PIP Joint Arthroplasty Revision Using - Small Bone Innovations
PIP Joint Arthroplasty Revision Using - Small Bone Innovations
PIP Joint Arthroplasty Revision Using - Small Bone Innovations

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
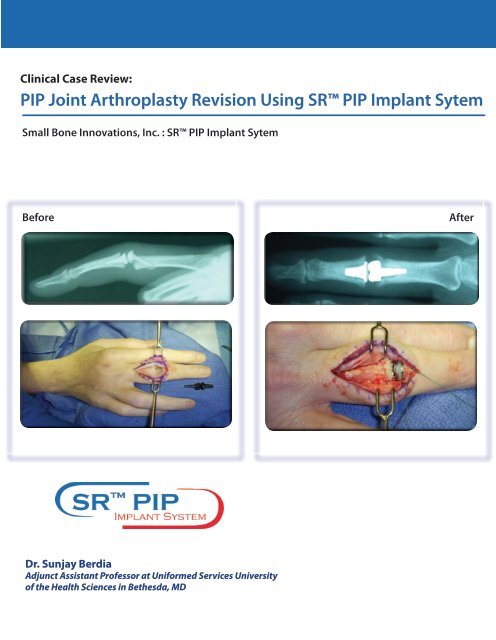
Clinical Case Review:<br />
<strong>PIP</strong> <strong>Joint</strong> <strong>Arthroplasty</strong> <strong>Revision</strong> <strong>Using</strong> SR <strong>PIP</strong> Implant Sytem<br />
<strong>Small</strong> <strong>Bone</strong> <strong>Innovations</strong>, Inc. : SR <strong>PIP</strong> Implant Sytem<br />
Before<br />
After<br />
Dr. Sunjay Berdia<br />
Adjunct Assistant Professor at Uniformed Services University<br />
of the Health Sciences in Bethesda, MD
Patient History<br />
Patient is a 53 year old, right-hand dominant female who sustained<br />
a distal radius fracture. She underwent open reduction<br />
internal fixation of this fracture but she subsequently developed<br />
severe complex regional pain syndrome in that extremity.<br />
Although with time her wrist and digital range of motion improved,<br />
she developed progressive degenerative arthritis in<br />
her middle finger <strong>PIP</strong> and DIP <strong>Joint</strong>s. Her <strong>PIP</strong> joint became increasely<br />
more painful with a concomitant loss of motion. She<br />
was initially treated conservatively with therapy, NSAIDS, and<br />
then finally with cortisone injections.<br />
Preoperative Write Up and X-Rays<br />
Fig. 1: <strong>PIP</strong> <strong>Joint</strong> AP Xray<br />
Fig. 2: <strong>PIP</strong> <strong>Joint</strong> Lateral Xray<br />
Physical examination revealed a <strong>PIP</strong> range of motion from<br />
5 degrees of full extension to 65 degrees of flexion. The <strong>PIP</strong><br />
<strong>Joint</strong> was ulnar deviated 10 degrees. Figures 1 and 2 show<br />
the posteroanterior and lateral radiographs. As she had failed<br />
conservative treatment, the decision was made to proceed<br />
with a joint replacement using the Pyrocarbon <strong>PIP</strong> <strong>Joint</strong> Replacement.<br />
A dorsal tendon splitting approach was used to carry<br />
out the joint replacement. Figures 3 and 4 show postoperative<br />
posteroanterior and lateral radiographs. By appropriate cuts<br />
and tightening of the radial collateral ligament, the ulnar deviation<br />
deformity was corrected. Although the proximal component<br />
seems slightly proud, the stem was tightly fixed into<br />
the canal.<br />
The patient did well in the immediate postoperative period.<br />
Her pain was alleviated. Her range of motion at 3 months was<br />
from 10 degrees of full extension to 75 degrees of flexion. At<br />
5 months, she started to exhibit signs of radiograph loosening<br />
(See Fig. 5 - 6). Therapy on the finger was halted and she was<br />
instructed to rest the finger as much as possible.<br />
Fig. 3: Postoperative AP Xray<br />
Fig. 4: Postoperative Lateral Xray<br />
She was followed using serial radiographs. Even with these<br />
precautions, she showed continued “windshield wiper” loosening<br />
on these radiographs. At 12 months post-operative, (See<br />
Fig. 7 - 8), the decision was then made to revise the arthroplasty<br />
before imminent catastrophic implant failure. Preoperative<br />
physical examination revealed a <strong>PIP</strong> range of motion from 15<br />
degrees of full extension to 55 degrees of flexion. Options<br />
that were then contemplated included using a silicone replacement<br />
or a cemented <strong>PIP</strong> Surface Replacement <strong>Arthroplasty</strong><br />
(SRA) from SBi. Preference was given to the SBi SR <strong>PIP</strong> because<br />
of the potential increase in range of motion, lack of silicone<br />
synovitis, lack of silicone implant breakage, and patient age<br />
and activity level.<br />
SBi SR <strong>PIP</strong> <strong>Arthroplasty</strong> was performed on November 13,<br />
2008.<br />
Fig. 5: <strong>PIP</strong> <strong>Joint</strong> Loosening AP Xray<br />
Fig. 6: <strong>PIP</strong> <strong>Joint</strong> Loosening Lateral Xray<br />
Fig. 7: Windshield Wiper AP Xray<br />
