LEICESTER, LEICESTERSHIRE AND RUTLAND PCT CLUSTER ...
LEICESTER, LEICESTERSHIRE AND RUTLAND PCT CLUSTER ...
LEICESTER, LEICESTERSHIRE AND RUTLAND PCT CLUSTER ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Paper 1<br />
LLR <strong>PCT</strong> Cluster Integrated Board meeting<br />
8 September 2011<br />
<strong>LEICESTER</strong>, <strong>LEICESTER</strong>SHIRE <strong>AND</strong> RUTL<strong>AND</strong> <strong>PCT</strong> <strong>CLUSTER</strong><br />
INTEGRATED BOARD MEETING<br />
Front Sheet<br />
Title of the report: Annual report on emergency preparedness 2010/11<br />
Report to:<br />
Section:<br />
LLR <strong>PCT</strong> Integrated Board meeting<br />
Public<br />
Date of the meeting: 8 th September 2011<br />
Report by:<br />
Sponsoring Director:<br />
Presented by:<br />
Andy Kelly, Emergency Planning Co-ordinator<br />
Deb Watson, Director of Public Health and Health<br />
Improvement<br />
Deb Watson, Director of Public Health and Health<br />
Improvement<br />
Report supports the following corporate objective(s) 2011 – 2012:<br />
Handing over a good legacy √ Deliver the six identified transitional<br />
strands of work<br />
Manage Providers’ performance against<br />
updated health goals and identified<br />
health inequalities<br />
Deliver agreed performance targets<br />
against the six identified transformation<br />
work streams<br />
Develop and maintain an energetic<br />
stakeholder engagement programme<br />
throughout the transition<br />
√<br />
EXECUTIVE SUMMARY:<br />
1. The purpose of this paper is to provide the Board with an update on activity in<br />
emergency preparedness during the year 2010 / 11. It will provide assurance that, as<br />
outlined in DH Emergency Planning Guidance 2005 “…Boards receive regular<br />
reports including…a specific statement relating to the emergency preparedness<br />
including reports on exercises, training and testing undertaken by the organisation<br />
and that adequate resources are made available to allow discharge of these<br />
responsibilities.”<br />
2. It also contains details of<br />
Incidents that have occurred in the past twelve months<br />
Planned training and exercising for the coming year, including preparation for<br />
the 2012 Olympics, Paralympics and Torch Relay<br />
Assurance that the Cluster is in a good position to prepare for the new NHS<br />
landscape<br />
1
RECOMMENDATIONS:<br />
Paper 1<br />
LLR <strong>PCT</strong> Cluster Integrated Board meeting<br />
8 September 2011<br />
The Trust Board is requested to:<br />
RECEIVE an update on the work undertaken in the last twelve months<br />
RECEIVE the current progress in this area on the Shared Operating Model for <strong>PCT</strong><br />
Clusters (DH, July 2011),<br />
APPROVE the work schedule for the coming year, and;<br />
APPROVE the outlined revisions to the Major Incident Plan and Business Continuity<br />
Policy<br />
2
Paper 1<br />
LLR <strong>PCT</strong> Cluster Integrated Board meeting<br />
8 September 2011<br />
<strong>LEICESTER</strong>, <strong>LEICESTER</strong>SHIRE <strong>AND</strong> RUTL<strong>AND</strong> <strong>PCT</strong> <strong>CLUSTER</strong><br />
INTEGRATED BOARD MEETING<br />
8 SEPTEMBER 2011<br />
Report on Emergency Preparedness activity 2010/11<br />
Introduction<br />
1. The purpose of this paper is to provide the Board with an update on activity in<br />
emergency preparedness during the year 2010 / 11. It provides assurance<br />
that, as outlined in DH Emergency Planning Guidance 2005 “…Boards receive<br />
regular reports including…a specific statement relating to the emergency<br />
preparedness including reports on exercises, training and testing undertaken<br />
by the organisation and that adequate resources are made available to allow<br />
discharge of these responsibilities.”<br />
Incidents in 2010 / 11<br />
2. During the period covered by this report, there were a number of incidents that<br />
required the organisation to be involved in the response.<br />
3. Operation Pennant – September 2010 was the planned response to the<br />
lawful demonstration in Leicester City by the English Defence League.<br />
Working with the Police and Ambulance Service, the <strong>PCT</strong> supported the<br />
response by the deployment of a doctor close to the scene to deal with any<br />
minor injuries and reduce the impact on the Emergency Department. It was<br />
also involved in the co-ordination of the response to ensure that the impact on<br />
the delivery of health care was reduced as far as possible. As a result of the<br />
plans put in place, there was no impact noted on community services or Out of<br />
Hours primary care, no impact on performance of the Emergency Department<br />
or Ambulance Service. A debrief report was sent to the Department of Health<br />
who commended the health community in the way in which we prepared for<br />
and responded to this event.<br />
4. Seasonal Influenza – December 2010. In December 2010, the LLR area was<br />
the first in the country to notice an increase in the level of respiratory illness in<br />
the population. Working with the Health Protection Agency, the <strong>PCT</strong> coordinated<br />
the response of partners in health and social care to ensure that the<br />
impact was managed as effectively as possible. With clear strategic objectives<br />
the impact was controlled as much as possible. Although the impact in UHL<br />
was significant, prompt actions to increase the availability of antiviral drugs to<br />
GPs and increase influenza vaccinations amongst staff staff and members of<br />
the public more vulnerable to the complications of influenza prevented an<br />
even greater impact in terms of illness and NHS capacity. The seasonal<br />
influenza experience in 2010 highlighted the need for influenza vaccination<br />
amongst staff and amongst those vulnerable to complications from influenza,<br />
such as those suffering from diabetes, respiratory or heart disease.<br />
3
Paper 1<br />
LLR <strong>PCT</strong> Cluster Integrated Board meeting<br />
8 September 2011<br />
5. Loughborough Fire – May 2011. In the early hours of the May Bank Holiday<br />
Monday, a fire at Jayplas in Loughborough sent a heavy plume of smoke<br />
through housing in the north of Loughborough. In collaboration with the Health<br />
Protection Agency, the <strong>PCT</strong> Cluster was involved with the co-ordination of<br />
response to this fire, providing clear and consistent advice to the public and<br />
other responders. Although there was a significant quantity of thick black<br />
smoke coming from the fire, there were no reports of people suffering health<br />
consequences as a result of exposure to the smoke. A debrief process is still<br />
underway to identify lessons to be learned<br />
6. Operation Horizon – August 2011. This was the name of the local police<br />
response to the potential spread of civil disorder from London and other<br />
metropolitan cities. The <strong>PCT</strong> was involved by representing the LLR health<br />
community in the strategic co-ordination of the response from local partners;<br />
the provider organisations were involved in the tactical co-ordination. There<br />
was no impact on NHS services during this period. A multi-agency debrief<br />
process is being managed by the Local Resilience Forum support team<br />
Exercises in 2010 / 11<br />
7. During the period of time covered by this report, the <strong>PCT</strong> Cluster took part in a<br />
number of multi-agency exercises.<br />
8. Exercise Brownfield – May 2010 was an exercise to test the way in which<br />
NHS organisations can work together in managing communications with both<br />
staff and public during an incident. As a result of this exercise agreements<br />
were made about how different organisations would be involved in either<br />
leading or supporting the response to an incident. Effective communications<br />
has been shown many times to be key in how we respond to an incident. The<br />
<strong>PCT</strong> was involved in developing and delivering this exercise, as well as taking<br />
a full part in it.<br />
9. Exercise Earthquake – October 2010 was a live exercise to test the<br />
response to a Chemical Biological Radiological or Nuclear (CBRN) incident. It<br />
involved the decontamination of over 150 volunteers from a simulated release<br />
of radioactive material at Leicester Racecourse. This venue was chosen for its<br />
facilities rather than any suggestion it would be at risk of such an incident. This<br />
tested the processes from decontamination of members of the public through<br />
to onward support in a Local Authority Survivor Reception Centre. The <strong>PCT</strong><br />
Cluster was involved as part of the tactical co-ordination of the incident. A<br />
debrief process has identified where improvements to plans and procedures<br />
will improve the response to such incidents in the future<br />
4
Paper 1<br />
LLR <strong>PCT</strong> Cluster Integrated Board meeting<br />
8 September 2011<br />
10. Exercise Greystoke – July 2011 was a live exercise to test the<br />
response to a mass casualty incident. The exercise involved over 500 people<br />
responding to an incident at Loughborough University. The scenario was<br />
around a fire and explosion at one of the laboratory buildings, and tested the<br />
Ambulance Service response to dealing with large numbers of casualties. UHL<br />
was involved in testing its plans through use of a simulation process (known<br />
as EMERGO) of its management casualties, alongside Nottingham and Derby<br />
Hospitals. A total of seven other hospitals across the region were also<br />
involved in the exercise to test the way in which large numbers of casualties<br />
are distributed to hospitals around the region. The exercise also tested the<br />
strategic co-ordination of the response by the Ambulance Service and NHS<br />
East Midlands. The <strong>PCT</strong> Cluster was involved in the strategic co-ordination of<br />
the response. A debrief process is still underway, and will be used to further<br />
develop and refine plans and procedures.<br />
Plans and testing of plans<br />
11. Prior to the transfer of services from the <strong>PCT</strong> under the Transforming<br />
Community Services programme, the business continuity and other relevant<br />
plans were reviewed and ensured that they were updated to transfer with their<br />
services to their new providers. This ensured that there was no risk to<br />
business continuity during the transfer period and enabled the integration of<br />
these plans with their new host’s arrangements<br />
12. The <strong>PCT</strong> Cluster has also developed a document that outlines the<br />
expectations of commissioners on all providers of NHS funded services with<br />
respect to emergency preparedness. This document details how organisations<br />
are expected to work both individually and collectively in preparation, training<br />
and exercising to ensure a prompt and effective response to incidents.<br />
13. The <strong>PCT</strong> Cluster’s Major Incident Plan has been revised in April 2011. This<br />
has been done to take into account the Cluster arrangements, and the<br />
maintenance of the <strong>PCT</strong> Cluster’s responsibility for strategic leadership of the<br />
local NHS. As the new arrangements across the NHS develop in the coming<br />
months, the plan will be revised further. The full revised plan will be published<br />
on the <strong>PCT</strong> website, as required under the Civil Contingencies Act 2004,<br />
following discussion of this report by the <strong>PCT</strong> Cluster Board.<br />
14. A test of the <strong>PCT</strong> Cluster’s Major Incident Plan is scheduled for early 2012 by<br />
means of a tabletop exercise. Some testing of directorate business continuity<br />
plans have also been scheduled for the <strong>PCT</strong> Cluster directorates.<br />
15. The Corporate Business Continuity Policy has also been revised in August<br />
2011 to take into account changes including the Cluster arrangements. This<br />
will be published on the Website following discussion of this report by the <strong>PCT</strong><br />
Cluster Board.<br />
5
Paper 1<br />
LLR <strong>PCT</strong> Cluster Integrated Board meeting<br />
8 September 2011<br />
16. The plans for setting up of antiviral distribution centres as required in<br />
pandemic influenza have also been exercised. This has involved setting up<br />
the pre-identified centres with the staff that would be expected to run them.<br />
This has taken place in two centres in Leicester City in January and June<br />
2011, and all nine designated centres across LLR will have had such an<br />
exercise by March 2011<br />
Training<br />
17. Training has been provided for <strong>PCT</strong> staff in the management of incidents at a<br />
strategic and tactical level, with a total of 12 staff attending exercises. The<br />
<strong>PCT</strong> Cluster has been involved in the testing of plans of other organisations<br />
with a statutory duty to develop plans, such as those produced under the<br />
Control of Major Accident Hazard (COMAH) Regulations, which could present<br />
a threat to the health of the local population.<br />
18. The <strong>PCT</strong> Cluster has also maintained its support for independent practitioners<br />
in developing business continuity plans, since training sessions in 2009 when<br />
71 of 152 GP practices attended one of three workshops held across LLR. At<br />
present, 135 of 152 GP practices (89%) have business continuity plans, and<br />
all remaining practices have been offered one-to-one support in development<br />
of plans.<br />
19. In September 2010, three business continuity exercises were arranged (in the<br />
City, Syston and Ashby-de-la-Zouch) but in the event, only two practices<br />
registered for the exercises in the City, one for the exercise in Ashby-de-la-<br />
Zouch, and three at Syston. There remains an on-going need to develop<br />
Business Continuity Management within General Practice, including further<br />
exercises to validate plans<br />
Future work programme<br />
20. There are a number of areas of work that are being undertaken in the year<br />
2011/12. These will be based around the requirements to maintain the<br />
capability to respond to an incident, while working through the challenges<br />
posed to this by the changes in structure to the way in which NHS funded<br />
services are commissioned and provided. Working with partners in the Local<br />
Resilience Forum (LRF), this will be driven by the priorities identified in the<br />
Community Risk Register. These priorities include:<br />
<br />
<br />
<br />
<br />
<br />
<br />
Pandemic influenza<br />
Flooding<br />
Incident involving transport of hazardous chemicals<br />
Low temperatures and heavy snow<br />
Heatwave<br />
Loss of telecommunications<br />
6
Paper 1<br />
LLR <strong>PCT</strong> Cluster Integrated Board meeting<br />
8 September 2011<br />
Pandemic influenza remains at the top of this list as the overall risk has not<br />
reduced despite the recent pandemic. For full details of the assessment of<br />
risks in the local area, the Community Risk Register can be found in the<br />
Leicester, Leicestershire & Rutland LRF - Library<br />
21. Upcoming exercises in 2011 / 12 will be focussed around the need to prepare<br />
for the Olympics. The planned schedule for the exercise programme is<br />
summarised below:<br />
Date<br />
Exercise<br />
Oct 2011 Loughborough Evacuation, Phase 1<br />
Nov 2011<br />
East Midlands Airport Exercise<br />
Jan 2012<br />
Mass Casualties / Fatalities<br />
Feb 2012<br />
Rest Centre Exercise<br />
Mar 2012<br />
Leicester City Evacuation<br />
April 2012 Loughborough Evacuation, Phase 2<br />
May 2012<br />
Torch Relay Event<br />
June 2012<br />
Leicester City Evening Event<br />
22. The <strong>PCT</strong> Cluster will be involved in the planning of these exercises and will be<br />
responsible for overseeing the involvement of Providers in these exercises.<br />
23. In addition, the <strong>PCT</strong> Cluster will be organising and delivering an exercise for<br />
all major providers of NHS funded care in LLR to test their Major Incident<br />
Plans. This will also test the <strong>PCT</strong> as co-ordinators of the response across LLR<br />
24. The <strong>PCT</strong> Cluster retains a resource to ensure that it has the capability to<br />
respond to incidents with no or short notice through the <strong>PCT</strong> Cluster Director<br />
on call rota, supported by the Emergency Planning Co-ordinator. The pack of<br />
information provided to the on call Director has been revised in August 2011,<br />
and further specific training has been agreed.<br />
25. Over the coming year, the <strong>PCT</strong> Cluster will also continue to work on<br />
developing and testing their business continuity plans, as well as the<br />
development and testing of the plans of independent contractors. We will also<br />
be involved in the testing and exercising of plans, both internally and with<br />
partners, in preparation for the London 2012 Olympics. The British Olympic<br />
Team will be based in Loughborough prior to the games themselves, which<br />
will impact upon the local area.<br />
Future structures<br />
26. This section summarises the requirements for Emergency Planning,<br />
Response and Resilience in the Shared Operating Model for <strong>PCT</strong> Clusters<br />
published by DH in July 2011, and the <strong>PCT</strong> Cluster’s progress against these<br />
responsibilities<br />
7
National context<br />
Paper 1<br />
LLR <strong>PCT</strong> Cluster Integrated Board meeting<br />
8 September 2011<br />
27. The new proposed model will establish a robust and resourced structure which<br />
operates at all NHS levels, providing the Secretary of State with a direct ‘line<br />
of sight’ to local providers of NHS funded care. This will allow the NHS CB to<br />
consistently lead the NHS response to any emergency or incident that has the<br />
potential to, or impacts on, the delivery of NHS services or requires the<br />
services/assets of the NHS to be mobilised at the most appropriate level<br />
Local requirements<br />
28. <strong>PCT</strong> Clusters are expected to maintain the capacity of NHS Commissioners to<br />
carry out Emergency Preparedness, Response and Resilience (EPRR) during<br />
the transition period. They are also expected to support the development of<br />
the new Emergency Planning and Resilience function within the NHS. In the<br />
transition to the new structures, clusters are expected to:<br />
<br />
<br />
Maintain a health emergency planning network, ensuring all NHS<br />
organisations in their area meet at least quarterly to agree health resilience<br />
issues<br />
Appoint/nominate a director who is responsible for health emergency<br />
planning; this person should:<br />
o Chair the Health Emergency Planning Network<br />
o Report to the board regularly on local risks to either delivering<br />
health care, and/or the health of the local population<br />
o Be responsible for representing the local health economy at the<br />
Local Resilience Forum Executive<br />
<br />
Provide a 24/7 arrangement to provide strategic leadership to the local<br />
NHS in the event of a major incident. This should be able to:<br />
o Operate via a suitably equipped control room for period of up to<br />
two weeks<br />
o Have clearly delegated authority to mobilise and direct the<br />
resources of any NHS organisations across LLR during an<br />
incident across the local health economy<br />
<br />
Maintain a sufficiently resourced and adequately trained health emergency<br />
planning team that can manage the day-to-day preparedness work, and<br />
support the Director and Cluster <strong>PCT</strong> board. This will include:<br />
o Promote, develop and facilitate relationships between NHS<br />
funded providers and other partners, including local authorities<br />
with regards to emergency preparedness and response<br />
8
Future arrangements<br />
Paper 1<br />
LLR <strong>PCT</strong> Cluster Integrated Board meeting<br />
8 September 2011<br />
o Ensure sufficient testing and exercising of communication plans<br />
in accordance with the 2005 DH guidance. This should include<br />
testing both in hours and out of hours<br />
o Ensure the local NHS contributes fully to any local multi-agency<br />
training and exercising programme<br />
o Ensure mechanisms are in place to support local system wide<br />
response, including cross boundary mutual aid for emergency<br />
response<br />
29. It is emerging that these requirements will in future be those of the “field force”<br />
of the NHS CB. The NHS CB will in future set a risk-based national<br />
Emergency Preparedness, Response and Resilience (EPRR) implementation<br />
strategy and planning structure for the NHS. It will also put in place a<br />
consistent national EPRR assurance framework for all providers of NHS<br />
funded care. At the sub-national level, it is proposed that NHS CB will<br />
commission, direct and assure the local EPRR structure to ensure delivery of<br />
the national EPRR strategy. At the local level, it is proposed that the NHS CB<br />
will discharge its EPRR function via 39 Local Health Resilience Boards<br />
(LHRB) which will map onto existing Local Resilience Forum boundaries. The<br />
sub-national hubs of the NHS CB will be responsible for appointing a suitable<br />
local NHS CB lead who will chair the LHRB. Supported by a NHS CB funded<br />
team, this lead will have responsibility for local planning, assurance and<br />
response.<br />
Current position in LLR<br />
30. Most of the major areas detailed in the local requirements are already in place<br />
in LLR. We have a mutual aid agreement that provides the background to our<br />
ability to support organisations involved in the response to incidents. We also<br />
have a memorandum of understanding that details the executive support for<br />
the “NHS Gold” role that would provide the strategic leadership required.<br />
Although we currently have two potential control rooms (which are currently<br />
being reviewed) this will need to be reviewed again in light of any estates<br />
changes in coming months.<br />
31. In order to make sure that emergency preparedness is maintained in the<br />
future, the Health Emergency Planning Group has been reconstituted to reflect<br />
the new and emerging landscape of the NHS. Membership includes those<br />
providers from outside of LLR who now provide core services within the<br />
boundaries including the George Eliot Hospital NHS Trust (Urgent Care<br />
Centre) and Central Nottinghamshire Clinical Services (GP Out of Hours<br />
service).This now meets as the LLR Health Emergency Preparedness and<br />
9
Paper 1<br />
LLR <strong>PCT</strong> Cluster Integrated Board meeting<br />
8 September 2011<br />
Response Group, which is a standing sub-group of the Local Resilience<br />
Forum. Its terms of reference are available on request.<br />
32. At present, the Chief Executive represents the Cluster on the LRF, with a lead<br />
DPH in Emergency Preparedness identified. With Directors of Public Health<br />
expected to move to Local Authorities by April 2013, the lead Director<br />
arrangements for NHS emergency preparedness, resilience and response will<br />
require review prior to April 2013. This is to ensure that a suitable NHS<br />
Director is designated to lead NHS resilience and response.<br />
33. During August and September 2011, the Department of Health is holding a<br />
series of national workshops to “road test” an outline model for future NHS<br />
Emergency Preparedness, Response and Resilience after April 2013. The<br />
Department of Health is expected to issue further guidance following these<br />
workshops<br />
Recommendations<br />
The Board is asked to:<br />
RECEIVE an update on the work undertaken in the last twelve months<br />
RECEIVE the current progress in this area on the Shared Operating Model for <strong>PCT</strong><br />
Clusters (DH, July 2011),<br />
APPROVE the work schedule for the coming year, and;<br />
APPROVE the outlined revisions to the Major Incident Plan and Business Continuity<br />
Policy<br />
10
Paper 2<br />
LLR <strong>PCT</strong> Cluster Integrated Board Meeting<br />
8 September 2011<br />
<strong>LEICESTER</strong>, <strong>LEICESTER</strong>SHIRE <strong>AND</strong> RUTL<strong>AND</strong> <strong>PCT</strong> <strong>CLUSTER</strong><br />
INTEGRATED BOARD MEETING<br />
Front Sheet<br />
Title of the report:<br />
Report to:<br />
Section:<br />
Leicester, Leicestershire & Rutland Winter Resilience<br />
Planning 2011/12<br />
Leicester, Leicestershire and Rutland <strong>PCT</strong> Cluster<br />
Integrated Board Meeting<br />
Public<br />
Date of the meeting: 8 September 2011<br />
Report by:<br />
Sponsoring Director:<br />
Presented by:<br />
Amita Chudasama, Planning & Delivery Manager<br />
Catherine Griffiths, LLR Cluster Chief Executive and Chair<br />
of the LLR Emergency Care Network.<br />
Report supports the following corporate objective(s) 2011 – 2012:<br />
Handing over a good legacy<br />
Deliver the six identified transitional<br />
strands of work<br />
Manage Providers’ performance against Develop and maintain an energetic<br />
updated health goals and identified<br />
stakeholder engagement programme<br />
health inequalities<br />
throughout the transition<br />
Deliver agreed performance targets x<br />
against the six identified transformation<br />
work streams<br />
EXECUTIVE SUMMARY:<br />
Update on the arrangements put in place by the Leicester Leicestershire and Rutland<br />
health and social care community to maintain access to services throughout Winter<br />
11/12 including, the Christmas and New year holiday period.<br />
RECOMMENDATIONS:<br />
The Trust Board are requested to:<br />
Note and Approve the Winter Resilience Plans for the LLR health and social care<br />
economy.<br />
1
Paper 2<br />
LLR <strong>PCT</strong> Cluster Integrated Board Meeting<br />
8 September 2011<br />
<strong>LEICESTER</strong>, <strong>LEICESTER</strong>SHIRE <strong>AND</strong> RUTL<strong>AND</strong> <strong>PCT</strong> <strong>CLUSTER</strong><br />
INTEGRATED BOARD MEETING<br />
7 September 2011<br />
Leicester, Leicestershire & Rutland Winter Resilience Planning 2011/12<br />
INTRODUCTION<br />
Context<br />
1. Winter impacts upon the full spectrum of health and social care services with<br />
extra demands on services during winter on all parts of the NHS including<br />
primary care, ambulance and acute hospital services, particularly the<br />
Emergency Department, critical care and medical inpatient beds, as well as on<br />
partners such as social care.<br />
Leicester, Leicestershire & Rutland Winter Resilience Plan 2011/12<br />
2. A co-ordinated, multi-agency approach is essential to ensure that preparation is<br />
robust and that processes are in place that can adapt to the different pressures<br />
as and when they arise. The LLR winter resilience plan has been coordinated<br />
through the LLR Winter Resilience Group, co chaired by the <strong>PCT</strong> Cluster and<br />
UHL. This multi agency group includes representation from all organisations<br />
across LLR involved in the delivery of urgent and emergency care, either in<br />
person or ‘virtually’ and has the full support of the local health and social care<br />
economy and is a sub-group of the LLR Emergency Care Network.<br />
3. The aim of the plan is to:<br />
Support the health and social care community to respond to periods of high<br />
and unusual demand by ensuring that service flexibility and capacity is at<br />
optimal levels as winter approaches.<br />
Provide assurance of business continuity between providers and<br />
commissioners.<br />
Prompt service responsiveness to increase during the winter months<br />
especially in relation to flexibility and capacity.<br />
Clarify escalation triggers, ensuring an integrated and shared process<br />
between primary and secondary care providers and partner agencies such as<br />
social care.<br />
Describe agreed communication and reporting channels to enable appropriate<br />
responses to be made in the event of escalation due to additional winter<br />
activity.<br />
2
Paper 2<br />
LLR <strong>PCT</strong> Cluster Integrated Board Meeting<br />
8 September 2011<br />
4. The LLR <strong>PCT</strong> cluster has led the formulation of the winter plan with partner<br />
agencies to harmonise procedures across the City and County, including each<br />
Urgent Care lead GP from each of the 3 Clinical Commissioning Group’s. The<br />
plan has also evolved following feedback from the national IMAS team and<br />
lessons learned from winter 10/11. It also aligns with the plans for pandemic<br />
flu.<br />
5. The winter plan is designed to form part of the long-term local strategy and the<br />
commissioning of responsive services that meet patient need. Although every<br />
effort has been made to prepare for winter, it is recognised that from time to time<br />
all care providers are likely to be functioning under extreme pressure and that<br />
