinical<br />
scenarios where the timing of the<br />
implant insertion and the incorporation<br />
of the superstructure play an essential<br />
role for the overall treatment outcome.<br />
He also illustrated clinical philosophies,<br />
protocols, tips and hints aiming to<br />
help dentists to achieve predictable<br />
highly aesthetic results in implant dentistry. Delegates were<br />
shown how to turn time into an ally rather than an enemy.<br />
Dr. Maghaireh also covered the clinical pros and cons of<br />
immediate, early and delayed immediate placement in his<br />
second lecture and went on his third lecture to present the<br />
various loading protocols in implant dentistry, illustrating<br />
various clinical cases on each technique.<br />
Prof. Esposito, in return presented<br />
the most up to date systematic reviews<br />
he conducted on placing dental<br />
implants in fresh extraction sockets<br />
(Immediate, Immediate-Delayed<br />
and Delayed Implants) and timing of<br />
restoring the dental implants with the<br />
final prosthesis. He discussed in his<br />
two lectures the significant difference<br />
between various clinical approaches in connection with the<br />
implant treatment. Delegates had the opportunity to discuss<br />
the random controlled trials conducted in the last three to five<br />
years on timing and loading of dental implants.<br />
Prof. Khairallah presented his lecture:<br />
“The Importance of 3D Radiographic Input<br />
in Planning Advanced Cases” which was<br />
specially prepared for this symposium and<br />
presented for the first time at this advanced<br />
implant symposium. Pof. Khairallah<br />
presented a series of radiological and<br />
technological enhancement showing<br />
all the benefits that a clinician can get<br />
during planning for immediate implant(s) placement surgery<br />
and furthermore, in making a decision on the timing of fitting<br />
prosthetic superstructure. Delegates were also given a unique<br />
opportunity to develop their skills in reading and analyzing Cone<br />
Beam CT scans and the various 3D planning software.<br />
Last, but not least was with Prof. Elattar,<br />
who is the author of several articles<br />
addressing the timing of implant insertion<br />
and loading and the founder of a new<br />
definition: ”Early Osteotomy “. In his lecture,<br />
Prof. Elattar focused on the prosthetic<br />
challenges which might face the dentist<br />
while restoring an immediate loading<br />
case in the aesthetic region. He presented<br />
clinical situations that would frequently face most practitioners,<br />
and would ultimately achieve better aesthetics if treated with<br />
immediate loaded implants. Prof. Elattar, who is in the final stages<br />
of publishing his new book; “ HOW TO BECOME A UNIQUE<br />
DENTIST” gave our course delegates some of his inspirational<br />
clinical and practice management tips in addition to sharing his<br />
clinical up to date experience skills which were very well received.<br />
| 92 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011
In the evening, the symposium delegates celebrated the<br />
social event – “<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> 5 th anniversary” at the<br />
Gala dinner party which took place at the Landmark hotel<br />
in Amman. We are proud at <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> that this<br />
anniversary celebration took place under the patronage of<br />
the president of the Jordan <strong>Dental</strong> Association; Dr. Azem<br />
Qadoomi, who has exchanged trophies and certificates<br />
with the speakers and the editorial team of <strong>Smile</strong> <strong>Dental</strong><br />
<strong>Journal</strong>. <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> is also delighted to have<br />
the president of the scientific committee in the Jordanian<br />
<strong>Dental</strong> Association; Dr. Mohammad Sartawi, and the<br />
president of the Palestinian <strong>Dental</strong> Implant Society; Dr.<br />
Marwan Al-Qasem among our honorary guests. The<br />
symposium was also well supported by dental and local<br />
private companies who have sponsored the prizes for the<br />
quiz show during the Gala dinner. So many presents were<br />
awarded to the course delegates during our 5 th anniversary<br />
celebration, some which were tickets to the 6 th CAD/CAM<br />
congress in Dubai in May 2012.<br />
<strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011| 93 |
Finally, we would like to thank the following<br />
companies for their support during<br />
organizing and planning our 1 st <strong>Dental</strong><br />
Implant Symposium:<br />
• Ferrari <strong>Dental</strong> Clinics & Labs (Inman Aligner)<br />
• Eastern Medical Laser w.l.r<br />
• Leader Italia srl (Tixos Implants)<br />
• Basamat Pharmadent<br />
• Bronze Medical Supplies Co. (BMSC)<br />
• Al-Shumukh (ImPLASA Implants)<br />
• CAPP MEA<br />
• Dara for Computers<br />
• Milano Sport<br />
• Budy Pendant<br />
| 94 | <strong>Smile</strong> <strong>Dental</strong> <strong>Journal</strong> | Volume 6, Issue 4 - 2011
implant maintenance made<br />
easy, efficient & effective!<br />
Solid<br />
TiTanium TipS<br />
• Same material as abutments<br />
• Safely glide over surfaces<br />
