

PDF Version - Glidewell Dental Labs
PDF Version - Glidewell Dental Labs
PDF Version - Glidewell Dental Labs

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
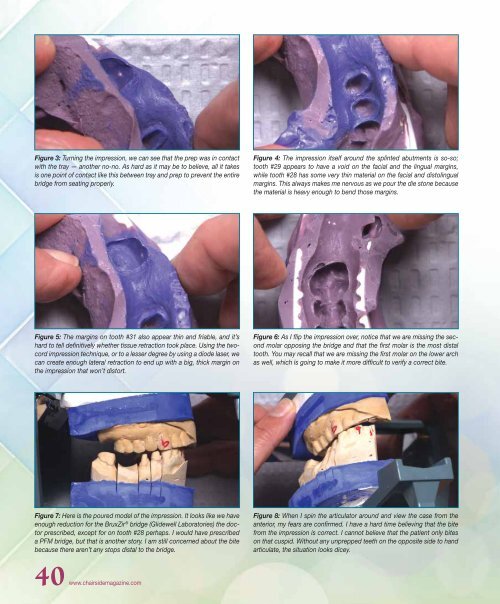
Figure 3: Turning the impression, we can see that the prep was in contact<br />
with the tray — another no-no. As hard as it may be to believe, all it takes<br />
is one point of contact like this between tray and prep to prevent the entire<br />
bridge from seating properly.<br />
Figure 4: The impression itself around the splinted abutments is so-so;<br />
tooth #29 appears to have a void on the facial and the lingual margins,<br />
while tooth #28 has some very thin material on the facial and distolingual<br />
margins. This always makes me nervous as we pour the die stone because<br />
the material is heavy enough to bend those margins.<br />
Figure 5: The margins on tooth #31 also appear thin and friable, and it’s<br />
hard to tell definitively whether tissue retraction took place. Using the twocord<br />
impression technique, or to a lesser degree by using a diode laser, we<br />
can create enough lateral retraction to end up with a big, thick margin on<br />
the impression that won’t distort.<br />
Figure 6: As I flip the impression over, notice that we are missing the second<br />
molar opposing the bridge and that the first molar is the most distal<br />
tooth. You may recall that we are missing the first molar on the lower arch<br />
as well, which is going to make it more difficult to verify a correct bite.<br />
Figure 7: Here is the poured model of the impression. It looks like we have<br />
enough reduction for the BruxZir ® bridge (<strong>Glidewell</strong> Laboratories) the doctor<br />
prescribed, except for on tooth #28 perhaps. I would have prescribed<br />
a PFM bridge, but that is another story. I am still concerned about the bite<br />
because there aren’t any stops distal to the bridge.<br />
Figure 8: When I spin the articulator around and view the case from the<br />
anterior, my fears are confirmed. I have a hard time believing that the bite<br />
from the impression is correct. I cannot believe that the patient only bites<br />
on that cuspid. Without any unprepped teeth on the opposite side to hand<br />
articulate, the situation looks dicey.<br />
40 www.chairsidemagazine.com