there will be an increase in demand for health and social care services during this<br />
period.<br />
6. Overall, the winter planning process has followed a route of logical, informed<br />
planning and preparation, good practice and collaboration, and contingency<br />
planning to deal with problems as they arise.<br />
7. The Winter Plan and the Escalation Plan are attached. All other appendices are<br />
in the process of being finalised in collaboration with stakeholders and are<br />
available if required.<br />
RECOMMENDATIONS<br />
The Trust Boards are requested to:<br />
Note & Approve the Winter Resilience Plan for the LLR health and social care<br />
economy.<br />
3
<strong>LEICESTER</strong>, <strong>LEICESTER</strong>SHIRE <strong>AND</strong> RUTL<strong>AND</strong> HEALTH <strong>AND</strong> SOCIAL CARE COMMUNITY<br />
Emergency Escalation Plan<br />
August 2011<br />
1
Index<br />
Page<br />
Background 3<br />
Introduction 4<br />
Role of the Leicester, Leicestershire and Rutland <strong>PCT</strong> Cluster 4<br />
UHL Bed Management Policy 5<br />
Leicester, Leicestershire & Rutland Whole System Escalation Plan 2011/12 7<br />
Escalation and De-Escalation Process 17<br />
Contacts 18<br />
2
BACKGROUND<br />
This plan has been developed in conjunction with representatives from the following organisations:-<br />
Leicester, Leicestershire and Rutland Cluster<br />
University Hospitals of Leicester NHS Trust<br />
Leicestershire Partnership Trust (incorporating City and County Community Health Services)<br />
East Midlands Ambulance Service NHS Trust<br />
West Leicestershire Consortium<br />
Crescent Consortium<br />
One Leicester Consortium<br />
Leicester City Social Services<br />
Leicestershire County Social Services<br />
Central Notts Clinical Services for Out of Hours Service<br />
George Eliot NHS Trust for Urgent Care Centre<br />
The Leicester, Leicestershire and Rutland Emergency Care Network have reviewed this escalation plan and will review at regularly determined<br />
intervals.<br />
3
INTRODUCTION<br />
EMERGENCY ESCALATION PLAN<br />
The Leicester, Leicestershire and Rutland Health and Social Care Community escalation plan includes separate escalation plans for the different<br />
partner agencies and areas of the Health and Social Care Community. The alert status declared by the University Hospitals of Leicester NHS Trust<br />
(UHL) determines the overall Leicestershire health and social care community alert status.<br />
Whilst detailed planning has taken place to profile expected activity against capacity, there are instances when any of the health or social care<br />
partners may have difficulty in providing their normal services. The escalation plan identifies actions that will be taken by each area and / or as a<br />
whole community to meet the demands being put on the service. The expectation is that each area will take all necessary management action to<br />
resolve local difficulties and pressures. However, it is recognised that despite all interventions there will be occasions when pressures cannot be<br />
easily contained by one organisation.<br />
The plan is designed to maintain a safe and good quality service for patients at all times and is not designed to shift the pressure from one area to<br />
another but to share the burden in order to achieve balance across the Health and Social Care Community.<br />
There are several levels of alert status for the escalation plan:<br />
Normal Working<br />
Level 1<br />
Early signs of difficulty/some excess pressure requiring some extra management intervention<br />
Level 2<br />
Persistent excess pressure requiring significant additional management action<br />
Level 3<br />
Level 4<br />
Severe and/or prolonged excess pressure requiring support for all agencies<br />
Extreme pressure requiring immediate and significant action<br />
ROLE OF THE <strong>LEICESTER</strong>, <strong>LEICESTER</strong>SHIRE <strong>AND</strong> RUTL<strong>AND</strong> <strong>PCT</strong> <strong>CLUSTER</strong><br />
The LLR <strong>PCT</strong> Cluster will act as the “communication cell” for the escalation plan. The different organisations will communicate their pressure<br />
problems and status of alert to the Urgent Care Lead, Rachna Vyas 0116 295 4179 so that the overall picture in the Health and Social Care<br />
Community is known at any one time.<br />
Each organisation will be responsible for developing their own organisational mechanisms to communicate any pressures. For example UHL Bed<br />
Bureau will act as UHL’s internal “communication cell” for escalation. The different areas will communicate their pressure problems and status of<br />
alert to the Bed Manager via the Bed Bureau so that the overall picture is known at any one time.<br />
4
The LLR <strong>PCT</strong> Cluster’s role will also be:<br />
• To lead the strategic development of emergency services for the local health and social care community.<br />
• To be the single point of contact for the Strategic Health Authority (SHA) for emergency services in relation to SITREPs and escalation planning<br />
with the exception being if a serious untoward incident occurs when the relevant Trust should notify the SHA directly as well as the LLR Cluster.<br />
• To be made aware by the Emergency Care Lead (ECL) of the organisations of the health and social care community of any issues that could<br />
affect the service delivery of emergency care i.e. bed/ward closures/exceptional demand for services.<br />
• To co-ordinate the SITREP submission for the local health and social care community liaising with each Trust who has data to submit against<br />
the SITREP timetable.<br />
• To oversee the delivery of the Escalation Plan, being informed by any organisation who wished to declare a 'major incident' of the situation and<br />
being part of the senior officer discussions prior to the formal declaration of the alert status. The organisation wishing to declare the alert would<br />
co-ordinate the meeting.<br />
• To chair the Daily Escalation Conference Calls and oversee any actions resulting from the calls.<br />
UHL BED MANAGEMENT POLICY<br />
The Major Incident Policy and the Bed Management Policy for University Hospitals of Leicester NHS Trust (UHL) interfaces with the escalation<br />
policy as the impact of the major incident may be to compromise capacity within UHL. It will therefore require co-operation from all agencies within<br />
the health and social care community to manage the situation as well as the ongoing health and social care needs of the population. The Level 4<br />
status may be exceeded if the situation continues to escalate or a major incident occurs but especially if a situation results in mass casualties, i.e.<br />
over 100, when the emergency plans in place for these situations will be implemented.<br />
If it is apparent that the Red alert status is not going to be stepped-down, then a meeting of the Directors/ Senior Officers from the partner agencies<br />
will be called by the organisation who is asking for the alert status to be escalated to ‘Black. This meeting, chaired by the organisation wishing to call<br />
a major incident, will make the decision whether the Health and Social Care Community should declare this. The actions to be taken will be agreed<br />
by the Senior Officers group which includes LLR <strong>PCT</strong> Cluster who is the strategic lead for emergency services. This group will also ratify the<br />
decision to downgrade the alert status.<br />
5
The University Hospitals of Leicester NHS Trust’s Bed Management Policy, details actions that UHL will take to manage the emergency admission<br />
process, bed capacity and the associated hospital status for internal escalation. The Bed Management Policy is Appendix 2 to the 2011/12 Winter<br />
Resilience Plan.<br />
Each day following assessments of overall bed capacity, the Admissions and Discharge Manager will determine the level of bed alert within UHL in<br />
hours Monday – Friday 8am – 5pm, out of hours this is the responsibility of the duty manager in discussion with the senior manager on call.<br />
The Trust’s aim is to start each day on a Normal Status and escalate where appropriate i.e. after discussions of bed capacity at the 8.30 bed<br />
meeting. The decision will be based on the predicted shortfall in capacity.<br />
The status of UHL beds is divided into the categories below and a “Bed Alert” is declared against this criteria<br />
Normal Status<br />
<br />
<br />
No problems identified<br />
Normal day to operation plan of bed management<br />
Stage One<br />
Bed Alert<br />
<br />
<br />
The rate of emergency admissions is exceeding the rate and which beds will become available.<br />
Elective Admissions are still prioritised – NOT Cancelled<br />
Stage Two<br />
Bed Alert<br />
<br />
<br />
<br />
<br />
The rate of emergency admissions has exceeded the number of beds available.<br />
Elective category B&C cases for non ring fenced beds reviewed for cancellation.<br />
Extra capacity to be created<br />
Outlying of patients to alternative Business Units/Divisions.<br />
Stage Three<br />
Bed Alert<br />
<br />
<br />
<br />
<br />
<br />
Situations deteriorating.<br />
Major shortfall in the number of beds available for emergency admissions.<br />
All available extra capacity to be created<br />
Outlying of patients to alternative Business Units/Divisions.<br />
Review of all electives cases for cancellation<br />
6
Leicester, Leicestershire & Rutland Whole System Escalation Plan 2011/12<br />
NORMAL WORKING<br />
System Triggers<br />
INDIVIDUAL ORGANISATION TRIGGERS<br />
URGENT CARE CENTRE/ MIU’S/ WIC<br />
EMAS<br />
UHL<br />
SOCIAL CARE<br />
• Urgent Care Centre, WIC’s & MIU’s<br />
working normally<br />
• No excess pressure on Emergency & PTS<br />
transport<br />
• No 30 minutes or more turnaround time<br />
• No ambulance diverts<br />
• Sickness Absence
NORMAL WORKING<br />
System Triggers<br />
LPT – COMMUNITY HEALTH SERVICES<br />
• No delays within Community Hospitals/<br />
IC Teams<br />
• In Hours Services working normally<br />
LPT – MENTAL HEALTH SERVICES<br />
INDIVIDUAL ORGANISATION TRIGGERS<br />
PRIMARY CARE<br />
• Currently status is ‘normal for season<br />
• Preparatory work is underway<br />
• Available appointments at GPs<br />
• Reviewing plans for business continuity<br />
• normal operation<br />
OUT OF HOURS<br />
• Out of Hours Services working normally<br />
System Actions<br />
• Daily teleconference at 11.45am involving urgent care leads from each organisation with Objective of identifying issues early on to avoid disruption to patient flow across LLR.<br />
• Community hospital bed state to be faxed/emailed daily to UHL Bed Bureau by 9am/2pm<br />
LPT – COMMUNITY HEALTH SERVICES<br />
LPT – MENTAL HEALTH SERVICES<br />
INDIVIDUAL ORGANISATION ACTIONS<br />
PRIMARY CARE<br />
OUT OF HOURS<br />
<br />
Daily monitoring of demand across<br />
services<br />
<br />
Daily monitoring of demand across<br />
services<br />
<br />
Daily monitoring of demand across<br />
services<br />
<br />
Daily monitoring of demand across<br />
services<br />
8
ESCALATION LEVEL 1 – EARLY SIGNS OF DIFFICULTY/SOME EXCESS PRESSURE REQUIRING SOME EXTRA MANAGEMENT<br />
INTERVENTION<br />
System Triggers @ Midday<br />
No. of patients in ED 40 -50 Time to see Senior Decision Maker > 1.5 hours ED breaches 4-6 Cancellation of elective admissions for capacity related issues Critical Care Capacity = 0 Admissions unit<br />
capacity/bed capacity – 100-110 More than 6 patients awaiting Community beds (excluding those waiting for choice reasons EMAS REAP Level 1 Ambulance turnaround times >15 mins<br />
INDIVIDUAL ORGANISATION TRIGGERS<br />
URGENT CARE CENTRE/ MIU’S/ WIC<br />
EMAS<br />
UHL<br />
SOCIAL CARE<br />
• Urgent Care Centre /WIC waiting times<br />
consistently 3 hours<br />
As above and<br />
• Jobs awaiting vehicle allocation does not<br />
exceed<br />
• 70 EMAS wide or<br />
• > 35- 40 for one control desk<br />
• >30 ‘on day’ transport request for<br />
PTS<br />
As above and<br />
• Planned discharges not sufficient to<br />
accommodate admissions from the<br />
admissions units and ED<br />
• The rate of emergency admissions is<br />
exceeding the rate at which beds will become<br />
available.<br />
• Increase in volume of referrals from wards to<br />
both Acute Trust Social Work Teams and<br />
Area Teams.<br />
System Actions<br />
• Service provider should in the first instance inform the contacts above, dependant on whether in or out of hours and agree the escalation level required. This should be confirmed at the next daily<br />
teleconference.<br />
• <strong>PCT</strong> leads will send out alert to the Emergency Care Network regarding service pressures. Each member of the ECN to implement actions listed below to help increase the flow of patients across the<br />
system.<br />
• Implement flu pandemic plan should a pandemic alert be called & FLU DIRECTORS NOTIFIED<br />
• Patient & public targeted communications strategy enacted across LLR<br />
INDIVIDUAL ORGANISATION ACTIONS<br />
URGENT CARE CENTRE/ MIU’S/ WIC<br />
EMAS<br />
UHL<br />
SOCIAL CARE<br />
• Urgent care Centre/WIC’s to review staffing<br />
and place off-duty on standby<br />
• Duty Control Manager to contact A&E Duty<br />
Control Manager.<br />
• Implement Level 1 Escalation<br />
• Manage pressures with internal escalation<br />
measures.<br />
• Site Duty Manager to confirm with CBU leads<br />
for bed management that all actions outlined<br />
in the daily operational plan have been taken.<br />
• If appropriate actions have not been taken the<br />
Clinical Business Manager will be informed<br />
• Review the potential shortfall in the number of<br />
beds and confirm that all capacity has been<br />
utilized before determining the alert status<br />
• Appropriate staff are made aware of<br />
increasing bed pressures verbally or via email<br />
(consultants on-call /manager on-call / senior<br />
nurses & managers<br />
• Ensure that all low risk actions are in place<br />
consider invoking moderate risk actions<br />
• Communicate Bed Status to Leicestershire<br />
Health Social Care Community<br />
• Implement Level 1 Escalation<br />
• Ensure no delays to transfer of care from<br />
community hospitals.<br />
• Alert A&E worker of possible pressures in<br />
A&E –UHL & LRI<br />
• Alert duty worker for EMU/MAU.<br />
• Implement Level 1 Escalation<br />
9
ESCALATION LEVEL 1 – EARLY SIGNS OF DIFFICULTY/SOME EXCESS PRESSURE REQUIRING SOME EXTRA MANAGEMENT<br />
INTERVENTION<br />
System Triggers @ Midday<br />
No. of patients in ED 40 -50 Time to see Senior Decision Maker > 1.5 hours ED breaches 4-6 Cancellation of elective admissions for capacity related issues Critical Care Capacity = 0 Admissions unit<br />
capacity/bed capacity – 100-110 More than 6 patients awaiting Community beds (excluding those waiting for choice reasons EMAS REAP Level 1 Ambulance turnaround times >15 mins<br />
INDIVIDUAL ORGANISATION TRIGGERS<br />
LPT – COMMUNITY HEALTH SERVICES<br />
LPT – MENTAL HEALTH SERVICES<br />
PRIMARY CARE<br />
OUT OF HOURS<br />
• Reduced bed capacity<br />
• Staff shortages resulting in some reduced<br />
capacity<br />
• Early signs of increased demand on services.<br />
• Some staffing difficulties linked to e.g. flu<br />
outbreak<br />
• Some increase in demand for appointments<br />
• Staff shortages linked to an impending<br />
situation e.g. flu outbreak<br />
• Increased early discharges from secondary<br />
care<br />
• Specified pharmacy closure<br />
• Increased demand during out of hours<br />
System Actions<br />
• Service provider should in the first instance inform the contacts above, dependant on whether in or out of hours and agree the escalation level required. This should be confirmed at the next daily<br />
teleconference.<br />
• <strong>PCT</strong> leads will send out alert to the Emergency Care Delivery Group regarding service pressures. Each member of the ECDG to implement actions listed below to help increase the flow of patients across the<br />
system.<br />
• Implement flu pandemic plan should a pandemic alert be called & FLU DIRECTORS NOTIFIED<br />
• Patient & public targeted communications strategy enacted across LLR<br />
INDIVIDUAL ORGANISATION ACTIONS<br />
LPT – COMMUNITY HEALTH SERVICES<br />
LPT – MENTAL HEALTH SERVICES<br />
PRIMARY CARE<br />
OUT OF HOURS<br />
• On call capacity manager to implement<br />
community capacity plan.<br />
• Situation to be monitored by LPT Senior<br />
Operations Team with appropriate<br />
intervention as necessary.<br />
• Situation to be monitored by LPT Senior<br />
Operations Team with appropriate<br />
intervention as necessary.<br />
• Additional clinics and/or different ways of<br />
working required to meet the demand<br />
• Number of routine appointments reduced<br />
• Enhanced coordination between health and<br />
social care<br />
• <strong>PCT</strong> communications to circulate Bed Bureau<br />
alerts<br />
• Practices to review capacity & demand plan<br />
• If practice specific, notify Consortium/<strong>PCT</strong><br />
• Consider whether activation of the practice<br />
Service Continuity Plan is appropriate<br />
• Alert Single Point of Access (SPA) team<br />
• If practice specific, notify Consortium/<strong>PCT</strong><br />
• Consider whether activation of the practice<br />
Service Continuity Plan is appropriate<br />
• Alert Single Point of Access (SPA) team<br />
• Alert Pharmacy Contractors/LPC of potential<br />
of increased demand for prescribed<br />
medicines, and to avoid possible supply<br />
problems<br />
• Invoke Pharmacy Closure protocol<br />
<br />
<br />
Real time monitoring and escalation<br />
where needed<br />
Daily capacity reviews<br />
10
ESCALATION LEVEL 2 – PERSISTENT EXCESS PRESSURE REQUIRING SIGNIFICANT ADDITIONAL MANAGEMENT ACTION<br />
No. of patients in ED 50 – 60 Time to see Senior Decision Maker > 2hours ED breaches 6-10 Cancellation of elective admissions Critical Care Capacity = 0 Admissions unit capacity/bed capacity – 80-100<br />
More than 10 patients awaiting Community beds EMAS REAP Level 2 Ambulance turnaround times >30 mins WiC/UCC time to see Senior Decision Maker Consistently 3.5 hours<br />
INDIVIDUAL ORGANISATION TRIGGERS<br />
URGENT CARE CENTRE/ MIU’S/ WIC<br />
• As Level 1<br />
EMAS<br />
As above and<br />
• Continuation of factors as stated in Level 1<br />
• Jobs awaiting allocation not decreasing after 2<br />
hours.<br />
• Functional failure of CAD, COMS, Radio in<br />
Control.<br />
• Demand & Capacity plan breached<br />
UHL<br />
As above and<br />
• Early morning elective patients placed but<br />
difficulty in placing later admissions<br />
• The triggers to escalate to an Amber Bed Alert<br />
will take place when there is a predicted<br />
shortfall in capacity across UHL. All of the<br />
actions outlined in the Bed Alert Status will<br />
take place with the addition of those for a<br />
Amber Bed Alert that are given below<br />
SOCIAL CARE<br />
• Increase in volume of referrals from wards to<br />
both Acute Trust social work teams and area<br />
team.<br />
System Actions<br />
• Service provider should in the first instance inform the contacts above, dependant on whether in or out of hours and agree the escalation level required. This should be confirmed at the next daily teleconference.<br />
• <strong>PCT</strong> leads will send out alert to the Emergency Care Network regarding the escalation. Each member of the ECN to implement actions listed below to help increase the flow of patients across the system.<br />
• Implement flu pandemic plan should a pandemic alert be called & FLU DIRECTORS NOTIFIED<br />
• Patient & public targeted communications strategy enacted across LLR<br />
INDIVIDUAL ORGANISATION ACTIONS<br />
URGENT CARE CENTRE/ MIU’S/ WIC<br />
• Diverts and mutual aid between UCC and ED<br />
EMAS<br />
• Implement Level 2 escalation<br />
• Mobilise additional A&E and PTS support to<br />
deal with increased sustained activity<br />
UHL<br />
• Confirm all action on level have been taken<br />
• Wards/departments, CSSD, Imaging and<br />
Pathology are made aware of alert status<br />
verbally or via emailed bed status<br />
• CBU bed management leads informed of the<br />
need to asses for moderate risk actions<br />
• Confirm that all available capacity has been<br />
utilised before escalation declared<br />
• Elective specialities to prepare for possible<br />
cancellation of Category B elective admissions<br />
according to prioritised list - to prepare for<br />
outlying<br />
• CBU(s) Senior Medical / Nursing & mgmt<br />
teams informed of the need to assess for<br />
moderate actions<br />
• (OOH– on-call clinicians, Senior nurses, bleepholders<br />
informed)<br />
• Inform elective specialities to cancel planned<br />
admissions (B & C cases) in order to create<br />
additional capacity<br />
• Communicate Bed Status to LLR Health Social<br />
Care Community<br />
SOCIAL CARE<br />
• As for Level 1<br />
• Implement Level 2 escalation<br />
• Alert all Social Services staff based in Acute<br />
Trust, areas and Out of Hours Team to need to<br />
expedite discharges.<br />
• All Service Users already having received a<br />
full care needs assessment, & awaiting “Home<br />
of Choice” will be asked to move immediately<br />
(with carers/Family consent) where<br />
appropriate<br />
• Need for earlier approval of funding.<br />
• Check staffing levels<br />
• Check capacity in Intermediate Care and LA<br />
short-term care beds.<br />
11
ESCALATION LEVEL 2 – PERSISTENT EXCESS PRESSURE REQUIRING SIGNIFICANT ADDITIONAL MANAGEMENT ACTION<br />
No. of patients in ED 50 – 60 Time to see Senior Decision Maker > 2hours ED breaches 6-10 Cancellation of elective admissions Critical Care Capacity = 0 Admissions unit capacity/bed capacity – 80-<br />
100 More than 10 patients awaiting Community beds EMAS REAP Level 2 Ambulance turnaround times >30 mins WiC/UCC time to see Senior Decision Maker Consistently 3.5 hours<br />
INDIVIDUAL ORGANISATION TRIGGERS<br />
LPT – COMMUNITY HEALTH SERVICES<br />
LPT – MENTAL HEALTH SERVICES<br />
PRIMARY CARE<br />
OUT OF HOURS<br />
• Reduced bed capacity<br />
• Staff shortages resulting in reduced capacity.<br />
• Increased demand on services.<br />
• Staffing difficulties linked to e.g. flu outbreak<br />
• Routine appointments unavailable<br />
• Reduction in non-critical services<br />
• GP/PN clinical triage of patients trying to<br />
access service<br />
• Implementation of admission and discharge<br />
criteria that are different to normal practice<br />
• Practices facing significant demand for<br />
appointment and/or home visits<br />
• Difficulty in accessing secondary care beds<br />
• Consortium/<strong>PCT</strong> Alert issued<br />
• Practice(s) Service Continuity Plan activated<br />
• Alert received from SPA or County Primary<br />
Care Coordinators<br />
<br />
As for level 1 with evidence of breaches<br />
against National Quality Requirement<br />
standards<br />
System Actions<br />
• Service provider should in the first instance inform the contacts above, dependant on whether in or out of hours and agree the escalation level required. This should be confirmed at the next daily teleconference.<br />
• <strong>PCT</strong> leads will send out alert to the Emergency Care Network regarding the escalation. Each member of the ECN to implement actions listed below to help increase the flow of patients across the system.<br />
• Implement flu pandemic plan should a pandemic alert be called & FLU DIRECTORS NOTIFIED<br />
• Patient & public targeted communications strategy enacted across LLR<br />
INDIVIDUAL ORGANISATION ACTIONS<br />
LPT – COMMUNITY HEALTH SERVICES<br />
LPT – MENTAL HEALTH SERVICES<br />
PRIMARY CARE<br />
OUT OF HOUR’S<br />
• Monitoring admissions from UHL<br />
• SPA to provide regular capacity updates<br />
• Early discharge to community supported by<br />
DN teams<br />
• UCC to contact Communication Centre – non<br />
urgent appointment deferred 5 hours (within<br />
QR standard)<br />
• Implement Level 2 Escalation.<br />
• Implement Daily Service Situation Reporting<br />
(Refer to LPT Emergency Plan) across all LPT<br />
services.<br />
• Monitoring of situation by LPT Senior<br />
operations Team.<br />
• Monitoring admissions from UHL.<br />
• Implement Daily Service Situation Reporting<br />
(Refer to LPT Emergency Plan) across all LPT<br />
services.<br />
• Implement Staff Mobilisation Plan, if<br />
necessary, (Refer to LPT Emergency Plan) to<br />
support hot-spots.<br />
• Early discharge to community with appropriate<br />
support if safe to do so.<br />
• Monitoring of situation by LPT Senior<br />
operations Team.<br />
• UHL to provide <strong>PCT</strong> info on high admitting<br />
practices<br />
• <strong>PCT</strong> to follow up with individual practices<br />
• <strong>PCT</strong> to monitor attendances at ED, UCC and<br />
WICs and identify trends<br />
• Surge prioritisation plan to be initiated<br />
• Practice-specific situation: Advise patients to<br />
use NHS Direct and alternative health<br />
site/phone number until recovery plan<br />
implemented<br />
As for level 2<br />
Additional resource allocation to affected<br />
areas<br />
Alert Clinical and none clinical agencies that<br />
additional resources may be needed<br />
12
ESCALATION LEVEL 3 – SEVERE <strong>AND</strong>/OR PROLONGED EXCESS PRESSURE REQUIRING SUPPORT FROM ALL AGENCIES<br />
System Triggers @ Midday<br />
No. of patients in ED 60 – 70 Time to see Senior Decision Maker > 2.5 hours ED breaches 10-15 Averaged ED attendance by midday more than 130 Cancellation of elective admissions Critical Care<br />
Capacity = 0 Admissions unit capacity/bed capacity – 60-80 More than 15 patients awaiting Community beds EMAS REAP Level 3 WiC/UCC time to see Senior Decision Maker Consistently 4 hours<br />
INDIVIDUAL ORGANISATION TRIGGERS<br />
URGENT CARE CENTRE/ MIU’S/ WIC<br />
EMAS<br />
UHL<br />
SOCIAL CARE<br />
• Urgent Care Centre waiting times consistently<br />
4 hours<br />
As above and<br />
• Jobs awaiting allocation not decreasing after<br />
4 hours.<br />
• Full/protracted failure of CAD, COMS, Radio<br />
in Control.<br />
• Substantial negativity against Demand &<br />
Capacity plan.<br />
As above and<br />
• Deteriorating situation. Major shortfall in the<br />
numbers of beds for emergency admissions.<br />
Major incident has been declared<br />
internal/external to UHL and extra capacity<br />
needs to be created.<br />
• All of the actions outlined within a Bed Alert<br />
Status will take place with the addition of<br />
those for a level 3 Bed Alert Status that are<br />
given below:<br />
• Nursing placements signalling 97%<br />
occupancy<br />
• Staffing absences over 50% in Care<br />
Management and Home Care Staff<br />
• Residential placements signalling 97%<br />
occupancy<br />
System Actions<br />
• Implement Level 3 Escalation<br />
• ECN briefed on a daily basis after daily teleconference at 11.45am and again at 4pm to review situation and actions required.<br />
• UHL/COMMUNITY HOSPITALS to identify patients for awaiting discharge and any delays in accessing packages of care, community beds, community equipment CHC assessments to be raised to <strong>PCT</strong><br />
leads. <strong>PCT</strong> leads to ensure actions to reinstate flow be implemented where possible.<br />
• Increase capacity in community by offering additional hours to bank nurses /AHPs and / or commission additional hours from agency<br />
• Open up closed beds, spare beds in community hospitals<br />
• Chief Exec to decide to cancel operations<br />
• The executive on call will give consideration to instigating the <strong>PCT</strong>s Major Incident Plan should Acute Trust instigate theirs or the demand placed on the <strong>PCT</strong>s community services become excessive<br />
• Patient & public targeted communications strategy enacted across LLR<br />
INDIVIDUAL ORGANISATION ACTIONS<br />
URGENT CARE CENTRE / MIU’S/ WIC<br />
EMAS<br />
UHL<br />
SOCIAL CARE<br />
• Diverts and mutual aid between UCC and ED<br />
• Stand by staff called in<br />
• Implement Level 3<br />
• As for Level 2<br />
• Implement Level 3 escalation<br />
• Continue to mobilise and use additional<br />
resources whilst re-prioritising sustained<br />
activity.<br />
• Ensure all actions outlined in the daily<br />
operational plan have been actioned<br />
• If appropriate actions have not been taken the<br />
Clinical Business Unit Manager will be<br />
informed.<br />
• Divisional Senior medical/Nursing &<br />
Management teams informed of the need to<br />
implement high risk actions.<br />
• Inform health and social care community and<br />
Strategic health Authority of agreed level of<br />
community wide status<br />
• Implement Level 3 Escalation<br />
• As for Level 2<br />
• Implement Level 3 escalation<br />
• Commission additional interim care beds from<br />
nursing/care homes subject to appropriate<br />
funding approval<br />
• Extra staffing hours made available on a<br />
case-by-case basis, agreed by Area manager.<br />
• Adult duty workers and managers and Rapid<br />
response teams to put services in to prevent<br />
admission for suitable community based<br />
referrals.<br />
13