Fig. 8: Windshield Wiper Lateral Xray
Operative Technique<br />
A dorsal tendon splitting approach was again utilized. In order to<br />
gain adequate exposure, the central slip insertion was elevated periosteally<br />
for later repair. The pyrocarbon implant was easy removed<br />
as both components were loose (See Fig. 9).<br />
As the collaterals were in good condition and tension, the decision<br />
was made to proceed using the SRA implant. As the pyrocarbon<br />
is larger than the SRA implant, no additional resurfacing cuts were<br />
necessary. Broaching was attempted but due to loosening within<br />
the canal no broaching was necessary. Any pseudocapsule within<br />
the canal was cleaned with a fine curette so as to promote good<br />
interdigitization at cement-bone interface.<br />
Fig. 9: Intraoperative Photo: Pyrocarbon<br />
Removal<br />
Fig. 10: Intraoperative Photo: Repairing<br />
the Central Slip<br />
Trials were placed temporarily within the canal. An implant size 2 was<br />
chosen based on the best fit to the exposed parts of the proximal and<br />
distal phalangeal metaphysis. The length of the SRA proximal component<br />
stem is longer than the implant. As such, the stem would be<br />
able to go past the “windshield wiper” changes and minimize any stress<br />
risers. Additional steps were taken to repair the central slip. Prior to cementing,<br />
two holes were created at the insertion of the central slip and<br />
a non-absorbable suture was passed through the holes (See Fig. 10).<br />
Fig. 11: Intraoperative Photo: Cementing<br />
Both components were cemented in place at the same time so that the<br />
appropriate length could be determined (See Fig. 11). Prior to cement<br />
hardening, a partial cement mantle was built manually on the proximal<br />
side because of the bone deficiency (See Fig. 12).<br />
Intra-operative radiographs were taken repeatedly including after final<br />
implantation and they confirmed no cement extravasation, especially<br />
on the volar aspect of the proximal phalanx at the level of the<br />
“windshield wiper” changes. Postoperative radiographs seen in Fig. 13<br />
and 14 show a well seated and positioned implant.<br />
Surgery time was 60 minutes.<br />
Fig. 12: Intraoperative Photo: Cement Mantle<br />
Fig. 13: Postoperative AP<br />
SR <strong>PIP</strong> Xray<br />
Fig. 14: Postoperative Lateral<br />
SR <strong>PIP</strong> Xray
Post-Operative Protocol<br />
Patient started 4 days postop with a dynamic splinting protocol during the day and a resting splint at night-time. The dynamic<br />
splinting protocol protects the central slip repair. The patient was extremely pleased with the results and was allowed to return to<br />
full activities after 6 weeks. At 3 months, her range of motion was 0 to 65 degrees of flexion. She continued with the therapy. At<br />
6 months follow-up (See Fig. 15 - 16) her range of motion is 10 degrees of full extension to 75 degrees of full flexion. There was no<br />
clinical evidence of instability, loosening or subsidence.<br />
In this case, the SR <strong>PIP</strong> implant has resolved the <strong>PIP</strong> joint pain, increased ROM, and provided a stable joint.<br />
Fig. 15: Postoperative AP SR <strong>PIP</strong> Xray: 6 Months<br />
Fig. 16: Postoperative Lateral SR <strong>PIP</strong> Xray: 6 Months<br />
<strong>Small</strong> <strong>Bone</strong> <strong>Innovations</strong>, Inc.<br />
1380 South Pennsylvania Ave.<br />
Morrisville, PA<br />
(215) 428-1791/ Fax (215) 428-1795<br />
SBi Customer Service: (800) 778-8837<br />
Technical Support: (866) SBi-TIPS<br />
www.totalsmallbone.com<br />
<strong>Small</strong> <strong>Bone</strong> <strong>Innovations</strong> International<br />
ZA Les Bruyères - BP 28<br />
01960 Péronnas, France<br />
Tel: +33 (0) 474 21 58 19<br />
Fax: +33 (0) 474 21 43 12<br />
Caution: United States federal law restricts this device to sale by or on the order of a physician.<br />
SR <strong>PIP</strong> is a Humanitarian Use Only Device.<br />
Copyright© 2009 <strong>Small</strong> <strong>Bone</strong> <strong>Innovations</strong>, Inc. All rights reserved.<br />
MKT 10870 Rev. A 8/09