• Easily remove debris<br />
• 7 Familiar pattern designs<br />
Visit us<br />
• Sterilize by any method<br />
during aEEdC:<br />
piro Trading intl<br />
• Easy to adapt<br />
Booth #209
AEEDC 2012<br />
Booth 329<br />
Middle East Area Manager<br />
Mahmoud Lutfi<br />
P.O.Box 641 11941 Amman Jordan<br />
Tel: +962 6 5656404/5<br />
Mobile: +962 7 95536867<br />
Email: mlutfi@m-lutfi.com
AEEDC 2009<br />
Stand # 309-407<br />
IDS 2009<br />
Booth Hall No. 11.2303<br />
Stand # R-040 - S-041<br />
Aisle R<br />
AEEDC 2012<br />
Middle East Area Manager<br />
Middle<br />
Mahmoud<br />
East Area<br />
Lutfi<br />
Manager<br />
Tel: +962 6 5656404/5<br />
Mahmoud Lutfi<br />
Fax: +962 6 5656402<br />
Tel: +962 6 5656404<br />
Mob: +962 7 95536867<br />
Mob: +962 7 95536867<br />
E-mail: mlutfi@go.com.jo<br />
E-mail: mlutfi@go.com.jo
PowerPen<br />
International<br />
Dealers Welcome<br />
info@quicklase.com<br />
Cordless<br />
Soft Tissue<br />
Management<br />
Diode Laser<br />
Specifications:<br />
Dimensions length 195mm (with battery)<br />
Diameter 18 mm<br />
Weight < 200g, with battery attached<br />
Laser Diode Wavelength 810±10 nm<br />
Output Power 4w (Auto power)<br />
Operation Mode, continuous wave (CW)<br />
Fibre Tip Diameter 400 um / 200um<br />
Aiming Beam diode 650 nm, < 1mW output<br />
Battery Rechargeable 3.2 volt DC, 600mAh<br />
Laser specialist since 1992<br />
Can also be used with<br />
Whitening<br />
Systems<br />
UK & International<br />
+44 1227 780009<br />
PPEN2WQL240511RG
Quality<br />
Quality and guarantee of<br />
effectiveness and trouble-free<br />
process of prosthetics is the main<br />
duty of Implasa Höchst company.<br />
Research & Development<br />
Is there a limit in development of<br />
dental practice? The answer to this<br />
question opens by itself, if we take a<br />
look to the way which the Implasa<br />
Höchst company passed for 10 years<br />
in the field of the newest technologies<br />
of the cure and prosthetics of teeth.<br />
Materials & Technologies<br />
The high-quality materials +<br />
constantly improving technologies =<br />
the guarantee of our quality and<br />
your success<br />
Production Cycle<br />
ImPlasa Höchst company specialists<br />
diligently control the quality of the<br />
released production at all the stages<br />
of technological process<br />
and production.<br />
Micros<strong>copy</strong><br />
The surface of implants is prepared<br />
by unique technology of ImPlasa<br />
Höchst company, named<br />
ImPlapore, which allows to reach<br />
minimal traumatizing in the area of<br />
implant installation, and such way<br />
maximally eases the<br />
osseointegration process.<br />
The Sole Representative in the<br />
Middle East and Africa<br />
E: dr.munther@implasa.de<br />
KSA<br />
Saudi Swiss<br />
Consultant <strong>Dental</strong> Center<br />
Tel: +96638898714<br />
professor_agha@yahoo.com.ca<br />
Lebanon<br />
Kingdom Medical &<br />
<strong>Dental</strong> Instruments<br />
Tel: +961 6 426462<br />
kingdom_est@hotmail.com<br />
Syria<br />
Kingdom Medical &<br />
<strong>Dental</strong> Instruments<br />
Tel: +963 21 5732052<br />
majedajami01@hotmail.com<br />
Turkey<br />
ASYA DENTAL<br />
Tel: +902164957287<br />
gulcan_celebi@mynet.com<br />
UAE Dubai<br />
Bright <strong>Smile</strong><br />
Medical Equipment<br />
Tel.: +971 4 4508423<br />
brightsmile.me@gmail.com
Quality<br />
Quality and guarantee of<br />
effectiveness and trouble-free<br />
process of prosthetics is the main<br />
duty of Implasa Höchst company.<br />
Research & Development<br />
Is there a limit in development of<br />
dental practice? The answer to this<br />
question opens by itself, if we take a<br />
look to the way which the Implasa<br />
Höchst company passed for 10 years<br />
in the field of the newest technologies<br />
of the cure and prosthetics of teeth.<br />
Materials & Technologies<br />
The high-quality materials +<br />
constantly improving technologies =<br />
the guarantee of our quality and<br />
your success<br />
Production Cycle<br />
ImPlasa Höchst company specialists<br />
diligently control the quality of the<br />
released production at all the stages<br />
of technological process<br />
and production.<br />
Micros<strong>copy</strong><br />
The surface of implants is prepared<br />
by unique technology of ImPlasa<br />
Höchst company, named<br />
ImPlapore, which allows to reach<br />
minimal traumatizing in the area of<br />
implant installation, and such way<br />
maximally eases the<br />
osseointegration process.<br />
The Sole Representative in the<br />
Middle East and Africa<br />
E: dr.munther@implasa.de<br />
KSA<br />
Saudi Swiss<br />
Consultant <strong>Dental</strong> Center<br />
Tel: +96638898714<br />
professor_agha@yahoo.com.ca<br />
Lebanon<br />
Kingdom Medical &<br />
<strong>Dental</strong> Instruments<br />
Tel: +961 6 426462<br />
kingdom_est@hotmail.com<br />
Syria<br />
Kingdom Medical &<br />
<strong>Dental</strong> Instruments<br />
Tel: +963 21 5732052<br />
majedajami01@hotmail.com<br />
Turkey<br />
ASYA DENTAL<br />
Tel: +902164957287<br />
gulcan_celebi@mynet.com<br />
UAE Dubai<br />
Bright <strong>Smile</strong><br />
Medical Equipment<br />
Tel.: +971 4 4508423<br />
brightsmile.me@gmail.com