ESCALATION LEVEL 3 – SEVERE <strong>AND</strong>/OR PROLONGED EXCESS PRESSURE REQUIRING SUPPORT FROM ALL AGENCIES<br />
System Triggers @ Midday<br />
No. of patients in ED 60 – 70 Time to see Senior Decision Maker > 2.5 hours ED breaches 10-15 Averaged ED attendance by midday more than 130 Cancellation of elective admissions Critical Care<br />
Capacity = 0 Admissions unit capacity/bed capacity – 60-80 More than 15 patients awaiting Community beds EMAS REAP Level 3 WiC/UCC time to see Senior Decision Maker Consistently 4 hours<br />
INDIVIDUAL ORGANISATION TRIGGERS<br />
LPT – COMMUNIITY HEALTH SERVICES<br />
LPT – MENTAL HEALTH SERVICES<br />
PRIMARY CARE<br />
OUT OF HOUR’S<br />
• Significant reduction bed capacity<br />
• Significant and sustained staff shortages<br />
resulting in reduced capacity.<br />
• Sustained increased demand on<br />
services.<br />
• Sustained staffing difficulties linked to<br />
e.g. flu outbreak.<br />
• UHL declare major incident<br />
• Practices facing significant demand for<br />
appointment and/or home visits<br />
• Difficulty in accessing secondary care<br />
beds<br />
• Consortium/<strong>PCT</strong> Alert issued<br />
• Practice(s) Service Continuity Plan<br />
activated<br />
<br />
Sustained increase in call volumes<br />
across all operational areas with<br />
significant breaches against National<br />
Quaility Requirement standards.<br />
System Actions<br />
• Implement Level 3 Escalation<br />
• ECN briefed on a daily basis after daily teleconference at 11.45am and again at 4pm to review situation and actions required.<br />
• UHL/COMMUNITY HOSPITALS to identify patients for awaiting discharge and any delays in accessing packages of care, community beds, community equipment CHC assessments to be raised to <strong>PCT</strong><br />
leads. <strong>PCT</strong> leads to ensure actions to reinstate flow be implemented where possible.<br />
• Increase capacity in community by offering additional hours to bank nurses /AHPs and / or commission additional hours from agency<br />
• Open up closed beds, spare beds in community hospitals<br />
• Chief Exec to decide to cancel operations<br />
• The executive on call will give consideration to instigating the <strong>PCT</strong>s Major Incident Plan should Acute Trust instigate theirs or the demand placed on the <strong>PCT</strong>s community services become excessive<br />
• Patient & public targeted communications strategy enacted across LLR<br />
INDIVIDUAL ORGANISATION ACTIONS<br />
LPT – COMMUNITY HEALTH SERVICES<br />
LPT – MENTAL HEALTH SERVICES<br />
PRIMARY CARE<br />
OUT OF HOURS<br />
• As per level 2<br />
• On-call Director/Manager informed<br />
• Surge plans activated for NHS LC CHS<br />
• Stand by staff called in<br />
• Implement Level 3<br />
• As per level 2.<br />
• On-call Director/Manager informed<br />
• Implement Staff Mobilisation Plan, if<br />
necessary, (Refer to LPT Emergency<br />
Plan) to support hot-spots.<br />
• Systematic review of in-patients with<br />
discharge to community with appropriate<br />
support if safe to do so.<br />
• GP’s offering telephone consultations<br />
• GPs offering more urgent appointments<br />
• 999 Cat C patients being taken directly to<br />
WIC’s, UCC, 8-to-8 centres instead of<br />
ED.<br />
• Implement relevant actions specified in<br />
Service Continuity Plan<br />
• Follow Consortium/<strong>PCT</strong>/PH advice or<br />
action plans<br />
• Implement available bank/agency<br />
arrangements to cover<br />
doctor/nurse/admin shortages<br />
• Support or seek support of neighbouring<br />
practices, especially for single-handed<br />
practices<br />
• Support of OOH service<br />
<br />
<br />
<br />
<br />
<br />
<br />
Additional resources where appropriate<br />
Additional PCC sessions<br />
Clinical streamning to bases and home<br />
visiting teams<br />
Daily performance and capacity reviews<br />
Escalation to GP consortia<br />
Cross working with other CNCS locations<br />
14
ESCALATION LEVEL 4 – EXTREME PRESSURE REQUIRING IMMEDIATE <strong>AND</strong> SIGNIFICANT ACTION<br />
System Triggers @ Midday<br />
No acute beds available or in near future No capacity in ED (all trolleys and bays full) Increasing number of patients waiting in ED >6 hours Time to see Senior Decision Maker > 4 hours<br />
EMAS REAP Level 4/5/6<br />
INDIVIDUAL ORGANISATION TRIGGERS<br />
URGENT CARE CENTRE/ MIU’S/ WIC<br />
EMAS<br />
UHL<br />
SOCIAL CARE<br />
• Urgent Care Centre waiting times consistently<br />
4 hours<br />
As above and<br />
Continuation of level 3 factors<br />
As above and<br />
• On very rare occasions, the Trust may find<br />
itself in a position whereby it continues to be<br />
on a Red Bed Alert with all available capacity<br />
used and minimal predicted discharges<br />
occurring over the next 24 hours. The situation<br />
may be compromising the care and safety of<br />
patients with the increasing risks associated<br />
with prolonged waits in ED.<br />
• As for level 3<br />
System Actions<br />
• Implement Level 4 Escalation<br />
• ECN briefed on a daily basis after daily teleconference at 11.45am and again at 4pm to review situation and actions required.<br />
• UHL/COMMUNITY HOSPITALS to identify patients for awaiting discharge and any delays in accessing packages of care, community beds, community equipment CHC assessments to be raised to <strong>PCT</strong> leads.<br />
<strong>PCT</strong> leads to ensure actions to reinstate flow be implemented where possible.<br />
• Increase capacity in community by offering additional hours to bank nurses /AHPs and / or commission additional hours from agency<br />
• Open up closed beds, spare beds in community hospitals<br />
• Chief Exec to decide to cancel operations<br />
• The executive on call will give consideration to instigating the <strong>PCT</strong>s Major Incident Plan should Acute Trust instigate theirs or the demand placed on the <strong>PCT</strong>s community services become excessive<br />
• Patient & public targeted communications strategy enacted across LLR<br />
INDIVIDUAL ORGANISATION ACTIONS<br />
URGENT CARE CENTRE / MIU’S/ WIC<br />
EMAS<br />
UHL<br />
SOCIAL CARE<br />
• As for level 3<br />
• Deployment of Major Incident Support Unit<br />
• Activation of Major Incident Plan<br />
• Exceptional bed management meeting to be<br />
held at the LRI to identify actions to improve<br />
bed situation.<br />
• Chair – Director of Operations/Nursing<br />
• Divisional /Senior Managers for all Divisions/<br />
Divisional/ Clinical Director for<br />
Medicine/CSSD/EMAS/Pathology/Discharge<br />
Team/Imaging/ED/on call manager and<br />
Director on call/Admission and Discharge<br />
Manager<br />
• Trigger points for identifying the need for<br />
exceptional bed meetings will be during the<br />
site bed meetings throughout the day.<br />
As for Level 3<br />
15
ESCALATION LEVEL 4 – EXTREME PRESSURE REQUIRING IMMEDIATE <strong>AND</strong> SIGNIFICANT ACTION<br />
System Triggers @ Midday<br />
No acute beds available or in near future No capacity in ED (all trolleys and bays full) Increasing number of patients waiting in ED >6 hours Time to see Senior Decision Maker > 4 hours<br />
EMAS REAP Level 4/5/6<br />
INDIVIDUAL ORGANISATION TRIGGERS<br />
LPT – COMMUNITY HEALTH SERVICES<br />
LPT – MENTAL HEALTH SERVICES<br />
PRIMARY CARE<br />
OUT OF HOURS<br />
• As for level 3<br />
• Significant reduction bed capacity<br />
• Sustained and severe staff shortages<br />
resulting in significant reduced capacity<br />
with potentially unsafe situations<br />
occurring.<br />
• As for level 3<br />
• Significant demand on services.<br />
• Sustained and severe staffing difficulties<br />
linked to e.g. flu outbreak.<br />
As for level 3 plus<br />
Practice experiencing severe and continuing<br />
difficulties in providing or maintaining services, due to<br />
pandemic situations, staff shortages or other practice<br />
specific emergency<br />
Continued and extended activation of Service<br />
Continuity Plan<br />
Closure of practice or associated pharmacy<br />
Service delivery difficulties notified by<br />
Community/DN teams<br />
As for level 3<br />
System Actions<br />
• Implement Level 4 Escalation<br />
• ECN briefed on a daily basis after daily teleconference at 11.45am and again at 4pm to review situation and actions required.<br />
• UHL/COMMUNITY HOSPITALS to identify patients for awaiting discharge and any delays in accessing packages of care, community beds, community equipment CHC assessments to be raised to <strong>PCT</strong> leads.<br />
<strong>PCT</strong> leads to ensure actions to reinstate flow be implemented where possible.<br />
• Increase capacity in community by offering additional hours to bank nurses /AHPs and / or commission additional hours from agency<br />
• Open up closed beds, spare beds in community hospitals<br />
• Chief Exec to decide to cancel operations<br />
• The executive on call will give consideration to instigating the <strong>PCT</strong>s Major Incident Plan should Acute Trust instigate theirs or the demand placed on the <strong>PCT</strong>s community services become excessive<br />
• Patient & public targeted communications strategy enacted across LLR<br />
INDIVIDUAL ORGANISATION ACTIONS<br />
LPT – COMMUNITY HEALTH SERVICES<br />
LPT – MENTAL HEALTH SERVICES<br />
PRIMARY CARE<br />
OUT OF HOURS<br />
• Emergency Plan triggered with TCG convened.<br />
• Consideration of Implementing LPT Service<br />
Reduction Plan (Refer to LPT Emergency<br />
Plan).<br />
• Reallocation of staff to support DN Teams as<br />
per Business Continuity Plans<br />
NHS DIRECT TRIGGERS <strong>AND</strong> ACTIONS<br />
• Emergency Plan triggered with TCG<br />
convened.<br />
• Consideration of Implementing LPT<br />
Service Reduction Plan (Refer to LPT<br />
Emergency Plan).<br />
• As for Level 3, plus<br />
• Notify Pharmacies of practice closures and<br />
vice-versa<br />
As for level 3<br />
NHS DIRECT<br />
• CALL Abandonment rate less than 4%<br />
• Calls transferred immediately to a Nurse Advisor<br />
• Staff deployed to normal duties<br />
• Incoming call volume stable<br />
NHS DIRECT<br />
• Expect increased call volume<br />
• Put out information on health alerts and how to<br />
care for viruses.<br />
• More staff rostered on at Christmas particularly<br />
OOH period.<br />
• Issue information on repeat prescriptions over<br />
bank holidays<br />
NHS DIRECT<br />
• CALL Abandonment rate above 4 %<br />
• Only priority 1 calls not transferred immediately to<br />
a Nurse Advisor<br />
• Some redeployment of staff onto other duties<br />
• Peaks in call volume<br />
• Implement Level 2 Escalation<br />
NHS DIRECT<br />
• CALL Abandonment rate above 4 %<br />
• Only priority 1 calls not transferred immediately to<br />
a Nurse Advisor<br />
• Some redeployment of staff onto other duties<br />
• Peaks in call volume<br />
• Implement Level 2 Escalation<br />
16
ESCALATION <strong>AND</strong> DE-ESCALATION PROCESS<br />
LLR ESCALATION PROCESS LLR DE-ESCALATION PROCESS<br />
Urgent Care Leads: Urgent Care Leads:<br />
LLR <strong>PCT</strong> Cluster Rachna Vyas 0116 295 4179 / 07935 390 092<br />
UHL Richard Jarvis 07950 661 644<br />
LPT John Mullan 0116 225 2878 / 07970051282<br />
Social Services County Jackie Wright 07881 836331<br />
Social Services City Ashraf Osman 0116 221 1555 / 07794 053 465<br />
EMAS 999 Mick Jones 07970 399 643<br />
EMAS PTS Mick Byrne 07974247583<br />
LLR <strong>PCT</strong> Cluster Rachna Vyas 0116 295 4179 / 07935 390 092<br />
UHL Richard Jarvis 07950 661 644<br />
LPT John Mullan 0116 225 2878 / 07970051282<br />
Social Services County Jackie Wright 07881 836331<br />
Social Services City Ashraf Osman 0116 221 1555 / 07794 053 465<br />
EMAS 999 Mick Jones 07970 399 643<br />
EMAS PTS Mick Byrne 07974247583<br />
17
CONTACTS<br />
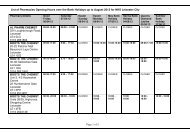
A full list of contacts including roles and job titles is included as Appendix 1 to the 2011/12 Winter Resilience Plan.<br />
The LLR <strong>PCT</strong> Cluster will act as the “communication cell” for the escalation plan. The different organisations will communicate their pressure<br />
problems and status of alert to the Urgent Care Lead so that the overall picture in the Health and Social Care Community is known at any one time.<br />
LLR <strong>PCT</strong> Cluster in hours contacts are: Rachna Vyas 07768 746 689, Amita Chudasama 07825 113 656 and Ket Chudasama 07760 990 396.<br />
The table below details how to contact organisations during out of hours.<br />
ORGANISATION<br />
Director on call for Leicester, Leicestershire and Rutland <strong>PCT</strong> Cluster<br />
CONTACT NUMBER<br />
07623 908865. Leave a message and a contact number<br />
Senior Manager for Leicester City Community Health Services 07789 865076<br />
Senior Manager for Leicestershire County and Rutland Community<br />
Health Services<br />
Director on call for University Hospitals of Leicester<br />
Director on call for Leicester Partnership Trust<br />
01509 611600 and ask to be put through to the CHS Senior Manager on<br />
call<br />
0300 303 1573 and ask to be put through to the Director on call.<br />
0116 225 6000 and ask to be put through to the Director on call.<br />
Out of Hours on Call Manager 0116 295 0076<br />
CNCS on Call Manager 03000 241118<br />
Urgent Care Centre (George Eliot on call Director)<br />
02476 351351 and ask for the on call Director<br />
18
Leicester, Leicestershire & Rutland Cluster<br />
Director Lead - Dr Simon Freeman, Director of Contracting, Information and Performance, LLR <strong>PCT</strong> Cluster<br />
Management Lead - Rachana Vyas, Planning and Delivery Speicalist, LLR <strong>PCT</strong> Cluster<br />
LLR EMERGENCY CARE NETWORK: Emergency Care Network (ECN)<br />
Chair: Cahterine Griffiths, Chief Executive, LLR <strong>PCT</strong> Cluster<br />
Facilitation of group: Rachna Vyas, Planning and Delivery Specialst, <strong>PCT</strong> LLR Cluster<br />
The LLR Emergency Care Network is operationally supported by the Senior Operational Group and the Clinical Interface Group. Stakeholders from across<br />
the Health Economy are present at this monthly meeting including Clinical Commissioning Group representation. During periods of surge the group will:<br />
1. Move to weekly meetings<br />
2. Communicate escalation levels across the health economy<br />
3. Facilitate mitigating actions to resume flow through the system<br />
4. Manage any other issues affecting system performance where possible<br />
Leicester, Leicestershire and Rutland<br />
Winter Resilience Plan 2011/12<br />
Governance and Performance Management<br />
Full details of all organisational leads and contact details can be found in Appendix 1<br />
ESCALATION PROCESS:<br />
1. The ECN will nominate urgent care leads from each organisation in the health economy to participate in a short daily<br />
telephone conference call at 11.45am to advise of pressures and initiate mitigating actions.<br />
2. The chair of this teleconference will send out an alert to the ECN distribution list, detailing the escalation level and mobilising<br />
agencies to enact the escalation plan, (detailed as Appendix 3).<br />
3. If necessary, a further teleconference will take place at 4pm to assess progress against the actions required.<br />
LLR wide SITREP reporting guidance is shown in Appendix 4. LLR Cluster will be copied into SITREP submissions and any<br />
cancellations will be outlined at the daily 11.45am teleconference.<br />
Plans will also be shared across the East Midlands area to enhance cross-border working and promotion of best practice across the region.<br />
Performance management of the system<br />
The ECN receive a weekly performance report.<br />
The ECN receive a performance dashboard detailing the system performance monthly.<br />
Each part of the system will be performance managed against agreed targets and ECN meetings will focus on those areas which are red rated<br />
Page 1
Operational management of the LLR Urgent and Emergency care system<br />
Management of system capacity & demand<br />
All providers have submitted evidence that gives assurance that capacity will meet both elective and emergency demand over the winter months.<br />
This is listed as Appendix 8: Contingency Strategies, Flu Pandemic plans, Business Continuity Plans and Incident plans are complete andare kept in a<br />
central folder by LLR <strong>PCT</strong> Cluster.<br />
A joint workshop was held with all stakeholder organisations to revise the Escalation Plan. A LLR wide escalation plan has been created and<br />
distributed to all organisations for use as required during periods of surge. This is shown in Appendix 3.<br />
Specific arrangements made for 11/12:<br />
The 3 Clinical Commissioning Group's (CCG's) across the city and county have developed individual Business Continuity<br />
Plans detailing the critical and non-critical functions of service provision. Trigger points have been identified in conjunction with<br />
the Winter Resilience Group which will enable them to identify if and when to temporarily stop routine tasks until demand<br />
reduces. These plans were developed in response to a Flu Pandemic with the support of the LMC but can be used in all<br />
emergency planning situations.<br />
Primary Care<br />
In addition, each Primary and Community Care directorate has an overarching Business Continuity Plan which details how<br />
operational activity would be maintained in case of any incident (including adverse weather and influenza pandemic). The plan<br />
also details how members of the team would communicate with all independent contractors to make them aware of issues<br />
affecting the wider health community.<br />
Primary Care Contracts teams have encouraged GPs and Pharmacists to open additional hours over the Christmas/New Year<br />
period to ease pressure on Secondary Care and Out Of Hours services. The collated list of opening times will be published to<br />
patients so they know when and where to go if they become ill. Also all GP Practices in the CIty and County have a buddy<br />
practice, practices use their buddy for relocation purposes if their practice became uninhabitable due to a business continuity<br />
incident, some practices use their buddy to share staff if either were faced with severe staff shortages and some have an<br />
agreement for both. A list of "Buddy Practices" can be found at Appendix 5.<br />
• Single Point of Access/Bed Bureau - A 3 month pilot was completed in October 2010. The aim of the pilot was to deflect any<br />
unnecessary acute hospital admissions to either a Community Hospital bed or a community service. This project was aimed at<br />
strengthening the interface between Secondary and Primary care. Gaps in service pathways were identified through the SPA<br />
integration pilot and exposed specific pathways that required further work, such as AUR. Pathways have been put in place<br />
since the end of the pilot and further work continues on other specific pathways.<br />
A single point of access is available for GPs and EMAS to access urgent response from community services 24/7. Work is<br />
underway to:<br />
Integrate City and County SPA/bed bureau<br />
Facilitate bed bureau pathway<br />
Complete and validate EDoS<br />
Roll out to SPA and associate clinicians<br />
A range of clinical pathways have been approved to support admission avoidance cellulites pathway, Acute Urinary Retention<br />
pathway, EOL Pathway. Agreed criteria for direct admission to community hospitals is shared with EMAS, GP and acute care<br />
colleagues. Access to community nursing service out of hours is centralised. Specialist Palliative Care Service available for<br />
city and county 2200-0800 7 days which is co-located with the out of hours service. Long term conditions hub is co-located<br />
with SPA and out of hours service communication centre. All LTC patients have special patient note with Out of Hours service<br />
to share end of life and acute exacerbation management plan.<br />
City Community Health Services<br />
Community Health Services • On a weekly basis the AD of Adult services meets with Operational leads to discuss service delivery<br />
• Daily review of all patients in intermediate care and rehabilitation beds to improve bed occupancy. Additional bed capacity<br />
available for up to seven beds in spot purchased care home beds.<br />
• 24/7 day a week service based on our Clinical Intermediate Care Unit with 11 beds.<br />
• Where possible, the Rapid Intervention Team (RIT) will provide care at home in order to reduce demand on bed space.<br />
• Process in place to identify vulnerable patients as part of the pandemic flu response. This information is updated weekly and<br />
provided to the Clinical Lead for Out of Hours.<br />
County Community Health Services<br />
• Community Hospital bed closures due to outbreak of infection are minimised by robust infection control procedures.<br />
• All organisations now have access to an ‘in-hours’ Countywide Bed Manager and bed escalation plan in place, developed in<br />
collaboration with UHL.<br />
• Daily review of patients in UHL waiting to be transferred to Community services / Community Hospitals by Primary Care<br />
Coordinators<br />
• Admission criteria agreed to enable direct access to community beds by GPs, community staff and EMAS<br />
• Podiatric Surgery, General Surgery, Urology and Orthopaedic day Case capacity is available in community Hospitals.<br />
• Access to diagnostic services including Endoscopy & H- Pylori breath testing in community services to avoid unnecessary<br />
admissions (via GP surgeries for NHS LCCHS). All Imaging departments in LCRCHS will be open as usual apart from the<br />
Bank Holiday Days themselves offering support to Direct Access, MIU and OPD referral with access to x-ray, ultrasound and<br />
MR as planned<br />
• Telephone Help Line available to all patients known to LTC service and to health professionals requiring advice or access to<br />
LTC Service (Mon - Friday 0800-1830)<br />
Page 2
City and County Community Health Services have business continuity plans for community intermediate care service to<br />
support people in their own homes.<br />
• They have Single Point of access (for adult services), which helps direct clinicians to use pathways as an alternative to UHL<br />
Community Health Services<br />
and provides direct link to intermediate care service 24/7.<br />
– Intermediate care<br />
• Rutland’s Intermediate Care team directly commission home care from Fraser’s agency as appropriate<br />
• NHS LCRCHS has a 24/7 community nursing service available across all localities.<br />
• Specialist end of life team is available 7/7 over night to support end of life care in city.<br />
Urgent Care Centre, 8-8<br />
Centre's, Walk-In Centres<br />
and Minor Injury Units<br />
The Urgent Care Centre, co-located with ED will be open 24/7 over the winter period. This will take most minor<br />
injuries/illnesses releasing capacity in ED to deal with more complex cases.<br />
There is a WiC at Loughborough, two 8-8 centres, 1 in the City at Merlyn Vaz Health Centre and 1 at Oadby and three MIU’s at<br />
Rutland, Market Harborough, and Melton. All have differing criteria and different hours of service (dates/times of opening<br />
shown in holiday cover section of this plan)<br />
The range of community services and community hospital are available to the WIC and Out of Hours service through<br />
specifically trained Nurses who can navigate the patient to the most appropriate service. All patients contacting the out of hours<br />
service can e routed to an alternative community service seamlessly including access to Marie curie staff for EOL care.<br />
NHSD <strong>AND</strong> EMAS can warm transfer calls to the out of hours service when required.<br />
OoHs can warm transfer calls to EMAS if condition life threatening.<br />
EMAS on scene with patient can contact OoH and will be immediately put through to first available clinician.<br />
Cat C patients can be referred 24 hours a day to SPA for response by community services for agreed pathway or direct<br />
admission to community hospitals.<br />
OoHs GPs support Community Hospitals out of hours to support patients who require medical intervention to prevent transfer<br />
to acute sector.<br />
EMAS – 999<br />
• Senior decision makers at front door of receiving bay to prevent ambulance queuing and any negative impact on ambulance<br />
turnaround times<br />
• EMAS will liaise with UHL on a daily basis if there are any issues that need resolving, including those impacting on<br />
turnaround times etc.<br />
• Operational manager will be stationed at ED to ensure smooth turnarounds, both pre and post clinical handover.<br />
• A deep clean team will also be stationed at ED to facilitate faster post handover times. These will be monitored daily and<br />
trends will be highlighted to the ECDG where necessary.<br />
• All departments to accept handover within 15 minutes of arrival<br />
• EMAS will divert suitable Category C patients to the Urgent Care Centre instead of ED<br />
• Potential pathway in place to divert patients to either SSAFA 8-8 or Oadby 8-8 centres to reduce pressure on the urgent care<br />
centre and ED.<br />
• Currently if pressures arise EMAS look to divert at the borders, this is by local agreement at the time of the pressure.<br />
• EMAS have direct access to community hospitals, access to nurse advice via community nursing/Single Point of Access and<br />
direct transfer to Walk- in centre or Minor Injury Unit<br />
PTS is redesigning its delivery model in line to meet expected workloads throughout the coming year. This includes using<br />
existing technology to match resources with activity on a weekly basis. Establishment levels are also being reconsidered.<br />
EMAS – PTS<br />
Social Services<br />
Social Services<br />
Reablement services<br />
• Locality contract meetings and EMAS task and finish group meetings merged in preparation for winter pressures to ensure<br />
alignment between measures taken and contractual processes.<br />
• Both city and county social services will continue to deliver to the standards set for achievement of section 2’s and section 5’s<br />
within a set time period.<br />
• Identified social worker for all Community Hospitals integrated with Multi Disciplinary Teams<br />
• Access to social care re-ablement and assessment beds.<br />
• Step down beds available in residential homes<br />
• Involvement of social services in operational planning groups<br />
• Criteria for referral to Social Services respite/rehabilitation beds in place<br />
• LC Adult Social Services has existing systems of negotiation between Health and Social care i.e. Discharge Liaison Staff<br />
(Health) and Team Managers (Social Services.) Staff work flexibly over 7 days.<br />
• The hospital teams ensure that individuals are discharged safely with social care when and where it is needed.<br />
• The County HART reablement service takes patients directly from hospital into reablement through the customer service<br />
centre.<br />
• Additional capacity is sought from the independent sector when there is an overflow.<br />
• Reablement beds have been identified in independent sector residential homes to facilitate discharge and reablement, for<br />
example for stroke pathway patients.<br />
• Council is engaged in planning re: winter pressures.<br />
Discussed at standing management meetings as part of the capacity agenda where mitigation and planning takes place to<br />
ensure that cases presented are taken.<br />
Page 3
Care Homes/CHC<br />
Community equipment<br />
• Work is ongoing with the Care Homes Advisory Group to ensure that delays in assessments prior to discharge are minimised.<br />
• The CHC team will facilitate placements prior to tariff being agreed at times of surge. The CHC process has been<br />
streamlined and this work will continue throughout 11/12.<br />
Community equipment services have transferred to Nottingham Rehab Services from the British Red Cross on 1 April 2011.<br />
• Where a patient is ready for discharge and a delay is due to the lack of suitable community equipment being sourced, the<br />
Community Equipment team will expedite the ordering and delivery of emergency community equipment orders.<br />
• A process has been agreed with the community equipment team and communicated across the health economy.<br />
Mental health<br />
UHL – ED<br />
UHL – ED<br />
• LPT have liaison psychiatry service based in ED who take responsibility for all psychiatry referrals during 9-5 on weekdays to<br />
make single comprehensive assessments so that multiple assessments are avoided and patients wait times in ED are<br />
reduced.<br />
• Crisis resolution team to prioritise patients at ED in order to reduce demand on ED resource<br />
• LPT has access to NHS professional’s bank if required due to staff shortages.<br />
• LPT are part of the Winter Resilience Group and have a presence on the daily teleconference calls to help expediate any<br />
issues with mental health patients.<br />
• Medical staffing cover arrangements in place to address peaks in demand<br />
• STAT team in place and operational between 9 am and 6 pm every day. This should ensure patient flow through the<br />
department.<br />
