Controlling Indirect Selection under Healthcare Reform - Society of ...
Controlling Indirect Selection under Healthcare Reform - Society of ...
Controlling Indirect Selection under Healthcare Reform - Society of ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
108<br />
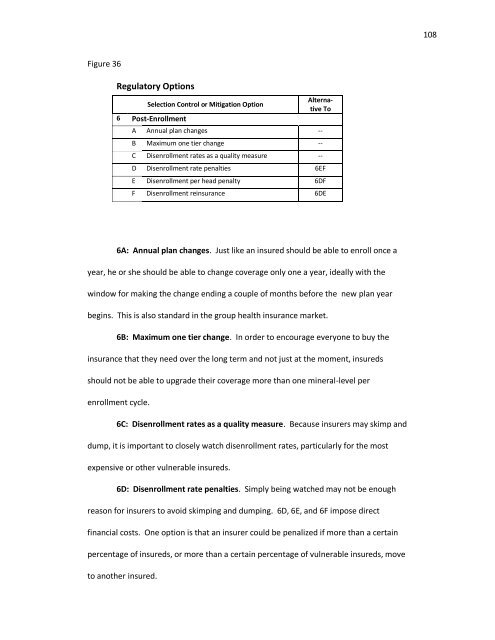
Figure 36<br />
Regulatory Options<br />
<strong>Selection</strong> Control or Mitigation Option<br />
6 Post-Enrollment<br />
Alternative<br />
To<br />
A Annual plan changes --<br />
B Maximum one tier change --<br />
C Disenrollment rates as a quality measure --<br />
D Disenrollment rate penalties 6EF<br />
E Disenrollment per head penalty 6DF<br />
F Disenrollment reinsurance 6DE<br />
6A: Annual plan changes. Just like an insured should be able to enroll once a<br />
year, he or she should be able to change coverage only one a year, ideally with the<br />
window for making the change ending a couple <strong>of</strong> months before the new plan year<br />
begins. This is also standard in the group health insurance market.<br />
6B: Maximum one tier change. In order to encourage everyone to buy the<br />
insurance that they need over the long term and not just at the moment, insureds<br />
should not be able to upgrade their coverage more than one mineral-level per<br />
enrollment cycle.<br />
6C: Disenrollment rates as a quality measure. Because insurers may skimp and<br />
dump, it is important to closely watch disenrollment rates, particularly for the most<br />
expensive or other vulnerable insureds.<br />
6D: Disenrollment rate penalties. Simply being watched may not be enough<br />
reason for insurers to avoid skimping and dumping. 6D, 6E, and 6F impose direct<br />
financial costs. One option is that an insurer could be penalized if more than a certain<br />
percentage <strong>of</strong> insureds, or more than a certain percentage <strong>of</strong> vulnerable insureds, move<br />
to another insured.