• Breach analysis circulated each day to understand and mitigate against further breaches of the 4 hour standard.<br />
• Comjmunity Health Services have a primary care team working in UHL including in the Emergency Department to facilitate<br />
the flow of patients through Health and Social care system. These posts reduce inappropriate unscheduled admissions to UHL<br />
by facilitating packages of care in a community setting where appropriate and reduce occupied bed days by facilitating timely<br />
and appropriate discharge<br />
• All walk in, ambulatory patients presenting at adult ED between 10am and 10pm, 7 days a week (inc bank holidays) are given<br />
30 second initial assessment at the front door of the ED by a senior nurse practitioner. These patients will then be streamed to<br />
either ED or the UCC for any further assessment necessary and treatment.<br />
• Other ambulatory pathways are being put into place to minimise admissions via ED. The pulmonary embolism pathway is in<br />
place and this is being replicated for other relevant and appropriate ambulatory care sensitive conditions.<br />
• Escalation process put in place between ED and other specialties to ensure that specialties take ownership of patients<br />
waiting in ED.<br />
ED have recruited 6 Advanced Nurse Practitioners, 4 Physician Assistants and 4 Consultants in 2011.<br />
Emergency Department Standards<br />
Operational Standards<br />
• Medical Staff resources aligned to demand<br />
o Ensure junior staff aligned to demand and check for variance four monthly<br />
o Consultant clinical presence targeted at busiest times to ensure optimal early decision making and patient care.<br />
• Emergency Nurse Practitioners aligned to demand<br />
• Check for variance 4 monthly<br />
Timelines<br />
1) Resuscitation Area<br />
• Category 1 Patient – Seen on Arrival by Doctor and nurse<br />
• Category 2 Patient<br />
o Seen on arrival by nurse<br />
o Seen by doctor within 20 minutes<br />
• Decision made by 90 minutes<br />
• Ready for admission/transfer by 150 minutes<br />
2) Paediatric ED<br />
• All patients seen by practitioner within 45 minutes<br />
• Decision made by 90 minutes<br />
• Discharge/admit by 120 minutes<br />
• If other specialist needs to review discharge/admit within 150 minutes<br />
3) Majors Area<br />
• Category 2 patient s assessed (nurse+/- doctor) within 30 minutes<br />
• Category 3 patients assessed (nurse+/- doctor) within 45 minutes<br />
• All patients to have all necessary bloods and ECGs carried out within 40 minutes<br />
• All X-rays and scans required to be ordered within 40 minutes<br />
• All patients to have a decision by 120 minutes<br />
• All patients not requiring specialist review in department admitted or discharged within 3 hours<br />
• All patients requiring specialist review admitted or discharged within 3 hours 30 mins<br />
Page 4
UHL – ED<br />
UHL – ED<br />
MONITORING<br />
Real Time<br />
• Coordinator for each area monitors assessment, decision and dispersal times<br />
• Coordinator informs NIC when concerned re patients not likely to be seen within standard times.<br />
• NIC assesses information. Liaises with Consultant/SpR in charge and after assessing whole department and resources<br />
available institutes relevant escalation.<br />
Audit<br />
• Regular monthly audit of waiting time standards for each area<br />
• Discussed at CBU Manager/Lead Clinicain meeting and fed back to staff on a monthly basis<br />
• Resource allocation to demand reviewed<br />
• Run charts for each standard developed<br />
Escalation<br />
Will depend on severity of situation and resources available to resolve it already in place in ED.<br />
Resuscitation Area<br />
1) Category 1 patients must be seen on arrival by a doctor.<br />
• If escalated senior doctor must attend the resuscitation room and with the nurse coordinator quickly assess all patients not yet<br />
seen.<br />
• Allocate additional medical staff from other areas as required. Must ensure all patients in the department are safe<br />
2) Decision made in 70 minutes<br />
• Coordinator escalates to NIC at 45 minutes if not confident of decision being made in time. NIC and senior doctor assess<br />
situation and liaise directly with medical team.<br />
3) Category 2 patients in the resuscitation room must be seen by a doctor within 15 minutes.<br />
• If escalated senior doctor must attend the resuscitation room and with the nurse coordinator quickly assess all patients not yet<br />
seen.<br />
• Allocate additional medical staff from other areas as required. Must ensure all patients in the department are safe<br />
Paediatric ED<br />
4) Category 2 patients must be seen by assessed within 30 minutes<br />
• If escalated senior doctor must attend and with the nurse in charge to quickly assess all patients for rapid prioritisation.<br />
• Must ensure that the agreed processes of care are being followed.<br />
• Ensure medical staff are working on medical tasks only and are aware of the situation.<br />
• Where possible senior doctor should attempt to use any middle grade or consultant staff to reassess needs of these patients<br />
ensuring particularly that pain relief is given.<br />
• Some patients may be able to be categorised as a priority 3 by such actions.<br />
• Consider reallocation of medical resources<br />
5) Category 3 patients must be assessed within 60 minutes<br />
• If escalated senior doctor must attend with the nurse in charge to quickly assess all patients for rapid prioritisation<br />
• Must ensure that the agreed processes of care are being followed.<br />
• Ensure medical staff are working on medical tasks only and are aware of the situation.<br />
• Consider reallocation of medical resources<br />
6) Category 3 patients must have a decision made within 120 minutes<br />
• Senior doctor alerted by area 3 coordinator at 90 minutes if expects standard will not be met.<br />
• He/She will liaise directly with patient’s doctor to facilitate decision.<br />
7) All patients not requiring specialist review in department admitted or discharged within 3 hours<br />
• Senior doctor alerted by area 3 coordinator at 150 minutes if expects standard will not be met.<br />
• Senior doctor liaises directly with patient’s doctor<br />
Majors<br />
If any of standard times are unlikely to be met nurse coordinator and senior doctor for the area must ensure processes being<br />
followed.<br />
Will liaise with NIC and senior doctor to look at possible reallocation of doctors to the area for a limited time.<br />
Reallocation of Medical Resources<br />
• Assess medical staff on duty and number of ENPs. Ensure all are present.<br />
• Assess whether reallocation is necessary (eg if nothing changes will the situation resolve itself ( a small bulge of attendances)<br />
If possible reallocate staff from other areas<br />
• If paediatric ED is under pressure can we send an ENP from Majors or a doctor to help. Vica versa.<br />
• If adult areas 3 under pressure can Paediatric medical staff see all category 6 patients? Could a paediatric doctor be pulled to<br />
help see category 3 patients?<br />
• Medical staff must ensure that their patients are not forgotten if they move to another area.<br />
Strain on nursing Resources<br />
If nursing staff are stretched it remains essential that where possible investigations such as bloods and ECGs are done at the<br />
initial assessment, by the HCA/Phlebotimist<br />
NIC consider asking Transfer Team/Pulling Nurse to collect patients and X-ray to collect and return patients.<br />
Ensure senior doctor is aware of stresses and considers alternative staff to take bloods and order X-rays early.<br />
Page 5
UHL – ED<br />
UHL – General<br />
UHL - Bed Management<br />
General Principles<br />
• Nursing staff at initial assessment follow investigation guidelines and discuss immediately with area coordinator or senior (not<br />
junior) doctor if unsure of relevant tests or patient has abnormal physiology<br />
• Junior doctors to ask for advice from SpR/consultant immediately after seeing a patient if not sure of a plan (waiting for<br />
bloods is not a plan)<br />
• Junior doctors must not ask for additional tests without consulting a senior<br />
• Any doctor asked to move from one clinical area to another must hand over his/her patients to a colleague before moving<br />
• If one clinical area is quiet senior doctor should look at reallocating medical staff before any escalation is required.<br />
• A timely correct assessment will help ensure a timely decision and good patient care<br />
• Patients in severe pain must be a category 2 as a minimum<br />
CLINICAL ST<strong>AND</strong>ARDS<br />
Based on CEM clinical standards<br />
1) Myocardial Infarction If Thrombolysis<br />
• Door to ECG 10 minutes (90%)<br />
• Door to Needle 30 minutes (75%)<br />
• Aspirin given 90% (if not contraindicated)<br />
2) Pain<br />
• Patients in severe pain (pain score 7 to 10) should receive appropriate analgesia according to local guidelines,<br />
• 50% within 20 mins of arrival or triage whichever is the earliest.<br />
• 75% within 30 mins of arrival or triage whichever is the earliest.<br />
• 98% within 60 mins of arrival or triage whichever is the earliest.<br />
• 90% of patients with severe pain should have documented evidence of re-evaluation and action within 30 minutes of<br />
receiving the first dose of analgesic.<br />
• Patients with moderate pain (pain score 4 to 6) should be offered or receive analgesia, according to local guidelines,<br />
• 75% within 30 mins of arrival or triage whichever is the earliest.<br />
• 98% within 60 mins of arrival or triage whichever is the earliest.<br />
3) Fractured Neck of Femur<br />
• Pain should be managed as above<br />
• 75% of patients should have an X-ray within 60 minutes of arrival or triage whichever is the earliest.<br />
• Only patients fit to be fast tracked should follow this pathway<br />
• 100% of patients should be admitted within 4 hours of arrival.<br />
• Hip fracture pathway should be used within ED<br />
4) Paracetamol Overdose<br />
• Patients should not have plasma levels measured earlier than 4 hours after the estimated ingestion time.<br />
• Staggered overdoses. Treatment started within one hour of arrival.<br />
• Patients arriving < 8 hours after ingestion. Treatment given appropriately as judged by presentation time and the treatment<br />
guidelines from National Poisons Information Service 2003.<br />
• Patients arriving 8 to 24 hours after ingestion. Treatment started before blood results available if there is a clear history of ><br />
12 g ingestion (or 150 mg/kg whichever is the smaller).<br />
• Patients presenting > 24 hours. INR, urea and electrolytes, bicarbonate & LFTs performed<br />
• Three times a day there will be a Trust Wide bed meeting at 8.30am, 12pm and 4pm to discuss the available capacity,<br />
staffing, ED attendences, EMAS capability and all other UHL issues relating to admission and discharge. This will then<br />
determine the appropriate escalation and de-escalation measures as that are required.<br />
•Information from the 10am bed meeting is then collated for the 11.45 health community conference call chaired by the <strong>PCT</strong><br />
commissioners where de-escalation will be declared.<br />
•Twice daily ward/board rounds including at weekends and bank holidays and other peak periods.<br />
• Patients will be outlayed in other directorate beds where capacity and infection control policies allow.<br />
• If required elective activity will be reduced, notwithstanding the fact that the 18-week target will not be compromised.<br />
• Each Clinical Business Unit has it's own internal staffing Business Continuity Plan to cover managing patient flows and for<br />
escalating staffing issues. A step by step approach for ensuring that staffing shortages are escalated and covered accordingly<br />
is in place in each CBU. If staffing levels are not appropriate and all measures are taken to assist then it will be escalated via<br />
the bed meetings in hours and to the duty manager out of hours.<br />
•Appropriate use of bank/agency staff has been agreed. In addition, UHL would look to utilising staff with a clinical registration<br />
to assist where appropriate.<br />
• Stringent infection control measures are in place, with work ongoing to identify and agree a separate ward space for infection<br />
control purposes.<br />
•At all times patient safety is paramount and no actions should take place that will put patients at risk whilst endeavouring to<br />
meet national targets.<br />
The UHL Bed Management Policy, details actions that UHL will take to manage the emergency admission process, bed<br />
capacity and the associated hospital status for internal escalation. The Bed Management Policy is Appendix 2 to the 2011/12<br />
Winter Resilience Plan.<br />
Each day following assessments of overall bed capacity, the Admissions and Discharge Manager will determine the level of<br />
bed alert within UHL in hours Monday – Friday 8am – 5pm, out of hours this is the responsibility of the duty manager in<br />
discussion with the senior manager on call.<br />
The Trust’s aim is to start each day on a Normal Status and escalate where appropriate i.e. after discussions of bed capacity at<br />
the 8.30 bed meeting. The decision will be based on the predicted shortfall in capacity.<br />
• The multi-agency Transition Planning Steering Group has replaced the Discharge Operational Group to deal with delays in<br />
discharge. This group will escalate any unresolved issues to the ECN.<br />
The LLR Cluster jointly with UHL are working on a project to increase the number of patients discharged by lunchtime. The<br />
focus will be on acute medical wards and work will be carried following a review of data and benchmarking against other<br />
organisations. A project plan is in place and roll out has commenced.<br />
• Patients ready for discharge who are suitable for the discharge lounge to be identified at the 11am bed meeting. These<br />
UHL – discharge processes<br />
patients should be in the discharge lounge by 1pm. HCA’s from the discharge lounge to aid movement of these patients at<br />
times of surge.<br />
• The discharge lounge and EMAS PTS coordinator to commence regular meetings to facilitate communications.<br />
• Working to the Delayed Discharge Act, Hospital Social Work Teams and Intermediate care Social Work teams have priority<br />
access to domiciliary care and interim residential beds.<br />
• Leicestershire County Adult Social Services – Emergency Discharge Team cover is commissioned for unplanned provision<br />
needed during OOHs periods.<br />
Page 6
The Trust use the following predictive tools to forecast bed occupancy and to help inform decisions relating to escalation<br />
levels.<br />
1) ED regression model (using historical levels and predicted temperatures) updated weekly which shows expected levels of<br />
daily attendances for the next couple of weeks<br />
2) Duty managers and bed managers working to an expected level of 150 acute emergency admissions a day with 3 meetings<br />
a day to monitor progress and agree plans to use contingency beds as appropriate.<br />
3) Weekly reports made available looking at historical monthly levels of emergency patients staying in hospital overnight for the<br />
last 5 years for reference.<br />
4) Daily ED reports e-mailed showing daily levels of ED attendances, breaches and admissions to the Trust.<br />
Page 7
UHL - Escalation Planning<br />
& Predicitve Tools<br />
UHL - Children's Services<br />
UHL – critical care services<br />
This year UHL have introduced e-Bedstate. This software system aims to:<br />
Make use of appropriate technologies, leveraging existing systems to better deliver bed status and availability information<br />
around the trust.<br />
To develop predictive elements that can assist with highlighting potential issues earlier, linking with ED and expected<br />
discharge information.<br />
To raise awareness of the importance of timely PAS updates, thus improving retrospective as well as real time analysis. This<br />
links with initiatives around electronic ordering and potentially e-prescribing both of which require up to date information about<br />
the location of a patient.<br />
To reduce the time taken to collate bed information, with the aim of reducing the frequency of or eliminating regular meetings<br />
entirely in future.<br />
To reduce the volume of email traffic associated with transferring files relating to bed meetings<br />
Further information on this can be found at Appendix 7 - Electronic bedstate at UHL<br />
• There is senior CBU manager/nurse on-call<br />
• Ensure that critical services are identified and maintained.<br />
• Ensure staff are deployed appropriately to meet service needs.<br />
• Formal communication with all staff that may be redeployed.<br />
• Contain and minimise the spread of infection and protect vulnerable groups of patients and staff.<br />
• Work effectively with partner health and other agency organisations in the community, CRAFT and Check it out<br />
• Ensure that all services are maintained and delivered safely and effectively for a long as possible.<br />
Actions<br />
• Communicate plan widely within the directorate<br />
• Develop and deliver an education programme for clinical preparedness.<br />
• Monitor bed availability<br />
• Monitor CICU/HDU bed availability<br />
• Monitor emergency activity<br />
• Monitor Planned Care ( for example chemotherapy)<br />
• Monitor Urgent work<br />
• Consider cohorting patients<br />
• Monitor cancelled non emergency/elective activity which will inform the recovery plan<br />
• Ensure that a robust recovery plan is in place.<br />
• Monitor manage staffing<br />
o Receive staff sickness/absence details<br />
o Hold directorate staff rotas & off duties<br />
o Monitor and co-ordinate staffing, including the redeployment of staff where necessary<br />
• Liaise with Infection Control<br />
• Ensure that information is clearly communicated within the directorate.<br />
• CBU bed meeting twice a day to review activity and plans and report to the Trust bed meeting<br />
• UHL conforms to the Intensive Care Society Transport standards which is guidelines for transportation of Critical care<br />
patients. This is summarised as the CENet guidance document listed in Appendix 2.<br />
• EMAS - Current arrangements are in place and operate with regard to transportation. There are no formal plans for this but it<br />
is locally agreed that at times of pressure transportation can be arranged and facilitated.<br />
Page 8
Operational readiness for Bank holiday and OOH period<br />
A multi-agency Christmas and New Year planner highlights availability for the various services over the holiday period detailing opening hours, levels of<br />
cover etc<br />
OOH provision must be maintained throughout the winter period to achieve appropriate patient flow through the system. The health community will address<br />
the Christmas and New Year Bank Holidays through agreement of minimum levels of service during this period to ensure continuity of high quality services to<br />
our patients.<br />
Access to GP<br />
When practices are closed, the OOHs service will be available for patients that will offer telephone triage, consultations and<br />
home visiting services along with the Urgent Care Centre based at the Leicester Royal Infirmary which is open 24/7, 365 days<br />
per year.<br />
Loughborough WIC, Oadby 8-8 & SSAFA 8-8 centres will also be open.<br />
Emergency Hormone Contraception will be offered by some general medical practices during their opening times. During the<br />
festive period when practices will be closed access to emergency contraception will be limited, however XX PHARMACY<br />
WILL BE OPEN ON XXXX FROM XXXXX and they will be offering EHC. The Urgent Care Centre will be open during the<br />
holiday period (24/7, 365 days per year) where EHC will be available.<br />
Primary care<br />
Access to community pharmacy<br />
Contractors will submit their proposed hours over the Christmas period by xx xx (i.e. 90 days prior to December 25th) and this<br />
will be communicated across LLR.<br />
Access to dental care<br />
The Dental Access Centre (DAC) is open during the holiday period and its opening times will be communicated to all dental<br />
contractors.<br />
The Dental OOH service operates Monday – Thursday from 18:30 pm to 08:30am pm and at weekends and bank holidays<br />
from Friday 18:30 to 08.30 Monday, with an on-call dentist available between 18.30 and 22.00 Monday to Friday, and 13.00 to<br />
18.00 at weekends and bank holidays. OOH is accessed via NHS Direct who offer triage and advice including advice available<br />
for pain control from GP OOH services and refer patients to the on call dental service.<br />
City Community Health Services<br />
OOH/UCC: Extra staffing to cover the expected demand over the Xmas period<br />
RITS: Normal working over the Xmas period<br />
DN service: Normal working over Xmas period<br />
Community matrons and specialist nurses: Normal working over Xmas period<br />
City Community beds: Normal working over Xmas period<br />
SPA: Normal working over Xmas period<br />
On call manager: As normal (usual number)<br />
On call Director: As normal – contact through on call manager<br />
CHS<br />
EMAS – 999<br />
NHS LCRCHS<br />
The out of Hours service has undertaken a full capacity and demand review to ensure clinical and non-clinical resources are<br />
deployed effectively during the winter period<br />
Revised Service Level agreement with associated pay rise has been agreed with sessional medical staff<br />
Capacity for the Christmas and New year periods will be examined carefully and resources matched to the expected demand.<br />
Escalation plans with predefined trigger points are in place for all service elements and will be managed by the clinical shift<br />
lead on duty at the Communications Centre.<br />
A Senior manager from Out of hours services is always on call.<br />
Rotas set for cover over holiday periods for all nursing and medical staff.<br />
Loughborough Walk-in Centre and all MIUs will work as usual during the Christmas Holiday period, with the exception of<br />
phlebotomy services.<br />
A review of the out of hours formulary has taken place to ensure provision of essential medication within the out of hours period<br />
in association with the on call pharmacist and 100 hour pharmacies.<br />
24 hour community nursing service in place and linked to the Out of Hours service<br />
Normal working over the xmas period<br />
EMAS – PTS<br />
UHL<br />
PTS capacity running throughout the holiday period and xxx extra crews will run for xx days from<br />
Possibility of increasing PTS capacity at times of severe surge or through the 'bank holiday' days will be considered as and<br />
when required through ECDG. Financial and operational implications have been clarified with EMAS in readiness.<br />
Clinical Business Unit Escalation plans are being developed to manage assist in managing high inflow into ED. Senior<br />
Manager and Executive Director on-call will communicate regularly with the site Bed Management teams. Rotas will be set to<br />
cover holiday periods for medical, nursing, allied professionals and non-clinical support staff. Each Clinical Business Unit will<br />
submit a Bank Holiday and Weekend plan to support capacity.<br />
Page 9
Social Services<br />
Enhanced access to social care assessment/beds in out of hours. Emergency service on DATES TO BE CONFIRMED, three<br />
member of staff per day working and they will attend the morning bed meeting and work with the most pressing case [or cases]<br />
identified.<br />
A review of capacity to speedily assess the assessment of patients with mental health problems in ED departments is to be<br />
undertaken by LPT Senior Operational Group.<br />
It is planned that all services will remain open during the winter period. Cover over the Bank Holidays will be in line with normal<br />
OOH arrangements, including a doctor in ED in line with OOH arrangements.<br />
Mental health<br />
The Trust retains comprehensive contact details, external and internal, within its Emergency Policy and Plan including for<br />
Services’ On-Call Managers. These can be contacted OOH via the LPT On-Call Director (Contactable via LPT Switchboard<br />
0116 2256000). However, the Trust will publish its’ Christmas Services working arrangements in<br />
LPT Teams have identified social workers in each locality and details of OOHs access. There are systems in place for LPT<br />
staff to contribute to discussions about packages of care. Where contact is already established for individuals out of hours<br />
and holiday contacts are communicated.<br />
Operational readiness for Seasonal Flu<br />
The LLR Cluster with NHS partners and the Local Resilience Forum have in place (and is continuing to develop) plans to minimise<br />
the impact of pandemic flu. All organisations have submitted Flu Pandemic - Business Continuity Plans, these are shown in Appendix 2. The plans are<br />
kept in a central folder.<br />
Immunisation campaign<br />
All organisations will actively encourage frontline health and social care workers to be vaccinated because they are both at an<br />
increased risk of catching swine flu and of spreading it to at-risk patients.<br />
LLR organisations will follow DH guidelines to immunise priority group, including pregnancy women, those with compromised<br />
immune systems and people over 65 in at-risk groups.<br />
Antiviral collection points<br />
Across LLR we have identified sites for antiviral collection should this be required. All pharmacies will be advised to stock up<br />
on antivaral medications if required.<br />
Flu assessment service<br />
Additional arrangements<br />
The Flu assessessment service will be encapsulated into streaming to the Urgent Care Centre, all patients preseting with flu<br />
like symptoms will be sent to the Urgent Care Centre. The UCC has turned an office at the back of the UCC into a holding<br />
area for children under 17 who present with flu like symptoms. This area is fully staff by a qualified nurse at all times, charged<br />
with taking obs etc throughout the wait.<br />
There is also a multi-agency flu meeting to deal with upsurges in levels of seasonal flu. The purpose of this meeting is to<br />
ensure that the health economy is as well prepared as possible for the Christmas and New Year period taking into account the<br />
significant levels of flu expected. This is complementary to the process already undertaken around winter pressures rather<br />
than instead of it. This applies particularly to services put into place to support discharges over the Christmas / New Year<br />
period.<br />
• Active participation and support by all Community Health Services with national winter campaigns including "AWAITING<br />
DETAILS OF NATIONAL WINTER CAMPAIGNS’.<br />
• Flu Awareness and agreed messaging is prepared and will be provided to callers during the expected flu season. All Media<br />
enquires are handled through internal Communications Department.<br />
• Joint working between the practices and community nursing teams to vaccinate housebound patients. District nursing teams<br />
to vaccinate housebound patients on their case load.<br />
• LPT Infection Control nurse is leading on current campaigns including flu vaccines and information about these and a plan is<br />
in place for all older person wards and learning disability homes<br />
• All practices are incentivised for Flu Immunisation & for Pneumococcal immunisation. This covers the provision of influenza<br />
immunisation for those aged 65 and over and 64 and under at risk groups (all those aged over 6 months in a clinical risk<br />
group) of patients registered with the Practice. This can avert the need for the patient to be hospitalised.<br />
Page 10
Norovirus<br />
The LLR Norovirus Tool kit that has been agreed by the whole health community and forms part of the supporting documents to this winter plan.<br />
Reporting of Norovirus Outbreaks as a Serious Untoward Incident (SUI)<br />
Inpatient Providers (including Acute Trusts, Mental health and Learning Disabilities, Prison Health, Community Providers)<br />
Either of the following two triggers will result in the organisation reporting and SUI<br />
1. One or more wards closed due to norovirus<br />
2. An outbreak meeting has been called.<br />
A report of the full outbreak all areas affected needs to be submitted within 20 days of the end of the outbreak.<br />
For all other providers (Nursing Homes, Residential Homes, Care Homes)<br />
The current system will remain in place where all outbreaks will be reported to the HPA. The HPA will share the information they have with all Directors of<br />
Infection Control in Primary and Secondary care, NHS East Midlands, Public Health, Microbiologist and Ambulance Trust.<br />
Adverse Weather<br />
The LLR Local Resilience Forum consists of all organisations and agencies involved with emergency response in the community. The<br />
Local Resilience aims of the group include assessing the risk of emergencies in the area, put in place business continuity management arrangements.<br />
Forum They also make arrangements to warn, inform and advise the public in the event of emergencies, severe weather etc.<br />
Primary Care<br />
During periods of severe weather if GP's/Medical Practitioners are having difficulty accessing people in need of medical attention, i.e.<br />
rural/remote areas the Local Authority co-ordinate a 4x4 Resilience Team. This is a pool of volunteers who are not a substitute for<br />
Business Continuity or normal House calls, they are for if the Emergency Services are having difficulty in accessing people<br />
UHL<br />
Social Services<br />
EMAS<br />
LLR <strong>PCT</strong> Cluster<br />
The Severe Winter Weather - UHL Response Plan (part of the supporting documents from UHL) addresses both business continuity and<br />
service response. The plan is written to mitigate risks to normal provision and to meet additional service pressures arising from snow, ice<br />
and extended periods of very low temperatures. The specific objectives of the plan seek to deliver the following:<br />
- Additional emergency service capacity, as appropriate, to manage increased trauma (RTAs / falls) and cold weather related illness<br />
- Business continuity of all vital UHL clinical services<br />
- Business continuity of elective care<br />
- Business continuity of key non-clinical support services<br />
- Co-ordinated decision making within UHL concerning contingency measures and any variations to normal service provision<br />
- Close collaboration and co-ordinated decision making with NHS and other multi-agency partners concerning contingency measures<br />
- Effective communication within and external to UHL<br />
During a pandemic situation, the Local Resilience Forum's Strategic and Tactical Groups will meet regularly and County and City Council<br />
attend these meetings. All Departments have identified their critical services that must be maintained during a Pandemic. The ‘supercritical’<br />
services (i.e. life and death) have also been identified, and in the event of very severe staff shortages the maintenance of these<br />
services would be the Council’s priority.<br />
The EMAS Winter Pressure Framework (part of the supporting documents from EMAS) covers severe weather pressures and highlights<br />
actions to be taken to minimise the impact of severe weather.This includes sickness, shortfalls in staffing, reduced manning levels, slips<br />
and falls, vehicle breakdowns, snow and icy conditions, fuel shortages and meeting response times.<br />
The LLR <strong>PCT</strong> Cluster have Business Continuity plans in place that ensure any business interruption incident from severe weather to<br />
pandemic flu can be dealt with. This is done through a tactical (corporate plan) and operational (CBU plans) approach to ensure<br />
communications, decisions and business functions are carried out during an incident.<br />
Communications Strategy<br />
Comprehensive communications plans have been developed by the LLR <strong>PCT</strong> Cluster. These plans will complement the communications plan that has been<br />
developed by the Local Resilience Forum.<br />
• All local and regional comms plans will follow similar themes to the national campaigns to ensure minimal patient confusion.<br />
• LLR <strong>PCT</strong> Cluster will lead the local communications campaign regarding winter pressures/Pandemic Flu for the health community.<br />
• Flu advice for parents and guardians is readily available for those who have children and young people returning to school/college/university. There is also<br />
information for Swine Flu available on the LLR <strong>PCT</strong> Cluster website as well.<br />
• NHS Direct has an advertising strategy in place for core services.<br />
• Leaflets with information specifically around swine flu are also available in Bengali, Gujarati, Polish, Urdu, Punjabi and Somali languages from the LLR <strong>PCT</strong><br />
Cluster website<br />
Choose Well campaign : The LLR <strong>PCT</strong> Cluster Choose Well Plan is in place and will be rolled out in partnership with stakeholder agencies. The campaign<br />
is designed to make the public aware of the various alternative healthcare options for non-emergency situations, to prevent inappropriate use of A&E. The<br />
full Communications Plan is attached as Appendix 6.<br />
Page 11
Paper 3<br />
LLR <strong>PCT</strong> Cluster Integrated Board meeting<br />
8 September 2011<br />
<strong>LEICESTER</strong>, <strong>LEICESTER</strong>SHIRE <strong>AND</strong> RUTL<strong>AND</strong> <strong>PCT</strong> <strong>CLUSTER</strong><br />
INTEGRATED BOARD MEETING<br />
Front Sheet<br />
Title of the report:<br />
Report to:<br />
Section:<br />
Date of the meeting:<br />
Report by:<br />
Sponsoring Director:<br />
Presented by:<br />
Real Accountability<br />
LLR <strong>PCT</strong> Integrated Board Meeting<br />
Public<br />
8 September<br />
Emma Cannaby<br />
Liz Rowbotham<br />
Liz Rowbotham<br />
Report supports the following corporate objective(s) 2011 – 2012:<br />
Handing over a good legacy √ Deliver the six identified transitional<br />
strands of work<br />
Manage Providers’ performance against<br />
updated health goals and identified<br />
health inequalities<br />
Deliver agreed performance targets<br />
against the six identified transformation<br />
work streams<br />
Develop and maintain an energetic<br />
stakeholder engagement programme<br />
throughout the transition<br />
√<br />
EXECUTIVE SUMMARY:<br />
The Real Accountability report contains details of 47 consultations leading to service<br />
change across Leicester Leicestershire and Rutland including work from the East<br />
Midlands Specialised Commissioning Group.<br />
The Department for Health requires <strong>PCT</strong>s to produce the report annually. The<br />
Report is to be submitted to the Strategic Health Authority mid-September.<br />
RECOMMENDATIONS:<br />
The Trust Boards are requested to:<br />
NOTE The contents of the paper and the Report<br />
AGREE to the sign off the report for submission on 14 September 2011<br />
1
Paper 3<br />
LLR <strong>PCT</strong> Cluster Integrated Board meeting<br />
8 September 2011<br />
INTRODUCTION<br />
<strong>LEICESTER</strong>, <strong>LEICESTER</strong>SHIRE <strong>AND</strong> RUTL<strong>AND</strong> <strong>PCT</strong> <strong>CLUSTER</strong><br />
INTEGRATED BOARD MEETING<br />
8 SEPTEMBER 2011<br />
Real Accountability<br />
1 Real involvement is a requirement under the statutory guidance in Section 242<br />
of the NHS Act 2006. Primary Care Trusts (<strong>PCT</strong>s), NHS trusts and Strategic<br />
Health Authorities have a statutory duty to involve patients and the public<br />
whether by consulting or providing information, or in other ways. Such<br />
involvement and consultation is required in:<br />
• planning the provision of services<br />
• the development and consideration of proposals for change in the way<br />
services are provided, and day to day processes, commissioning,<br />
prioritising and service re-design<br />
• decisions to be made affecting the operation of services<br />
2. The July 2010 White Paper Equity and excellence: Liberating the NHS said<br />
“We will put patients at the heart of the NHS, through an information revolution<br />
and greater choice and control.”<br />
• shared decision-making will become the norm: for patients this must mean<br />
“no decision about me without me”<br />
• we will also look at existing mechanisms, including relevant legislation, to<br />
ensure that public engagement is fully effective in future, and that services<br />
meet the needs of neighbourhoods<br />
• we will proactively seek and build continuous and meaningful engagement<br />
with the public and patients, to shape services and improve health<br />
• we will lead continuous and meaningful engagement with clinicians to<br />
inform strategy, and drive quality, service design and resource utilisation.<br />
3. In April 2010 the Department of Health published new guidance for the NHS,<br />
which asked local <strong>PCT</strong>s to produce an annual report about how they have<br />
acted on feedback from patients and the public, and to highlight forthcoming<br />
consultations. This requirement is called ‘Real Accountability’. The report must<br />
also include influences that have been made as a result of the consultation.<br />
4. This is the second report covering all consultations from April 2010 to March<br />
2011. It is a joint report for both NHS Leicester City and NHS Leicestershire<br />
County and Rutland, which began working collaboratively as a single <strong>PCT</strong><br />
cluster in the autumn of 2010. We have already begun transferring increased<br />
responsibility to the three clinical commissioning groups (CCGs) for our area –<br />
Leicester City CCG, West Leicestershire CCG and East Leicestershire and<br />
Rutland CCG, which are due to take full legal responsibility for most local<br />
commissioning functions by April 2013, subject to Parliamentary approval of<br />
the Health and Social Care Bill and the successful authorisation by the<br />
2
CONTEXT<br />
Paper 3<br />
LLR <strong>PCT</strong> Cluster Integrated Board meeting<br />
8 September 2011<br />
Department of Health for these CCGs to undertake their relevant<br />
commissioning duties.<br />
5. NHS Leicester City, Leicestershire County and Rutland along with all other<br />
NHS trusts are required to proactively engage with all stakeholders in all<br />
groups: staff, public, patients, partner organisations, voluntary, independent<br />
and private sector to collect and collate their feedback on consultations. This<br />
is not only a legal duty, but it is also best practice to feedback outcomes form<br />
the consultations locally. This is to be fed into the Real Accountability report<br />
once a year. This will further underpin the vision of the organisation to reduce<br />
inequalities and to represent, support and enable the population of Leicester<br />
Leicestershire and Rutland to have their say on such major changes.<br />
6. More and more people across the country should feel better informed and<br />
encouraged to have a say about what really matters to them about their area’s<br />
healthcare services. NHS Leicester City and NHS Leicestershire County and<br />
Rutland have been making great strides in involving local residents in the<br />
development of these services. Our goal is to ensure that Leicester residents<br />
are among the most informed and empowered in the country. It is also our<br />
ambition that we are as demographically representative of the city and two<br />
counties as is realistically possible to ensure that typically hard-to-reach and<br />
seldom heard groups also have appropriate opportunity to have their say. The<br />
two <strong>PCT</strong>s’ new Cluster Board and the area’s three CCGs are using the<br />
feedback and insight into patients’ needs and wishes in order to inform<br />
improvements in health services.<br />
7. In future we need to illustrate best practice engagement and lead the way<br />
ready for the time when legal responsibility for engaging with the population of<br />
Leicester Leicestershire and Rutland transfers to our CCGs. There are various<br />
high quality patient and public groups available, who have been or can be<br />
contacted to feed into future engagements. NHS Leicester City and NHS<br />
Leicestershire County and Rutland are looking into the facilitation of the<br />
transition of engagement from local trusts to the CCGs to empower GPs and<br />
their clinical colleagues to meaningfully engage with their patients in future.<br />
RECOMMENDATIONS<br />
The Trust Boards are requested to:<br />
NOTE: The contents of the paper and the Report<br />
AGREE to the sign off the report for submission mid-September 2011<br />
APPENDICES:<br />
Appendix 1: Real Accountability 2010 - 2011<br />
3
Consultations and public engagement<br />
projects to inform decisions on<br />
commissioning healthcare
Real Accountability Annual Report 2010-2011<br />
Introduction<br />
Real involvement is a requirement under the statutory guidance in Section 242 of the<br />
NHS Act 2006. Primary Care Trusts (<strong>PCT</strong>s), NHS trusts and Strategic Health<br />
Authorities have a statutory duty to involve patients and the public whether by<br />
consulting or providing information, or in other ways. Such involvement and<br />
consultation is required in:<br />
• planning the provision of services<br />
• the development and consideration of proposals for change in the way<br />
services are provided, and day to day processes, commissioning, prioritising<br />
and service re-design<br />
• decisions to be made affecting the operation of services<br />
The July 2010 White Paper Equity and excellence: Liberating the NHS said “We will<br />
put patients at the heart of the NHS, through an information revolution and greater<br />
choice and control.” The Paper set out the following:<br />
• shared decision-making will become the norm: for patients this must mean “no<br />
decision about me without me”<br />
• we will also look at existing mechanisms, including relevant legislation, to<br />
ensure that public engagement is fully effective in future, and that services<br />
meet the needs of neighbourhoods<br />
• we will proactively seek and build continuous and meaningful engagement<br />
with the public and patients, to shape services and improve health<br />
• we will lead continuous and meaningful engagement with clinicians to inform<br />
strategy, and drive quality, service design and resource utilisation.<br />
In April 2010 the Department of Health published new guidance for the NHS, which<br />
asked local <strong>PCT</strong>s to produce an annual report about how they have acted on<br />
feedback from patients and the public, and to highlight forthcoming consultations.<br />
This requirement is called ‘Real Accountability’. The report must also include<br />
influences that have been made as a result of the consultation.<br />
This is the second report covering all consultations from April 2010 to March 2011. It<br />
is a joint report for both NHS Leicester City and NHS Leicestershire County and<br />
Rutland, which began working collaboratively as a single <strong>PCT</strong> cluster in the autumn<br />
of 2010. The Cluster has already begun transferring increased responsibility to the<br />
three clinical commissioning groups (CCGs) for our area – Leicester City CCG, West<br />
Leicestershire CCG and east Leicestershire and Rutland CCG. The groups are due<br />
to take full legal responsibility for most local commissioning functions by April 2013,<br />
subject to Parliamentary approval of the Health and Social Care Bill and the<br />
successful authorisation by the Department of Health for these CCGs to undertake<br />
their relevant commissioning duties.<br />
3
Foreword<br />
The people of Leicester, Leicestershire and Rutland have every right to make their<br />
voices heard on the healthcare services which their NHS commissions for them.<br />
Good engagement must be integral to all commissioning decisions. It is not only a<br />
legal duty, but it also makes good sense – socially, financially, clinically and<br />
strategically - and no business case for a new or modified service will succeed<br />
without it.<br />
The Secretary of State for Health presented to Parliament the White Paper Equity<br />
and excellence: Liberating the NHS in July 2010. It includes the policy to phase out<br />
primary care trusts and create a lead role for clinical commissioning groups in future.<br />
It also gives weight to the principle of “fuller engagement with primary care<br />
professionals, patients and the public” and sets out “to ensure that public<br />
engagement is fully effective in future, and that services meet the needs of the local<br />
neighbourhoods”.<br />
The engagement expertise we have developed in Leicester, Leicestershire and<br />
Rutland will prove a valuable asset to future local commissioning bodies. So in the<br />
interim we need to maintain the standard we have set, as an example of best<br />
practice for those who follow us. The practice based commissioning groups, who<br />
played such a vital role on our former Commissioning Executive, provided an ideal<br />
forum for this expertise to be shared and its legacy continues in its successor body,<br />
the clinical Collaborative, and during the ‘shadow clinical commissioning group’<br />
phase of the ongoing NHS reforms.<br />
Our clinicians know that Leicester, Leicestershire and Rutland is a complex area.<br />
What suits one area may not suit another. There is no longer a place for a ‘one size<br />
fits all’, or ‘top-down’ mentality when it comes to designing clinical pathways and<br />
other areas of our healthcare services. If we cannot make the service fit the local<br />
need – clinically and culturally – we are not doing our job to the standards required<br />
by the principles of ‘equity and excellence’ set out by the government.<br />
Engagement is not only part of the service development and procurement process,<br />
but also an essential part of the evaluation process. The public will have a major say<br />
in the ‘last word’ on whether our commissioning decisions worked. As the Secretary<br />
of State for Health, Andrew Lansley, has said on behalf of patients: “There should be<br />
no decision about me without me”.<br />
Catherine Griffiths<br />
Chief Executive<br />
4
Contents<br />
Page<br />
Introduction 3<br />
Foreword 4<br />
Background 7<br />
Part I: Joint partnership engagements 8<br />
Adult mental health strategy 9<br />
CFS (Chronic Fatigue Syndrome) and ME (Myalgic Encephalomyelitis) 12<br />
Children and Adolescent Mental Health Service strategy 13<br />
Children and young persons needs assessment 16<br />
Community consultation on equality outcome objectives 18<br />
Community development worker project 19<br />
Drug and alcohol strategy 22<br />
End of Life Care 25<br />
Greater Choice and Control and the Information Revolution White Paper 28<br />
Maternity and neonatal services review 30<br />
Maternity Service Liaison – designing a 12-month rolling programme 32<br />
Naming the IAPT service 33<br />
Older Persons Month 35<br />
Pharmaceutical Needs Assessment 36<br />
Public Health White Paper 39<br />
Quality, Innovation, Productivity and Prevention (QIPP) 41<br />
Quality Innovation, Productivity and Prevention: Strategic Operating Plan 42<br />
Quality Innovation, Productivity and Prevention (QIPP) event 3: Right Care –<br />
Planned Care 44<br />
Transforming community services 46<br />
The White Paper Equity and excellence: liberating the NHS 47<br />
Part 2: Leicester City engagements 49<br />
Beaumont Leys Surgery – procurement training 50<br />
Belgrave Medical Centre closure and patient registration 51<br />
“Call time on drink” campaign 53<br />
Medicines Use Review survey 54<br />
New arrivals engagement 55<br />
Out of Hours Service 57<br />
Patient Participation Group event 59<br />
Sexual health website 60<br />
Part 3: Leicestershire County and Rutland engagements 61<br />
Bowel cancer and bowel cancer screening awareness 62<br />
Dental access 63<br />
5
Contents<br />
Page<br />
Health care for older people, patients and carers 64<br />
Loughborough University health and wellbeing event 65<br />
Membership Consultation 66<br />
Pacesetters Bowel Cancer Screening Awareness Project 68<br />
Patient experience 71<br />
Perinatal psychosis 72<br />
Public Consultation on the proposed closing of Ketton and Gretton branch surgeries<br />
by Uppingham General Practice. 74<br />
Smoking, diabetes and eyes event 75<br />
Women’s Cancer Event 76<br />
Part 4: East Midlands Specialised Commissioning Group (EMSCG)<br />
engagements 77<br />
Introduction 78<br />
Forward 79<br />
Teenage and Young Adults Cancer (TYA) 80<br />
East Midlands Renal Network (EMRN) 81<br />
Midland Burn Care Network (MBCN) 82<br />
Safe and Sustainable - National Paediatric Congenital Heart Surgery Review 83<br />
East Midlands Haemophilia Management Group 84<br />
National Commissioning documents for Haemoglobinopathy 85<br />
Involvement of regional Expert Patient Committees in the commissioning and<br />
development of Specialised Perinatal Mental Health Services in the East Midlands 86<br />
Policy Development 88<br />
EMSCG Commissioning Policy for the use of Pre Implantation Genetic Diagnosis<br />
(PGD) (version 2). 88<br />
How to contact us 92<br />
Do you need help understanding this report? 94<br />
6
Background<br />
NHS Leicester City, Leicestershire County and Rutland along with all other NHS<br />
trusts are required to proactively engage with all stakeholders in all groups: staff,<br />
public, patients, partner organisations, voluntary, independent and private sector to<br />
collect and collate their feedback on consultations. This is not only a legal duty, but it<br />
is also best practice to feedback outcomes form the consultations locally. This is to<br />
be fed into the Real Accountability report once a year. This will further underpin the<br />
vision of the organisation to reduce inequalities and to represent, support and enable<br />
the population of Leicester Leicestershire and Rutland to have their say on such<br />
major changes.<br />
More and more people across the country should feel better informed and<br />
encouraged to have a say about what really matters to them about their area’s<br />
healthcare services. NHS Leicester City and NHS Leicestershire County and Rutland<br />
have been making great strides in involving local residents in the development of<br />
these services. Our goal is to ensure that Leicester residents are among the most<br />
informed and empowered in the country. It is also our ambition that we are as<br />
demographically representative of the city and two counties as is realistically<br />
possible to ensure that typically hard-to-reach and seldom heard groups also have<br />
appropriate opportunity to have their say. The two <strong>PCT</strong>s’ new Cluster Board and the<br />
area’s three CCGs are using the feedback and insight into patients’ needs and<br />
wishes in order to inform improvements in health services.<br />
In future we need to illustrate best practice engagement and lead the way ready for<br />
the time when legal responsibility for engaging with the population of Leicester<br />
Leicestershire and Rutland transfers to our CCGs. There are various high quality<br />
patient and public groups available, who have been or can be contacted to feed into<br />
future engagements. NHS Leicester City and NHS Leicestershire County and<br />
Rutland are looking into the facilitation of the transition of engagement from local<br />
trusts to the CCGs to empower GPs and their clinical colleagues to meaningfully<br />
engage with their patients in future.<br />
7
Part I: Joint partnership engagements<br />
8
Adult mental health strategy<br />
What was the issue?<br />
The Joint Commissioning Strategy for Mental Health sets out the commissioning<br />
intentions of NHS Leicester City and Leicester City Council in respect of services for<br />
people with mental health over the next 18 months. As the key partners to this plan<br />
NHS Leicester City is responsible for commissioning health services locally and<br />
Leicester City Council is responsible for commissioning social care services. In the<br />
summer of 2010 consultation took place about the commissioning priorities with<br />
service users and family carers, facilitated through voluntary organisations and<br />
existing forums.<br />
Who was consulted?<br />
The strategy has been developed through the NHS Leicester City Mental Health<br />
Programme Board, which brought together a range of stakeholders who are<br />
interested in mental health and wellbeing. The role of the Programme Board was to<br />
develop the strategic direction for commissioning and delivery of mental health<br />
services in Leicester and monitor its implementation. In drawing up this strategy we<br />
took into account the needs of service users, expert and clinical knowledge,<br />
evidence of what works and most importantly how the people who use services<br />
would like to see them developed. The stakeholders consulted included:<br />
• staff and clinicians working for Leicester City Council and the Leicestershire<br />
Partnership Trust<br />
• services users and carers<br />
• residential Care providers within Leicester City<br />
• other independent Providers of mental health services within Leicester City<br />
• GPs and primary care staff<br />
• voluntary organisations<br />
Additional focus groups were also held with the South Asian community, a Bengali<br />
women’s group and the Somalian community.<br />
The focus groups were facilitated by the following local voluntary sector<br />
organisations and they also supported the completion of questionnaires:<br />
• LAMP (Leicestershire Action for Mental Health)<br />
• Adhar (meaning ‘support’ – for adults with mental health problems and their<br />
carers)<br />
• Network for Change<br />
• Akwaaba Ayeh (advocacy and advice on mental health for BME communities)<br />
• Community development workers<br />
What information was given?<br />
A covering letter was sent to stakeholders via email and through the post which<br />
outlined the intentions for the Joint Commissioning Strategy for Mental Health.<br />
Information with a link to the questionnaire was also put on the <strong>PCT</strong> and local<br />
authority websites including links on the voluntary sector organisations’ website. A<br />
presentation was given in the focus groups meetings explaining the need for a new<br />
strategy highlighting the identified priorities for discussion. In all engagement it was<br />
explained that the feedback would be used to inform the development of the<br />
strategy.<br />
9
What were people asked to comment on?<br />
Consultation about the priorities, their current experiences and the type of services<br />
they would like in the future took place over August and September 2010. An online<br />
survey was developed including the provision of paper based surveys to gather<br />
people’s views. Furthermore, a series of focus groups took place across the city. The<br />
focus groups were held with groups with which the organisations do not often<br />
engage. The service users and carers were given the draft priorities and asked to<br />
state whether they agreed or disagreed. They were then asked to rate the<br />
importance of each priority. Questions were asked about the different types of<br />
support on offer with recommendations for improvements.<br />
Summary of feedback<br />
Overall there were over 240 responses to the survey. A total of 79% of the<br />
respondents were mental health service users and 21% were carers.<br />
In total 65% of the respondents were female and 35% were male. The ethnic<br />
breakdown of the respondents is as follows:<br />
• Asian/Asian British – 56%<br />
• Black/Black British – 8%<br />
• Chinese – 0%<br />
• mixed/dual heritage – 1%<br />
• White – 23%<br />
• other Ethnic Group 4%<br />
• non-respondents 8%<br />
When analysing the ethnicity data it is pleasing that we had such a high percentage<br />
response from the Black Minority Ethnic groups. This is vital in a diverse city like<br />
Leicester.<br />
Just fewer than 54% of the respondents considered themselves to have a disability.<br />
Over 96% of the respondents considered their mental wellbeing to be very important.<br />
The respondents considered that the following were very important to their<br />
wellbeing:<br />
• physical Health – 86%<br />
• housing – 86%<br />
• financial position – 76%<br />
• local environment – 73%<br />
• employment – 59%<br />
Over 86% of the respondents felt that access to mental health support was<br />
important. When asked what type/s of services/support people accessed when they<br />
or a family member/friend needed support; we received the following responses:<br />
• GP – 70%<br />
• family members – 54%<br />
• psychiatrists – 41%<br />
• friends – 40%<br />
• counselling services – 28%<br />
10
A total of 39% of the respondents indicated that they/friend/family member were an<br />
inpatient in a mental health hospital. Only 4% did not access any support for their<br />
mental health issue/s.<br />
Over 83% of the respondents felt it was very important to have mental health<br />
services that are local i.e. within 3-5 miles of where they live. Over 89% said that<br />
services need to be easily accessible i.e. convenient opening hours, parking, meets<br />
their specific cultural and religious requirements, good disability access and public<br />
transport links.<br />
People were asked what types of services would have met/would meet their or their<br />
family member/friend’s needs. The following types of support were highlighted by the<br />
respondents:<br />
• group support – 64%<br />
• drop-in services – 56%<br />
• 1:1 support – 49%<br />
• community based services – 49%<br />
• peer groups – 39%<br />
• support into education – 24%<br />
Only 42% wanted hospital based services.<br />
Just over 68% felt it was important to be able to choose the services or packages of<br />
support would help maintain their mental wellbeing if they were given the money to<br />
do so.<br />
Decisions made<br />
The feedback supported the identification of the joint commissioning priorities and<br />
the development of the strategy and the implementation plans. These were shared<br />
back with service users, carers, stakeholders and partners.<br />
11
CFS (Chronic Fatigue Syndrome) and ME (Myalgic<br />
Encephalomyelitis)<br />
What was the issue?<br />
There are many different possible causes for these conditions, which are better<br />
known by their abbreviated title CFS/ME. Potential causes include neurological,<br />
endocrinal, immunological, genetic, psychiatric and infection-based factors. All have<br />
been investigated, but the diverse nature of the symptoms cannot yet be fully<br />
explained.<br />
The World Health Organisation (WHO) classifies CFS/ME as a neurological illness.<br />
Leicestershire’s CFS/ME services are currently provided by Leicestershire<br />
Partnership Trust (LPT) and predominantly cover the psychological aspects of<br />
care. Following the NICE guidelines (2007), nationally the majority of CFS/ME<br />
services now sit in acute care services, mainly within neurology. We needed to know<br />
if we were providing the most clinically appropriate services for people with this<br />
condition.<br />
Who was consulted?<br />
In 2010/11 a local task and finish group engaged with ME Positive (the local user<br />
group) and collated feedback on the current service and views on what a future<br />
service should look like.<br />
What information was given?<br />
The current service based at LPT was discussed with the group, who were already<br />
familiar with many aspects of it, and the service specification documentation and<br />
NICE guidelines were scrutinised.<br />
What were people asked to comment on?<br />
ME Positive, a patient representative group were asked to comment on the current<br />
service specification, the NICE guidelines and draft a proposed new pathway for<br />
CFS/ME sufferers.<br />
Summary of feedback<br />
The main recommendations from this engagement were:<br />
• more GP engagement on CFS/ME to ensure better diagnosis within primary<br />
care<br />
• a neurological rather than a psychological pathway for CFS/ME patients<br />
• improved availability of alternative therapies<br />
• a personalised approach to the management of the condition and symptoms.<br />
A proposed pathway was also developed by the group with recommendations for a<br />
redesigned service. The current service specification was examined and suggestions<br />
were made based on direct patient experiences.<br />
Decisions made<br />
Discussions are currently taking place about the service review and proposed<br />
pathway redesign. The next step in this process includes wider engagement with<br />
clinicians, stakeholders and other user groups.<br />
12
Children and Adolescent Mental Health Service strategy<br />
What was the issue?<br />
NHS Leicester City and NHS Leicestershire County and Rutland reviewed the<br />
Children and Adolescent Mental Health Service (CAMHS) for the period of 2011 to<br />
2014. This is to provide clear, timely and honest information about the direction of<br />
travel for CAMHS in Leicester, Leicestershire and Rutland. It was not possible for<br />
this consultation to be a simple strategy review or questionnaire, as this is a complex<br />
part of the health service.<br />
Not only does the CAMHS strategy need to reflect the needs of a diverse<br />
community, it also needs to prioritise actions and service requirements to suit the<br />
needs of the patients, who are young people, and be sensitive to their needs. As the<br />
patients have mental health problems, NHS Leicester City led the consultation to<br />
identify all stakeholders who needed to participate in the service redesign. The<br />
communication and feedback channels had been designed to enable patients to<br />
express their views without bias.<br />
Who was consulted?<br />
There were several groups of people involved in the project. The approach taken led<br />
to several groups being consulted. There were several media releases promoting<br />
feedback throughout September 2010 to February 2011. There was a publically<br />
available questionnaire for patients, public, children and young people, parents and<br />
carers, service staff and partners of the CAMHS service.<br />
There was an easy read questionnaire with instructions of how to help the child or<br />
young person fill in the questionnaire. There was a questionnaire written by specialist<br />
nurses, with supporting pictures, to enable children with mental health and learning<br />
disabilities to be able to contribute to the consultation.<br />
There were several stakeholders meeting from November 2010 to February 2011 to<br />
collect stakeholder and partner organisation feedback on the strategy. There were<br />
also some focus groups with children and young people with an interest in the<br />
CAMHS service who took part in the consultation.<br />
What information was given?<br />
Existing information was used to design the questionnaires and surveys. Local<br />
partner organisations shared feedback from their patients to help design which<br />
issues needed to be considered as priorities for the period of 2011 to 2014.<br />
Alongside this, there was easy read information describing the purpose of the<br />
consultation and why people need to feedback honestly.<br />
The pathway and service delivery was also described in basic English along with a<br />
visual interpretation of the CAMHS system. This was done using a hand-drawn<br />
graphic illustration of the process (please see image): -<br />
13
What were people asked to comment on?<br />
The public, children and young people, carers, parents, staff and partners were all<br />
asked to comment on the principle and priorities, which had been selected from<br />
previous feedback. This was done by selecting on a rating scale of how important<br />
this would be to them. Alongside this we asked for their reasons. These included<br />
which conditions or mental health categories they felt needed prioritising for<br />
Leicester, Leicestershire and Rutland.<br />
In the focus groups, people were shown the pathway diagram and asked to feedback<br />
on experience and potential improvements for each stage and the transfers between<br />
stages, including communication.<br />
Once the draft strategy was completed, the draft document was consulted with the<br />
stakeholders to make it an appropriate document to be used by partner<br />
organisations across the city.<br />
Summary of feedback<br />
Some of the comments leading to the redesign included:<br />
• there is a lot of untreated childhood anxiety<br />
• families need to be more involved in children’s and young people’s treatment<br />
• service delivery locations need to be child friendly in a comfortable<br />
environment<br />
• children and young people should get a say in the treatment they receive.<br />
The stakeholders wanted the assurance that plans developed were fed back to<br />
interested stakeholders and people who participated, complying with the standards<br />
of engagement for all organisations involved.<br />
Decisions made<br />
Using this feedback, the CAMHS service is working on:<br />
• maintaining and developing mental health promotion and prevention to<br />
increase resilience and reduce risks<br />
• ensuring that good links with adult services are maintained is relation to<br />
transition from children to adult services and taking the ‘whole family<br />
approach’ work forward<br />
• making all services child and young person friendly<br />
14
• continually getting feedback from patients, carers and partner organisations<br />
about the service they are providing, and acting upon realistic suggestions or<br />
improvements.<br />
15
Children and young person’s needs assessment<br />
What was the issue?<br />
This is a needs assessment for Leicester City, which was aimed to outline the<br />
priorities for services in different areas. It was designed jointly between NHS<br />
Leicester City, Leicester City Council, Voluntary Action Leicester, Connexions and<br />
associated partners. Engaging with children and young people is one of the least<br />
practiced and they are nationally seen as a ‘seldom heard group’.<br />
This needs assessment identified groups in particular need:<br />
• disabled children<br />
• children in care<br />
• young offenders<br />
• teenage parents<br />
• young people not in education employment and training<br />
• young carers<br />
• children and young people with parents who use drugs and alcohol<br />
Who was consulted?<br />
The Children Trust was the vehicle for consultation. Therefore, representatives from<br />
this group was asked to use the presentation and executive summary to deliver the<br />
key findings from the needs assessment and then feedback into the process. A wide<br />
range of partners were consulted, many of whom did not provide written feedback<br />
however, written feedback was received from:<br />
• Leicester City Children’s Trust and associated thematic groups<br />
• Investing in Children’s Priority Board Leicester City Council<br />
• Parents of young offenders<br />
• Parenting strategy Advisory Board<br />
• CAMHS partnership<br />
• NHS Leicester City Childrens Commissioner and Safeguarding lead<br />
• Drug and alcohol commissioning manager<br />
• Leicester city PE and school sports Board<br />
• Healthy weight strategic group<br />
• 12 Neighbourhood Advisory Boards 0-12 and 13-19<br />
• Early Prevention Services Strategy team Leicester City Council<br />
• Voluntary and community sector - feedback from 21 organisations.<br />
What information was given?<br />
Stakeholders and members of the public were informed of the discrepancies of the<br />
quality of life in different areas of the city. A presentation was used to give examples<br />
of a child growing up in two areas in the city and how different their expected<br />
outcomes were due to the area they lived in. Information included health outcomes,<br />
educational outcomes, and other life indicators.<br />
There was also a needs assessment summary which was shared for comment<br />
including the priorities the city would have to improve the health and quality of life<br />
outcomes of areas that are lower than the national standards.<br />
16
What were people asked to comment on?<br />
People were asked if the summary of the needs assessment was accurate in the<br />
context of their knowledge of the city and the areas within the city, and, if not, why.<br />
They were then asked if there was any significant information in the needs<br />
assessment that had been missed out, that they felt needed to be included. After the<br />
presentation these questions were posed by the presenter and feedback collated<br />
and returned to public health.<br />
Summary of feedback<br />
The life course stories of two children in different parts of the city resonated with<br />
those that fed back on the work. A range of feedback received including the<br />
identification of some groups that had been missed in the earlier iterations and these<br />
have now been included, along with more recent data that was included in the final<br />
version.<br />
Decisions made<br />
The revised Leicester City Children and Young People’s Plan has now been<br />
published and the focus on outcomes reflects the needs of the children and young<br />
people in the city. City youth advisors have commented and agreed on the plan.<br />
17
Community consultation on equality outcome objectives<br />
What was the issue?<br />
NHS Leicester City, and NHS Leicestershire County and Rutland and Leicestershire<br />
Partnership NHS Trust needed assistance to identify and meet its Public Sector<br />
Equality Duty (PSED) under the Equality Act 2010. They needed to identify and<br />
agree with the NHS workforce and community stakeholders a set of equality<br />
outcome objectives and priorities for 2011-12.<br />
Who was consulted?<br />
Internally we consulted staff members throughout NHS Leicester City, NHS<br />
Leicestershire County and Rutland, University Hospitals of Leicester NHS Trust,<br />
Leicestershire Partnership NHS Trust. Externally; service users, voluntary and<br />
community groups including service level agreement organisations reflecting<br />
ethnicity, disability and sexual orientation were consulted. Also involved were<br />
Leicestershire Working Together Forum which represented all protected<br />
characteristics across Leicestershire.<br />
What information was given?<br />
Information was given on the new integrated equality service for NHS Leicester City,<br />
Leicestershire County and Rutland, along with an overview of Equality Act 2010<br />
including:<br />
• public sector equality duty – due regard<br />
• analysis of equality (equality impact assessment)<br />
• equality delivery system (the Department of Health Framework for Equality,<br />
Diversity and Human Rights in all we do)<br />
• organisations to assess their equality performance against 12 outcomes<br />
grouped into four objectives.<br />
Participants were also given a detailed overview including evidence to support each<br />
proposed equality outcome objective and enabler.<br />
What were people asked to comment on?<br />
Internal and external stakeholders were asked to comment and provide preferences<br />
on a set of draft equality outcome objectives and priorities. This included an<br />
opportunity to vote on each objective and outcome.<br />
Summary of feedback<br />
Feedback included comments that could be grouped under the following themes:<br />
• focus on outcomes not process<br />
• be clear in communications<br />
• make more of what we have<br />
• don’t lose quality and focus in the drive for greater efficiency<br />
• keep it real<br />
• involve local people and groups<br />
• be transparent.<br />
Decisions made<br />
The project planning and implementation is still ongoing at the time of going to print.<br />
18
Community development worker project<br />
What was the issue?<br />
The aim was to review the effectiveness of a three-year project to improve referrals<br />
within Black and Minority Ethnic (BME) communities to access mental health<br />
services in Leicester City, Leicestershire and Rutland. It had been set up as part of a<br />
national Department of Health programme called Delivering Race Equality (in mental<br />
health).<br />
The ethnicity of the Leicester City, Leicestershire and Rutland population is diverse.<br />
In Leicestershire and Rutland nearly 95% of the population are from white ethnic<br />
groups. The main minority ethnic group is south Asian with large populations in<br />
Loughborough and Oadby and Wigston.<br />
Approximately 40% of Leicester’s population has an ethnic minority background and<br />
evidence suggests that it is becoming more diverse. Statistics show that 28% of the<br />
Leicester population are Gujarati Indians, originally either from East Africa, especially<br />
Uganda and Kenya, or from Gujarat. Other smaller communities in the city include<br />
the African Caribbean and Somali communities, at around 3% each, as well as<br />
people from Pakistan, Bangladesh, along with other African or Chinese communities.<br />
The age profile of these population groups is younger than average with 54% of<br />
Leicester’s school pupils from a minority ethnic background.<br />
The project’s host organisation was Age Concern, who had employed a team of<br />
CDWs to run the project. The project lead wanted to review the service and identify if<br />
there were any gaps which were not covered by other existing services in Leicester<br />
City, Leicestershire County and Rutland. This was important as not only are there<br />
various communication barriers, but there can also be a lack of knowledge of<br />
services available and unwitting negative stereotyping within the service. Therefore a<br />
consultation was run from October to November to gain feedback on the knowledge<br />
and attitudes of the service provided, and gaps that would be left if there was to be<br />
no replacement service, following the end of the existing project contract<br />
arrangement in March 2011.<br />
Who was consulted?<br />
There were three separate consultations. The host, Age Concern, and relevant staff<br />
were consulted about services they had provided and referral success rate. They<br />
were also asked for details of activities and successful projects during the three-year<br />
project.<br />
The partner organisations who worked closely with the CDW project were also<br />
consulted. This was done by an online and paper questionnaire going to each<br />
member of staff working with the CDW project. Finally service users were also asked<br />
to complete a questionnaire either online or a paper copy.<br />
What information was given?<br />
NHS Leicester City, and NHS Leicestershire County and Rutland shared information<br />
and agreed that an evaluation of the service was needed. The overall objective of<br />
the evaluation was to assess the extent to which the CDW project had successfully<br />
contributed to the delivery of the DH’s wider agenda of achieving equality and<br />
tackling discrimination in mental health services.<br />
19
The evaluation reviewed the service against the four main roles as set out in the<br />
policy guidance and the output specification, as set out by the two primary care<br />
trusts as commissioning bodies. It also aimed to assess the value-for-money<br />
element within the current climate of financial constraints. Finally, the evaluation<br />
aimed to identify the ways in which the agenda for tackling discrimination and<br />
achieving equality in mental health services might be sustained.<br />
What were people asked to comment on?<br />
To assess the impact of the CDW project, all people consulted were asked for<br />
feedback on the extent to which the following project aims had been achieved in the<br />
past three years:<br />
To act as a change agent by:<br />
• raising levels of understanding of the mental health needs of BME population<br />
groups<br />
• identifying gaps in services<br />
• improving communication between BME community services and statutory<br />
services.<br />
To facilitate access to mental health services by:<br />
• identifying the barriers which prevent BME communities from accessing timely<br />
and effective mental health services<br />
• helping to overcome those barriers.<br />
To develop services by:<br />
• advising on training and education of staff<br />
• highlighting the importance of cultural awareness in service systems and<br />
practice<br />
• developing joint working between statutory and community services.<br />
To build community capacity by:<br />
• helping the BME population group to develop grassroots solutions to mental<br />
health issues<br />
• supporting the development of BME community resources for mental health<br />
• helping local groups and networks to develop the relationships and know-how<br />
which will enable them to make their views known and play an effective role in<br />
local partnerships for mental health.<br />
Summary of feedback<br />
Overall, the CDWs were seen as having been fairly successful in engaging with<br />
community organisations and undertaking specific programmes which have<br />
contributed to the raising of awareness of mental health issues within the BME<br />
community. Much of the work by the CDW team has included developing and<br />
managing relationships with key stakeholders, partners and services, aimed at<br />
raising the profile of the CDWs and the Delivering Race Equality (in mental health)<br />
programme.<br />
It has been through the development of such links that the CDWs have been able to<br />
gather intelligence about gaps in service provision for BME communities and begin<br />
to devise and implement some solutions. Feedback showed that the CDWs had<br />
undertaken awareness raising sessions and had made contact with a number of<br />
voluntary and statutory organisations, users and carers to promote further<br />
awareness.<br />
20
The project has been less successful in demonstrating the outcomes of the initiatives<br />
and their sustainability. There were areas where there appeared to be a lack of<br />
continuity and evidence of CDW work which demonstrated the need for capacity<br />
building.<br />
The feedback also suggested that the CDWs were strong in identifying gaps in<br />
services, but had not been sufficiently innovative, had missed opportunities for<br />
greater integration and had not become sufficiently effective agents of change.<br />
Decisions made<br />
It was decided that the existing contract could be terminated at the end of the third<br />
year, March 2011. There would still be a service gap for the African Caribbean<br />
community, therefore a CDW would need to be commissioned specifically for this<br />
community.<br />
21
Drug and alcohol strategy<br />
What was the issue?<br />
The National Drug Strategy (NDS) 2008-2018 emphasizes the need to focus more<br />
on families, addressing the needs of parents and children as individuals, as well as<br />
working with whole families to prevent drug use, reduce risk and get people into<br />
treatment. The NDS also clearly states that we need to deliver new approaches to<br />
drug treatment and social re-integration. The Alcohol Harm Reduction Strategy for<br />
England: Safe. Sensible, Social, (2007), outlines the next steps in the alcohol<br />
strategy. Priorities include engaging harmful and dependent drinkers with prevention<br />
and treatment services, tackling alcohol-fuelled crime and disorder; and promoting<br />
sensible drinking. Services were being re-designed to reflect local and diverse<br />
needs. We were also seeking to test the market in line with Leicester City Council’s<br />
procurement policy and EU (European Union) procurement law.<br />
The Safer Leicester Partnership (SLP), Drug and Alcohol Action Team (DAAT) are<br />
responsible for the commissioning of adult and young people’s substance misuse<br />
treatment services. NHS Leicester City is responsible for commissioning adult<br />
alcohol prevention and treatment services. SLP DAAT and the NHS Leicester City<br />
are in the process of undertaking a re-commissioning (and service redesign) of their<br />
adult treatment service with the aim of improving access to and quality of service<br />
provision and to develop an integrated drug and alcohol treatment model.<br />
Who was consulted?<br />
Questionnaires were available on-line, and a further 2000 paper questionnaires were<br />
disseminated across the city via council run locations and drug and alcohol treatment<br />
providers.<br />
Stakeholders, including the general public were made aware of the consultation<br />
process, and how to respond through a variety of promotional means, including<br />
email alerts, web site signposting, and use of the media. Specifically this included<br />
adverts, posters, radio interviews and local publications across the city, in particular,<br />
faith, language and cultural based publications (Leicester Link, Ramadan<br />
Publications, Kohinoor Newsletter, Clasp Newsletter, Service Users News (SUN),<br />
Helping Hands Newsletter, NHS customer and patient involvement newsletter.<br />
Participants were given the opportunity to give their views via the website, or via<br />
paper and electronic questionnaires. Translated questionnaires, special needs<br />
versions (large print / Braille) and translators were available on request.<br />
In addition to the completion of questionnaires, a community engagement approach<br />
was adopted to target key groups to provide their views. Community and<br />
neighbourhood support groups for feedback were organised to support the inclusion<br />
and involvement of vulnerable and underrepresented people and communities.<br />
Small informal discussion groups, with target groups were undertaken, alongside<br />
presentations, displays interviews, exhibitions, and advertising, to promote and<br />
encourage participation.<br />
A single large event for key stakeholders was organised, focus groups were used to<br />
feedback their responses to the questionnaires.<br />
What information was given?<br />
22
All people including stakeholders were given a briefing note and access to other<br />
informative resources before given the questionnaire or attending one of the groups<br />
or meetings. Information included:<br />
• a background to the Drug and Alcohol Services<br />
• The current treatment system<br />
• gaps and weaknesses in the current drug treatment system<br />
• gaps and weaknesses in the current alcohol treatment system<br />
• key changes being proposed included those to address the following topics:<br />
o accessibility<br />
o the range of services available<br />
o moving towards primary care services<br />
o quality of life issues<br />
o criminal justice role<br />
o one single point of access / treatment<br />
o one venue for both drugs and alcohol services.<br />
Finally there was information on why people should take part in the consultation<br />
process by providing views and comments on the proposed changes to drug and<br />
alcohol treatment services, also there was information on where to get a<br />
questionnaire and alternative feedback methods available.<br />
What were people asked to comment on?<br />
There were questions based on a combined drug and alcohol pathway including:<br />
• accessibility of services<br />
• a wider range of services<br />
• having services accessible through primary care, ie, GPs<br />
• should ‘quality of life’ services (for example housing support, relapse<br />
prevention, education and life skills training) be included in drug and alcohol<br />
treatment<br />
• should the service be flexible to suit the service users needs<br />
• should the service be community based<br />
• should the service be in a neighbourhood setting<br />
• should there be a single drug and alcohol service for people in the criminal<br />
justice system (before sentence and following release)<br />
• should non-drug and alcohol children and young person agencies have<br />
support available<br />
• should there one venue for both drug and alcohol services<br />
People who worked with alcohol services only were asked an additional question<br />
about an assessment of treatment being completed in a single point of access.<br />
Summary of feedback<br />
There were 404 responses for the adult survey and 110 responses for the young<br />
person’s survey.<br />
The stakeholder groups within the adult and young person’s community engagement<br />
group varied from those having no experience or knowledge of drug and alcohol<br />
services to those who were currently or had previously been in receipt of services or<br />
had worked in services and this was reflected in their responses.<br />
23
Those that had less knowledge and experience were able to make valuable<br />
contributions. For example, the positive impacts of accessible community based<br />
services, and the contributions that families and communities could make to support<br />
both service users and services at local level.<br />
Overall people were supportive of the changes. Negative responses centred on adult<br />
drug and alcohol users receiving treatment within GP surgeries. There was overall<br />
support for this change, but on the principle that this service would be located within<br />
a different part of the surgery and at different times to regular GP appointments.<br />
There was positive support for the proposed changes to young people’s drug<br />
treatment services. One community based service for young people was principally<br />
supported on the basis that young people should feel safe and that the service was<br />
available especially for them.<br />
Service providers gave mixed responses to the service redesign changes. Better<br />
accessibility received the most positive responses, including weekend and late<br />
opening and operating times, with neighbourhood based services meaning less<br />
travelling was involved. Negative responses highlighted drinkers not wanting to<br />
associate with drugs users and the potential barriers due stigmatisation of drug and<br />
alcohol users within the community.<br />
Service providers considered the impact of equality issues within their stakeholder<br />
event, relating to the proposed changes to treatment services. This will contribute to<br />
the Equality Impact Assessment for service redesign and change.<br />
Decisions made<br />
The redesign of young person’s alcohol and drug services is being carried out in<br />
conjunction with the adult drug and alcohol treatment redesign. It is proposed that<br />
the end product of the redesign process will be a specialist treatment service that will<br />
deliver treatment and support the delivery of information, advice and guidance in<br />
mainstream services.<br />
Based on the findings of the adult and young person’s stakeholder consultation, it<br />
was recommended the feedback and proposed changes to drug and alcohol<br />
treatment are implemented and should inform the commissioning and service<br />
redesign processes.<br />
24
End of Life Care<br />
What was the issue?<br />
We aimed to develop a strategy to deliver the best quality care pathway for all those<br />
of 18 years and over who are approaching the end of their lives.<br />
Who was consulted?<br />
Broad and wide engagement took place to inform the strategy. Two stakeholder<br />
events took place attended by staff across Leicester, Leicestershire and Rutland and<br />
included staff from University Hospitals Leicester, LOROS, Community Health<br />
Services, East Midlands Cancer Network, local authorities, Leicester University, East<br />
Midlands Strategic Health Authority, Voluntary Action Leicester, Foundation Housing,<br />
Hospice Hope, Confederation of Indian Organisations, NHS Leicestershire County<br />
and Rutland, NHS Leicester City, GPs, palliative care consultants; out-of-hours GP<br />
services, pharmacists, the public and carers.<br />
A questionnaire was developed and sent to all those who had joined the NHS<br />
Leicestershire County and Rutland membership scheme (approx 3,000 members)<br />
and members of NHS Leicester City membership scheme who had previously<br />
expressed an interest in end-of-life care.<br />
What information was given?<br />
The first event held in May 2010 was designed to identify the improvements that<br />
stakeholders felt were important. It was themed around the National End of Life<br />
Strategy.<br />
The second event held in July 2010 was designed to confirm and challenge the three<br />
supporting documents developed to deliver the improvements. Therefore,<br />
information given included the NHS Leicester, Leicestershire and Rutland End of Life<br />
Care Strategy, Action Plan and the High Level Care Pathway.<br />
The questionnaire was designed to canvas the views of members about the strategy.<br />
Its purpose was to provide a local snapshot, in time, to gauge local current<br />
awareness and views of the population on end-of-life care.<br />
What were people asked to comment on?<br />
At the first stakeholder event, people were asked to comment on improvements they<br />
felt to be most important. The objectives of the event were:<br />
• to achieve a common understanding of what was happening currently across<br />
Leicester, Leicestershire and Rutland<br />
• to identify and understand current gaps in the services.<br />
At the second event people were asked if they were happy that the priorities<br />
identified at the first stakeholder event could be identified in the three documents<br />
including the strategy, the action plan and the care pathway. If not, stakeholders<br />
were asked to challenge this apparent omission.<br />
Summary of feedback<br />
The priorities identified were at the first stakeholder meeting were:<br />
• choice<br />
25
• co-ordination of processes<br />
• assessment<br />
• 24hr access to services<br />
• verification of death<br />
• care after death<br />
Following the event these priorities were reflected in the action plan.<br />
At the second stakeholder event held in July 2010 the stakeholder group were asked<br />
to confirm and challenge the three documents listed above. It was agreed that all the<br />
priorities identified at the first stakeholder group meeting had been included in the<br />
documents.<br />
In all, 2000 questionnaires were received from the questionnaire sent out to<br />
members. Information gathered from the feedback told the trusts that 60% of LCR<br />
members and 75% of LC members wished to die at home.<br />
To support ‘choice to die at home’ people felt it was important to be able to access a<br />
full range of services including specialist services, equipment and support for carers<br />
and family. These themes were also highlighted as the reasons people die in<br />
hospital rather than at home.<br />
To help people to talk about ‘planning a good death’, the top two themes were to<br />
provide leaflets in GP surgeries and raise awareness through the television and<br />
radio.<br />
The majority of respondents agreed that hospice care should be reserved for the<br />
most complicated cases. However, this was contradicted when the majority<br />
responded that, even if they did not meet the criteria for hospice care, they should<br />
still be allowed access. Alternative arrangements identified would be to provide<br />
hospice at home or nursing care home.<br />
Decisions made<br />
The <strong>PCT</strong> Trust Boards agreed the strategy on 14 October 2010. With the<br />
introduction of the High Level Care Pathway, all patients approaching end of life, and<br />
their carers will:<br />
• have their physical, emotional, social and spiritual needs and preferences<br />
assessed by a professional with appropriate skills and competencies<br />
• have an effective care plan<br />
• have their needs, preferences and care plan reviewed as their condition<br />
changes with the appropriate systems in place to ensure that this information<br />
can be accessed by all relevant health and social care staff<br />
By 2014 end-of-life care will:<br />
• be effectively co-ordinated across all sectors<br />
• ensure patients and carers will feel well supported<br />
• provide good quality of care in the last months, weeks and days of life<br />
• have effective processes in place for the verification and certification of death<br />
and care after death<br />
• ensure that quality and effectiveness of care will be robustly monitored<br />
26
• ensure that there will be equality in access to and provision of end of life care<br />
services<br />
• ensure that all carers report their experience as ‘the best possible’.<br />
All those who had taken part by attending meetings and completing the<br />
questionnaire were informed of the results via the media, by publishing the strategy<br />
and our Trust Board papers online, and via the membership schemes’ newsletters.<br />
Members were also emailed the decisions taken.<br />
27
Greater Choice and Control and the Information Revolution<br />
White Paper<br />
What was the issue?<br />
The Department of Health released two White Papers - Greater Choice and Control<br />
and The Information Revolution.<br />
In Greater Choice and Control, the DH proposed a vision of an information revolution<br />
in which people have the information they need to stay healthy, to take decisions<br />
about and exercise more control of their care, and to make the right choices for<br />
themselves and their families. This includes an accurate record of their care which is<br />
available to them electronically. Health and adult social care information will be<br />
liberated from a closed, bureaucratic system in order to serve patients and the<br />
public, and to help drive better care, improve outcomes, innovation and better use of<br />
resources.<br />
In The Information Revolution the DH proposed moving:<br />
• away from information belonging to the system to information enabling<br />
patients to be in control of their care<br />
• away from patients and service users merely receiving care to being active<br />
participants in their care<br />
• away from information for administrative and technical needs to information<br />
based good clinical and professional practice<br />
• away from top-down information collection to a focus on meeting the needs of<br />
individuals and local communities.<br />
NHS Leicester City, and NHS Leicestershire County and Rutland’s objective was to<br />
capture the voice of all stakeholders, public members and communities in the city by<br />
inviting them to provide feedback on the consultation and inform them on the<br />
changes which will be happening as a result of these White Papers.<br />
Who was consulted?<br />
The consultation was organised on behalf of Leicester City Council, NHS Leicester<br />
City and NHS Leicestershire County and Rutland. A number of communication<br />
channels and methods were used to gather the feedback required. Emails and<br />
letters were sent to over 100 local stakeholders. Over 5,800 emails and letters were<br />
sent to NHS Leicestershire County and Rutland and NHS Leicester City’s public<br />
members, who had chosen to provide feedback on health topics. Stakehloder<br />
briefings also took place.<br />
There were press releases to local media hubs for both radio and newspaper<br />
release. There was a session on Kohinoor Radio, a multi-lingual radio station,<br />
informing various communities of the proposed changes for public health. There was<br />
a fairly rounded response in terms of demographics, many of the communities<br />
invited either attended the consultation event or sent back their feedback via a<br />
questionnaire.<br />
What information was given?<br />
A briefing of the main points of the White Paper was given out with the questionnaire<br />
and was presented at the consultation events. The easy read version of the White<br />
Paper was sent with the questionnaire to people requesting paper copies.<br />
28
What were people asked to comment on?<br />
The Greater Choice and Control consultation, launched on 18 October 2010, asked<br />
for views on:<br />
• what extending patient choice could mean and how it could work in practice<br />
• whether the proposed choices are the ones that people want<br />
• how shared decision-making can become the norm, in particular the 'no<br />
decision about me without me' ethos<br />
• having the right information, technology and infrastructure in place<br />
• arrangements to support choice of any willing provider, such as pricing<br />
• possible new duties on healthcare providers and professionals<br />
• personal health budgets.<br />
The Information Revolution consultation, launched on 18 October 2010, asked for<br />
views on:<br />
• transforming the way information is collected, analysed and used by the<br />
NHS and adult social care services<br />
• providing good information for patients and their families in line with the 'no<br />
decision about me without me' principles and a culture that enables people<br />
to make use of it<br />
• publication of data for public accountability<br />
• the role of information in improving outcomes for patients and service users<br />
• professionally endorsed and universally applied standards for recording<br />
care, including the role of informatics as a profession<br />
• giving people control of their care records and allowing them to share it as<br />
they see fit with others<br />
• encouraging greater use of technology and information to provide more<br />
convenient care and means of communication, and to create efficiencies to<br />
free up resources<br />
• an information strategy, including the NHS Commissioning Board and<br />
Department of Health's role in setting clear national informatics standards<br />
for both the NHS and adult social care.<br />
Summary of feedback<br />
The responses of the people of Leicester, Leicestershire and Rutland to the specific<br />
questions asked in this national consultation have been submitted to the Department<br />
of Health.<br />
Based on the feedback from consultation channels, local respondees detailed that<br />
the way people can have greater choice and control over their care is to have GPs<br />
offer more consultation time. In addition they would like to have the statistics about<br />
the success or otherwise of operations performed by surgeons. In conclusion, people<br />
wanted hospital success rates so they could choose where they go based on<br />
treatment outcomes. The discussion prompted comments on topics not directly<br />
connected to the consultation issues, such as inadequate hospital parking and public<br />
transport to healthcare providers.<br />
Decisions made<br />
Feedback was sent to the Department of Health as part of the national consultation<br />
process and the draft legislation, based on the principles of these White Papers is<br />
currently going through Parliament.<br />
29
Maternity and neonatal services review<br />
What was the issue?<br />
The engagement process for the Next Stage Review – Leicester, Leicestershire and<br />
Rutland maternity and neonatal services took place throughout November 2009<br />
aimed at service improvement in line with the vision report published in 2008. A<br />
summary of the 2009 engagement process and its impact is included in this 2010-11<br />
report, because the engagement informed Trust Board decisions taken in December<br />
2010.<br />
Who was consulted?<br />
More than 1,600 questionnaires were sent to mothers who gave birth during a sixweek<br />
period earlier in the year. Questionnaires were sent out to 27 Sure Start<br />
centres across Leicestershire county and Leicester city, where staff helped parents<br />
to complete them. Also, questionnaires were sent to 973 nursery and toddler groups<br />
and 233 primary schools in Leicestershire. Members of the two <strong>PCT</strong>s’ public<br />
membership schemes received information about the questionnaire and were invited<br />
to attend the events.<br />
Teams also attended other events and meetings to speak to harder-to-reach groups,<br />
including asylum seekers, younger mums, those living in rural areas, women from<br />
the south Asian community and gypsies and travellers. A special easy read version<br />
of the questionnaire was also created for those with learning disabilities.<br />
More than 100 people attended the public events, and thousands of people were<br />
made aware of the questionnaire via the media and the distribution processes<br />
described. More than 800 questionnaires were completed.<br />
What information was given?<br />
Presentations were given at the events to inform people on the NHS Leicestershire<br />
County and Rutland vision for the service and the challenges associated with making<br />
that vision a reality. This was followed by an overview of the current service. An<br />
introduction to distributed questionnaires also described the relevant information.<br />
What were people asked to comment on?<br />
People were asked to comment on maternity services and the care of newborn<br />
babies (eg, special care units). Women of childbearing age were asked to comment<br />
on the distances they were willing to travel to access maternity services and<br />
appropriate services for their newborn babies.<br />
Summary of feedback<br />
More than 800 people had their say on the future of maternity and newborn services<br />
in Leicestershire and Rutland as part of an engagement programme. Their views<br />
were fed back into the ongoing planning for local maternity and newborn services.<br />
Decisions made<br />
During the financial year 2009-10, as a result of this consultation the NHS health<br />
community covering Leicester, Leicestershire and Rutland improved early access to<br />
maternity services with new support workers and specialist midwives. A number of<br />
other options were developed for the future of maternity and newborn care in<br />
Leicester, Leicestershire and Rutland.<br />
30
In December 2010 these other options went to the Trust Board of University<br />
Hospitals of Leicester NHS Trust, NHS Leicestershire County and Rutland and NHS<br />
Leicester City. This was publicised via the local media and the trust websites, to<br />
inform the people who took part in the maternity and neonates engagement activities<br />
of the outcomes of the review.<br />
31
Maternity Service Liaison – designing a 12-month rolling<br />
programme<br />
What was the issue?<br />
NHS Leicester City and NHS Leicestershire County and Rutland’s Maternity Service<br />
Liaison Committee (MLSC) identified a need for a dialogue with mothers regarding a<br />
variety of issues in maternity services. Mothers are perceived as a difficult group to<br />
communicate with due to childcare and work responsibilities. To communicate<br />
successfully, two focus groups were set up, one in the city and one in the<br />
Leicestershire to identify the best communication channels. This research informed<br />
the design of a 12-month rolling programme of interaction to identify key issues and<br />
look for solutions.<br />
Who was consulted?<br />
Initially two small focus groups of mothers were consulted, both with under 10<br />
members.<br />
What information was given?<br />
It was explained that there was no extra funding available and not everything could<br />
be solved immediately, but wherever possible service changes and improvements<br />
could be made. There was also information on joining the liaison committee as a<br />
patient representative and options for communication.<br />
What were people asked to comment on?<br />
There were four main subjects for discussion initially, which informed the planning of<br />
the 12-month engagement plan. The subjects were essentially questions:<br />
• How did they want to be involved?<br />
• What do they think of having a workshop?<br />
• How did they want feedback to be given to them?<br />
• What topics did they want to discuss throughout the programme?<br />
Summary of feedback<br />
People wanted to be involved using both newsletters and websites together, or<br />
through communication from children’s centres, Sure Start and interviews.<br />
They thought focus group were not appropriate, as the times of mothers’ availability<br />
varied.<br />
They said that feedback should be via website or a newsletter and include<br />
signposting to other available services and that topics should include ante-natal<br />
services, parent craft, communication, having the baby, post-natal care, breast<br />
feeding and bottle feeding and complaints.<br />
Decisions made<br />
A newsletter has been produced covering specific topics of interest, and this is fed<br />
out via email, websites and relevant mother and baby groups and organisations.<br />
32
Naming the IAPT service<br />
What was the issue?<br />
As part of the government's £170 million investment in Improving Access to<br />
Psychological Therapies (IAPT) programme - which was designed to open up easy<br />
to access, effective mental health services to people in need - we have<br />
developed two new services to provide better access to talking therapies for people<br />
living in Leicester, Leicestershire and Rutland.<br />
The two <strong>PCT</strong>s consulted with the communities of Leicester City and Leicestershire<br />
and Rutland to rename the IAPT service to something more meaningful. This had to<br />
cover a variety of target groups, including the young and old, male and female and<br />
those of different ethnic origins.<br />
Who was consulted?<br />
NHS Leicester City, and NHS Leicestershire County and Rutland consulted various<br />
patients, representative groups, community leaders and members of the two trusts to<br />
devise a list of potential titles and then vote on their preferred names from that list.<br />
There was a media release explaining when and how voting was taking place,<br />
explaining that it was open to all stakeholders and the public to vote on the preferred<br />
name.<br />
What information was given?<br />
In the focus groups, members were given a brief background of what the service was<br />
about and why a new name had to be created to be meaningful to residents. This<br />
information was then put in a briefing for a media release, which was available on<br />
the website and was sent to the membership for the voting process.<br />
What were people asked to comment on?<br />
The focus groups were asked to respond to various parts of communicating about<br />
the service, this included:<br />
• creating some names for the service<br />
• commenting on how information should be communicated to patients, such as<br />
posters, leaflets and other paper based media<br />
• commenting on where the information on the service should be readily<br />
available<br />
• explaining how the service should be described including what type of<br />
language would be understood by the various communities.<br />
Summary of feedback<br />
Comments were grouped under the following shared themes:<br />
• certain words related to mental health need to be avoided as they increase<br />
stigma and will reduce referral rates<br />
• leaflets which are discrete were chosen as the best paper based medium to<br />
promote the service as they can easily be slipped into a pocket or a bag<br />
• information to be available at relevant community locations such as support<br />
groups, local services, GP surgeries and pharmacies<br />
• radio and media releases would be a positive way of promoting the service.<br />
Decisions made<br />
33
For people living in Leicestershire County and Rutland the service is called Good<br />
Thinking.<br />
For people living in Leicester City the service is called Open Mind.<br />
The patients chose leaflets to be the best form of information to be used and wrote<br />
the content together with the service commissioner via a reader’s panel format to<br />
reduce stigma and increase understanding.<br />
The leaflets are available in GP surgeries and relevant community groups services to<br />
increase self referral.<br />
Media releases were sent out to promote the service and information on where the<br />
service is and further information was also included in the media releases.<br />
34
Older Persons Month<br />
What was the issue?<br />
This was a project between numerous partners. The consultation was on behalf of<br />
NHS Leicester City, NHS Leicestershire County and Rutland, Leicester City Council<br />
and Leicestershire County Council.<br />
Older Persons Month is a local month of awareness-raising for issues affecting<br />
people over the age of 50. During this month, events are run to raise awareness of<br />
issues, promote tools and solutions to problems and help people interact and be<br />
active. This happens across Leicester City, Leicestershire County and Rutland. In<br />
September 2010, the city and the county joined forces to promote the event across<br />
the whole area. The problem which arose was that the city and the two counties<br />
have very different demographics and organisers needed to know what the key<br />
health issues were and what types of events would prove most effective for city<br />
residents.<br />
Who was consulted?<br />
Members of NHS Leicester City, community groups and local representative groups<br />
What information was given?<br />
All members involved were given a briefing explaining what the purpose of older<br />
persons month was and where there is thought to be health gaps which need<br />
consideration throughout the month.<br />
What were people asked to comment on?<br />
People were asked to comment on what they thought were health issues affecting<br />
people over 50 and what types of events would be useful to promote the different<br />
health issues in those areas. This was done in community meetings and at events.<br />
Summary of feedback<br />
There were some enthusiastic responses resulting in further partnership working for<br />
running different types of events across the city. People highlighted isolation, low<br />
activity and fitness, safety, healthy eating and mental health as key issues affecting<br />
older people. They felt awareness events and activity events should be based on<br />
these issues and should be taken to the individual communities not be city centre<br />
based as this would result in less attendance of people who need to be targeted.<br />
Decisions made<br />
The following events were run:<br />
• two mental health and wellbeing activity sessions in a care home<br />
• a Health and Safety event in Saffron<br />
• A Caribbean Culture Celebration Day was held in partnership with the<br />
Caribbean Court and delivered in Highfields<br />
• A Senior Citizens Health awareness event in Belgrave<br />
• An Older Person’s Fun Day including dance activities<br />
• A Young At Heart event including activity sessions in New Parks<br />
• A health talk on Alzheimer’s and dementia in partnership with Leicestershire<br />
Partnership NHS Trust was held in Braunstone<br />
• A health talk on Alzheimer’s and dementia in partnership with Leicestershire<br />
Partnership NHS Trust was held in St Marks<br />
35
Pharmaceutical Needs Assessment<br />
What was the issue?<br />
NHS Leicester, and NHS Leicestershire and Rutland has 206 pharmacies and 19<br />
dispensing doctors in the Leicestershire County and Rutland, ie, a doctor’s surgery<br />
which is able to supply medicine and which provides an increasingly wide range of<br />
services. We asked patients who access NHS services to tell us what they think<br />
about the service pharmacists and dispensing doctors currently provide. This is<br />
called the Pharmaceutical Needs Assessment (PNA).<br />
By law, all primary care trusts in England must publish a Pharmaceutical Needs<br />
Assessment by the 1 February 2011 to:<br />
• highlight whether there are gaps in the services provided by pharmacists<br />
• show pharmacists and dispensing doctors which services are required,<br />
where and by whom<br />
• assist NHS LCR with their commissioning of high quality services.<br />
The aims of the Pharmaceutical Needs Assessment are:<br />
• to gain a complete picture of the population within the NHS LLR area<br />
• to identify specific communities with particularly poor health<br />
• to enable comprehensive ‘benchmarking’ comparison with comparable<br />
populations<br />
• to give a clear view of unmet needs.<br />
Who was consulted?<br />
In order to produce a meaningful Pharmaceutical Needs Assessment it was<br />
necessary to understand what people thought about current services offered by<br />
pharmacists and dispensing doctors and how services should be shaped for the<br />
future. Therefore, an engagement process was undertaken from mid June 2010 to<br />
mid July 2010. Engagement was broad and far reaching and included a<br />
questionnaire (available online, in hardcopy and as an easy read version) alongside<br />
face to face engagement with a variety of community groups, including 13<br />
community forums throughout Leicestershire and similar meetings in Rutland. The<br />
following seldom heard groups were also included:<br />
• people with learning disabilities<br />
• gypsy/travellers<br />
• older people<br />
• young people<br />
• asylum seeker and refugees<br />
• people with visual impairment<br />
• carers<br />
• people living in areas of health inequalities<br />
• BME groups<br />
• people living in rural isolation.<br />
In the Leicester City area, Officers organised meetings with relevant stakeholders<br />
who had interest in community pharmacy services, these included:<br />
• ADHAR - an organisation that provides support for Asian people with<br />
mental health conditions<br />
36
• LOROS - (Leicestershire and Rutland Organisation for the Relief of<br />
Suffering) a local charity providing skilled nursing and specialist care within<br />
Leicester, Leicestershire and Rutland<br />
• WISCP – (West Indian Senior Citizens Project) an organisation who provide<br />
a support service for the elderly Afro – Caribbean population<br />
• VAL – (Voluntary Action Leicester) a key voluntary organisation that<br />
involves volunteers in improving life in Leicester and Leicestershire<br />
• CLASP – (Carers of Leicestershire, Advocacy and Support project) a charity<br />
that provides support services for carers in Leicester, Leicestershire and<br />
Rutland<br />
• A young mothers group<br />
• A Travellers group<br />
An easy-read presentation was developed for these groups.<br />
Questionnaires were sent out to all pharmacies across Leicester, Leicestershire and<br />
Rutland for them to distribute to customers, and NHS LLR members were invited to<br />
complete the questionnaire.<br />
Leicester, Rutland and Leicestershire LINks invited their members to complete the<br />
questionnaire, and Rutland LINk steering group also received a presentation. By<br />
working in partnership with Voluntary Action Leicestershire and Rutland we were<br />
also able to invite members of the voluntary sector to be part of the engagement<br />
process.<br />
The second phase of this process began on 1 September, in the form of a 60-day<br />
consultation on pharmaceutical needs, which ended on 30 October 2010.<br />
What information was given?<br />
When attending meetings a presentation was given to explain what the PNA was<br />
and why feedback was needed from the public on current services to ensure it was<br />
fit for purpose. As an introduction to the online questionnaire and the hard copy<br />
questionnaires a full briefing was attached. This included information on the purpose<br />
of the final PNA document.<br />
In the second phase of this process information was given on the feed back from the<br />
engagement process.<br />
What were people asked to comment on?<br />
During the engagement process stakeholders and members of the public were<br />
asked:<br />
• Who uses pharmacists and dispensing doctors?<br />
• Which services offered by pharmacies are used most?<br />
• Whether or not people think pharmacies and dispensing doctors are<br />
convenient<br />
• Whether people would like more services from their local pharmacy.<br />
During the consultation people were asked:<br />
• Do you agree that the eight smaller areas (localities) best reflect the areas of<br />
Leicester, Leicestershire and Rutland, and that they are the right areas?<br />
37
• From the information in the PNA and your personal experience do you believe<br />
your pharmaceutical needs are met?<br />
• Do you feel that the purpose of the PNA has been explained sufficiently?<br />
• Do you feel the pharmaceutical needs of the population of Leicester City,<br />
Leicestershire County and Rutland have been adequately reflected?<br />
• Do you feel that we have responded to the needs shown in the feedback<br />
through the engagement process and included the into the PNA document?<br />
Summary of feedback<br />
More than 700 questionnaire responses were received in the engagement phase.<br />
Following the release of the final draft of the PNA the <strong>PCT</strong> received over 100 online<br />
responses and over 20 comments by letter from stakeholder organisations including<br />
the Local Pharmaceutical Committee (LPC) and neighbouring <strong>PCT</strong>s and LPCs.<br />
From the engagement and consultation process the <strong>PCT</strong>s have gained a wealth of<br />
knowledge. Overall findings identified that one fifth of respondents use a GP<br />
dispensary to obtain their medicines. Most respondents use pharmaceutical services<br />
on a regular basis for ongoing medical conditions and for the collection of medicines.<br />
A high percentage of respondents use the same pharmacy on a regular basis and<br />
this was mostly due to the convenient location and continuity of care. A high number<br />
of respondents are happy with their arrangements for repeat medication and more<br />
than half have never had any problems with their medicines. A high proportion of<br />
respondents reported that they had received enough information about their<br />
medicines and that the information was helpful. In Leicestershire and Rutland only<br />
8% had experienced problems in finding a pharmacy to meet their needs within the<br />
last 12 months. Of those, the problem was not generally related to access but more<br />
to the supply of medicines. There was a general awareness of some of the other<br />
services available from local pharmacies.<br />
Decisions made<br />
Members of the public and stakeholders involved in the engagement and<br />
consultation process were informed when the PNA was to be agreed at the Trust<br />
Board in January 2010. The PNA was made available to view via the website and<br />
hard copies made available on request. They were also informed that the PNA would<br />
be used by the <strong>PCT</strong> as a commissioning and market-entry tool, ie, a tool to help<br />
them understand on what basis services are commissioned. It will also be used by<br />
the public as an information document.<br />
Enhanced service commissioning from community pharmacy is led by need, crucially<br />
a need that can be addressed by community pharmacy. The <strong>PCT</strong> currently<br />
commissions a range of enhanced services aimed at meeting needs that exist,<br />
across the City. This PNA has not identified any current health need that would<br />
require an enhanced service from community pharmacy and in the current economic<br />
position is not, realistically, likely to secure funding for such a service. However the<br />
<strong>PCT</strong> will continue to work with community pharmacy to understand the health<br />
outcomes from the range of non-commissioned services which are predominately<br />
related to health improvement, with a view to developing models for future enhanced<br />
services, should funding become available.<br />
38
Public Health White Paper<br />
What was the issue?<br />
The Department of Health released a national White Paper for consultation entitled<br />
Healthy Lives, Healthy People: Our Strategy for Public Health In England. It sets out<br />
the Coalition Government’s new approach to public health and some of the<br />
structures and processes that will support delivery. The vision is to protect the<br />
population “from serious health threats, helping people live longer, healthier and<br />
more fulfilling lives; and improving the health of the poorest fastest”.<br />
There were important factors to be considered when inviting stakeholders to take<br />
part to ensure all community voices were heard. Leicester’s predominant ethnic<br />
minority community is of south Asian origin. Leicestershire County and Rutland’s<br />
demographic profile is very different and has an ageing population, so it was<br />
important to gather a representative response to support the national consultation.<br />
NHS Leicester City, and NHS Leicestershire County and Rutland wanted to capture<br />
the voice of all communities, stakeholders and public in the city and county by<br />
inviting them to provide feedback on the consultation and inform them on the<br />
changes which will be happening as a result of this White Paper.<br />
Who was consulted?<br />
NHS Leicester City, and NHS Leicestershire County and Rutland undertook an<br />
engagement exercise including surveys, questionnaires and consultation events.<br />
The consultation events were held for patients, members of the public, NHS staff,<br />
clinicians, local authorities, voluntary sector organisations and seldom heard groups<br />
to ensure a wide range of views was collected.<br />
What information was given?<br />
A briefing of the main points of the White Paper was provided with the questionnaire<br />
and was delivered verbally at the consultation events. An easy read version of the<br />
White Paper was sent to people requesting paper copies of the questionnaire.<br />
What were people asked to comment on?<br />
Everyone was asked to comment on the proposals being made in the White Paper,<br />
along with any concerns and potential solutions that all needed to be taken into<br />
consideration both locally and nationally.<br />
Summary of feedback<br />
The strong partnerships across the city, two counties, local authorities and other<br />
statutory bodies have enabled us to gather a wide range of views.<br />
This indicated broad support for:<br />
• the focus on preventative health<br />
• the new role for the local authority, the establishment of Public Health<br />
England as a means of ensuring consistent health protection<br />
• the local focus – critical for effective services in response to people and their<br />
needs<br />
• the emphasis on the voluntary sector and wider contributions by individuals<br />
and communities<br />
39
• the Health and Well being Board as the local focus which may provide and<br />
ensure local coherence in the commissioning by the local authority for adults<br />
social care and public health and GP-led commissioning groups for health<br />
care<br />
• the ring-fenced budget for public health funding and the health improvement<br />
functions to be performed by the local authority.<br />
There were concerns that:<br />
• health may worsen due to the economic circumstances and the continuing<br />
effects of poverty, particularly on children<br />
• the voluntary sector may not be intact to work with local authorities and GP<br />
consortia in the provision of services and input that improve health and public<br />
health<br />
• the public health budget in general and for local authorities in particular will be<br />
insufficient. (The White paper itself says that funding has not gone into<br />
prevention and there was a concern that in the transition to these new<br />
arrangements might raise expectations but lower funding)<br />
• the Health and Wellbeing Board will lack the authority to create coherence in<br />
the local approach to health care, health protection and health improvement<br />
• the public health premium may distort the issues focussed on locally.<br />
• there is potential for performance indicators to be politicised locally and<br />
nationally – “long term outcomes do not benefit from changing goal posts”,<br />
was one expression of this.<br />
Decisions made<br />
This information was fed back to the Department of Health and used to inform the<br />
current changes being delivered to the reforms of public health.<br />
40
Quality, Innovation, Productivity and Prevention (QIPP)<br />
What was the issue?<br />
NHS Leicester City and NHS Leicestershire and Rutland have taken several<br />
opportunities during 2010-11 to engage with the public on QIPP. Our aim was for the<br />
public to understand the current financial climate and challenges facing the NHS.<br />
The first QIPP event in September 2010 was a joint event without two <strong>PCT</strong>s,<br />
University Hospitals of Leicester NHS Trust (UHL) and Leicester Partnership Trust<br />
(LPT).<br />
Who was consulted?<br />
Members of the public and major stakeholders including both <strong>PCT</strong>’s public<br />
memberships along with people from UHL’s and LPT’s membership schemes.<br />
What information was given?<br />
Those attending were informed that each person in our area was allocated a per<br />
capita healthcare funding amount of £1,600 to pay for treatments, medicines and<br />
equipment, and that some also covered other costs such as the management of<br />
buildings, running vehicles and employing staff. A series of examples of the cost of<br />
services was also given. For example, the average cost for attending the Urgent<br />
Care Centre (open 8am – 6.30pm) is £40. Attending the Minor Injuries Unit is £59 an<br />
hour, and attending the GP out-of-hours service (available 6pm – 8am) is also £59.<br />
Attending the Accident and Emergency Department is also £59 and the average cost<br />
of an overnight stay in hospital is £147. Along with some ‘did you know that’<br />
information, for example, the cost of a hip replacement is £6,000, a knee<br />
replacement is £6,000, a Caesarian section is £2,000 and a normal, uncomplicated<br />
birth is £1,000.<br />
What were people asked to comment on?<br />
Participants were then asked to vote by choosing options to answer a variety of<br />
questions about making services more cost-effective and efficient while maintaining<br />
quality of care. Participants used voting pads to feed back on how they thought<br />
unnecessary admissions could be avoided, where people would consider going for<br />
diagnostic scans, and where they would consider accessing minor surgery; and<br />
more.<br />
Summary of feedback<br />
Feedback indicated that members of the public were willing to consider alternative<br />
options for service delivery.<br />
Decisions made<br />
The public received immediate feedback totals from the voting system and were told<br />
that information gathered would be used for future QIPP considerations by<br />
healthcare commissioners and providers. This event was also used to inform the<br />
content of further QIPP engagement work.<br />
41
Quality Innovation, Productivity and Prevention:<br />
Strategic Operating Plan<br />
What was the issue?<br />
As part of the engagement about our spending priorities in our Strategic and<br />
Operating Plan for 2011-12, NHS Leicester City and NHS Leicestershire County and<br />
Rutland held a public event and workshop on the morning of 31 January 2011.<br />
Who was consulted?<br />
Members of both organisations’ membership schemes were invited, and altogether<br />
more than 80 people attended. Key stakeholders from the voluntary sector and Local<br />
Involvement Networks were also invited, together with representatives of seldom<br />
heard groups, including people with learning and other disabilities, gypsy travellers,<br />
and people from BME groups.<br />
What Information was given?<br />
During the event, there were presentations about the financial context from Sue<br />
Bishop, Director of Finance for NHS LCR, and Dr Tim Daniel, Consultant in Public<br />
Health Medicine at NHS LCR.<br />
What were people asked to comment on?<br />
The participants were asked about their views on health spending via a number of<br />
simple statements. During the workshop, they decided by a vote how they would<br />
theoretically allocate funding to a number of common procedures and treatments,<br />
including drugs and preventative treatments. They were then given more information<br />
about each of the procedures, including their costs, success rates and clinical<br />
effectiveness, and were asked to vote again in the light of the new information.<br />
During feedback, they had opportunities to make comments, which were also<br />
captured.<br />
Summary of feedback<br />
The notional budget at this event was in the form of a sheet of adhesive peel-off<br />
‘dots’. Attendees allocated as dots to each procedure in line with their priorities and<br />
preferences. The first time they voted, participants divided up their notional money in<br />
the following ways (the first figure refers to the number of peel-off dots, the second<br />
figure is the percentage of the notional budget):<br />
Total Workshop 1<br />
33.7%<br />
81, 21%<br />
89, 22%<br />
17, 4%<br />
36.5, 9%<br />
42, 11%<br />
42, 11%<br />
49, 13%<br />
42<br />
Wisdom teeth extract<br />
Stop smoking campaign<br />
Alcohol abuse prevention<br />
Hip replacement surgery<br />
New bowel cancer drug<br />
Bowel cancer screening<br />
Kidney transplant<br />
IAPT
Comments included:<br />
• prevention and public education is a priority<br />
• knee replacement - it is up to the individual to make the most of it, if it is to be<br />
effective and improve quality of life<br />
• treatment should not be age related<br />
• kidney transplants are saving lives and are cheaper than dialysis<br />
• mental health has additional costs<br />
• more investment and support for carers is needed<br />
• prevention must take priority - what is the benefit of alcohol treatment?<br />
• mental health had the most votes while wisdom teeth had a low priority<br />
After further explanation about the conditions and treatments, their costs, success<br />
rates and clinical effectiveness, participants voted again. These are the results:<br />
Total Workshop 2<br />
3, 1% 31, 8%<br />
92, 26% Wisdom teeth extract<br />
46, 12% Stop smoking campaign<br />
Alcohol abuse prevention<br />
Hip replacement surgery<br />
40, 11%<br />
57, 15%<br />
New bowel cancer drug<br />
Bowel cancer screening<br />
Kidney transplant<br />
77, 21%<br />
24, 6%<br />
IAPT<br />
In the second vote less was allocated to wisdom teeth extraction (just one per cent),<br />
stop smoking campaigns, a new bowel cancer drug which prolongs life for a few<br />
weeks, and bowel cancer screening. More was allocated to alcohol abuse<br />
prevention, hip replacement surgery, kidney transplant, and psychological therapies.<br />
A major theme in the discussion and feedback was the importance of prevention,<br />
including screening, eg, for different cancers, monitoring of school children. People<br />
also debated quality of life. Mental health was seen as important, and people were<br />
interested in the comparative costs of a transplant as against regular dialysis. A<br />
strong point was also made about the importance of support for carers.<br />
Other key themes included the importance of good health education, a sense that<br />
people should take some responsibility for their own health costs, concern about<br />
mental health issues, concern about the cost of drugs and the potential for saving<br />
some of the money spent on them.<br />
Decisions made<br />
The findings from the event have been used to inform the planning for the financial<br />
year 2011-12 and will also help public health teams in their planning. All members<br />
attending the event were made aware that this is how there feedback would be used.<br />
43
Quality Innovation, Productivity and Prevention (QIPP)<br />
event 3: Right Care – Planned Care<br />
What was the issue?<br />
NHS Leicestershire County and Rutland and NHS Leicester City wanted to improve<br />
their approach to planned care and proposed changes which would help GPs decide<br />
the right care at the right time for patients through standardised referral thresholds<br />
for access to some services. This was intended ensure that the referral process was<br />
based on clinical need and benefits, and was fair and transparent for everyone.<br />
Who was consulted?<br />
A briefing event took place to inform stakeholders of the proposed standardised<br />
referral thresholds for right care. Taking part were those from the membership<br />
schemes of the NHS Leicester City and NHS Leicestershire County and Rutland,<br />
members of the public, the Local Involvement Networks, while representatives from<br />
seldom heard groups were invited to attend the briefing. Those who attended were<br />
asked to complete a hard copy questionnaire at the event, and an online version was<br />
also made available. Those who had been invited to the briefing, but were unable to<br />
attend, were made aware of the online questionnaire and invited to complete it.<br />
What information was given?<br />
Information given identified that the proposed changes were based on the expertise<br />
of local GPs, hospital consultants and other healthcare professionals in the city and<br />
two counties. In addition, recommendations on right care at the right time had also<br />
been drawn from evidence from across the region.<br />
People were also informed that the number of planned care procedures had risen<br />
exponentially over the last few years. Some of these procedures are shown to have<br />
limited clinical value in terms of improvements to the quality of life of patients.<br />
Procedures under consideration were:<br />
• primary knee replacements<br />
• primary hip replacements<br />
• carpal tunnel (wrist) and minor hand surgery<br />
• cataract removal<br />
• tonsillectomy<br />
• some hernia repairs<br />
• assistive conception services.<br />
People were also reassured that, in identifying these procedures, consideration had<br />
been given to the following factors:<br />
• the evidence base to support their development<br />
• the impact that their introduction will have for patients<br />
• clinical support for their introduction<br />
• the wider impact for the local health and social care economy.<br />
It was also explained how assessments would be made for each condition when<br />
using a standardised referral system.<br />
What were people asked to comment on?<br />
44
Following the information giving session, people were given the opportunity to ask<br />
questions. They were then asked to complete a questionnaire. People were asked if<br />
they agreed or not with standardised referral thresholds for each of the conditions<br />
identified. If people did not agree, they were asked to explain their reasons so that<br />
these could be taken into consideration by the trusts.<br />
Summary of feedback<br />
At the briefing event 13 people completed the questionnaires and 92% agreed with<br />
the standardised referral thresholds for all the conditions identified.<br />
Decisions made<br />
Following the consultation with the public, patients, carers and clinicians around the<br />
Right Care thresholds a final list of surgical and referral thresholds were developed.<br />
These have been circulated to primary care clinicians and within local providers. The<br />
referral thresholds have been in use from the 1 st of June 2011 and their impact will<br />
be reviewed on an ongoing basis.<br />
The consultation with the public provided invaluable in informing the development of<br />
the thresholds and ensured that the work we were undertaking was as responsive to<br />
local need as possible in what is a challenging time for the NHS.<br />
45
Transforming community services<br />
What was the issue?<br />
It was necessary to carry out engagement about the planned transfer of community<br />
services out of <strong>PCT</strong>s and into other provider arrangements, in line with national<br />
policy to separate healthcare commissioners from actual providers. Nationally it had<br />
been know as Transforming Community Services (TCS). The change was essentially<br />
a transfer of management arrangements, rather than a change to frontline services,<br />
but it was felt important to engage with the public and stakeholders to give them an<br />
understanding of what was happening.<br />
Who was consulted?<br />
Members of the public and stakeholders were consulted at public meetings in Market<br />
Harborough, Leicestershire, and Oakham, Rutland, as well as at a stall as part of the<br />
pre-meeting ‘wellbeing markets’ at both NHS Leicestershire County and Rutland’s<br />
and NHS Leicester City’s AGMs, and at community forums in Wigston and Oadby.<br />
Key stakeholders had opportunities to comment after regular updates at quarterly<br />
stakeholder briefings during the period April 2010 to January 2011.<br />
What information was given?<br />
Information was given about the national policy to separate commissioner and<br />
provider functions, our locally planned changes to community services and the<br />
perceived benefits.<br />
What were people asked to comment on?<br />
People were given information about the local plans for Transforming Community<br />
Services and asked to comment on how important they felt it was to create ‘one-stop<br />
shops’, to have care closer to home, to have health services that are efficient and<br />
cost effective, including efficient use of buildings and support services. They also<br />
had the opportunity to record any concerns about the plans, and to suggest<br />
improvements.<br />
Summary of feedback<br />
In general, people were supportive of improving services in the suggested ways. The<br />
concerns they expressed were to do with whether re-organisation was needed and<br />
some cited the many reorganisations there have been in the NHS in recent years,<br />
whether re-organisation would improve services, and whether the process would b<br />
expensive. Suggestions for improvements tended to be about better, more<br />
convenient access.<br />
Decisions made<br />
The TCS steering committee and Boards of both <strong>PCT</strong>s noted the feedback as they<br />
continued with plans to transfer community services. The transfer was completed on<br />
31 March 2011, involving the move of most of the services provided by both city and<br />
county community health services to Leicestershire Partnership Trust.<br />
46
The White Paper Equity and excellence: liberating the NHS<br />
What was the issue?<br />
The Department of Health published a White Paper for NHS reform entitled Equity<br />
and excellence: liberating the NHS in July 2010. The paper has wide-reaching<br />
implications for future of the NHS in England.<br />
On 22 July 2010, the DH launched a period of public consultation on the White<br />
Paper, specifying three key issues:<br />
• transparency in outcomes - a framework for the NHS<br />
• increasing democratic legitimacy in health<br />
• commissioning for patients<br />
NHS Leicester City, and NHS Leicestershire County and Rutland wanted to capture<br />
the voice of all communities, stakeholders and public in the city and county by<br />
inviting them to provide feedback on the consultation and inform them on the<br />
changes which could happen as a result of the proposals in the White Paper. There<br />
were important factors that had to be considered to make sure all community voices<br />
were heard. Leicester’s predominant ethnic minority community is of south Asian<br />
origin, while Leicestershire and Rutland do not share this characteristic, but have a<br />
larger ageing population than the city. There are major differences, too, in the levels<br />
of deprivation and affluence between the city and county areas, and we felt it was<br />
important to gather a demographically representative response from across this<br />
diverse area.<br />
Who was consulted?<br />
NHS Leicester City led on the consultation on behalf of both <strong>PCT</strong>s. The main<br />
channels of consultation were:<br />
• both <strong>PCT</strong>s websites<br />
• NHS Leicester City and NHS LCR holding consultation events for local<br />
residents of Leicester and other interested stakeholders<br />
• Questionnaires, both hard copy and electronically, were sent to NHS LCR and<br />
NHS Leicester City membership<br />
• attendance at community events with those stakeholders who possessed<br />
‘protected characteristics’ under the Equality Act 2010.<br />
• briefing and engagement with key patient groups, ie, LINk<br />
• a specially convened briefing and question and answer session with elected<br />
members of Leicester City Council as well as briefings for Leicestershire and<br />
Rutland County Councils.<br />
• consultation sessions with clinicians, especially GPs.<br />
What information was given?<br />
All people involved were given information on the key principles of the changes:<br />
• <strong>PCT</strong>s and Strategic Health Authorities to be abolished from 2013<br />
• GPs to have responsibility and budgets for planning and paying for services<br />
• Greater emphasis on outcomes for patients, rather than simply meeting<br />
targets<br />
• putting patients and the public first<br />
• a greater degree of independence for health care providers and reduced<br />
bureaucracy<br />
47
• health improvement will be the responsibility of local authorities<br />
What were people asked to comment on?<br />
Everyone was asked to comment on the proposals in the White Paper, to express<br />
their concerns and/or to offer potential solutions which could be taken into<br />
consideration both locally and nationally. They needed to understand that the<br />
reforms would see radical changes across the NHS landscape and the provision of<br />
health and social care.<br />
Summary of feedback<br />
Overall the proposals have been met with some support but also apprehension from<br />
a great many key stakeholders - both clinical and non-clinical. However, the<br />
predominant view of all who see the NHS as a vital national resource, is that it needs<br />
to work more effectively to ensure patients are its prime focus and that people’s lives<br />
and health are improved.<br />
Decisions made<br />
The information gathered was sent to the Department of Health as part of the<br />
national feedback process, and the relevant legislation based on these White Papers<br />
is still on its way through Parliament at the time of this report’s publication. However,<br />
during 2010-11 <strong>PCT</strong>s started the process of implementing the key principles of these<br />
reforms, and GPs began the formation of clinical commissioning groups in readiness<br />
to take over most local healthcare commissioning functions from April 2013.<br />
48
Part 2: Leicester City engagements<br />
49
Beaumont Leys Surgery – procurement training<br />
What was the issue?<br />
NHS Leicester City had entered in to an open tender process to secure a new<br />
provider for the Beaumont Leys surgery. Patient representation on the evaluation<br />
and interview panel was sought to ensure that patient views were taken in to account<br />
as part of the process. Training was to be provided.<br />
Who was consulted?<br />
Patients registered at the Beaumont Leys surgery.<br />
What information was given?<br />
Patients attending the training session were given information about procurement<br />
and the steps involved in the tender process.<br />
What were people asked to comment on?<br />
Patients attending were asked to consider whether they would be able to participate<br />
in the procurement process.<br />
Summary of feedback<br />
The attendees found the sessions useful and informative.<br />
Decisions made<br />
Unfortunately those patients who attended the session were not available to<br />
participate on the evaluation dates, providing lessons to be learned in engaging<br />
patients in the stages of the procurement process normally undertaken by trained<br />
professionals. Alternative representation was secured to ensure that the process ran<br />
smoothly in future.<br />
50
Belgrave Medical Centre closure and patient registration<br />
What was the issue?<br />
In September 2010, the Belgrave Medical Centre, a surgery situated in the heart of<br />
Leicester, was closed following the death of the doctor who held the <strong>PCT</strong> contract.<br />
Due to unforeseen circumstances the lease extension for another GP to occupy the<br />
same premises could not be agreed and the GP in question was unable to secure<br />
alternative premises within the locality meaning the Belgrave Medical Centre had to<br />
be closed. The patients registered at the centre had to seek alternative<br />
arrangements at a ‘caretaking’ practice for a period of three months to ensure<br />
continuity of care.<br />
The patient list of the former practice reflected not only an extremely diverse<br />
population, but special consideration also had to be taken of those in need of<br />
specialised communication, such as those who were elderly, vulnerable and those<br />
for whom English was not their first language.<br />
Who was consulted?<br />
All patients at the practice were initially consulted of the surgery’s closure via letter<br />
sent on the 1 September 2010. A patient meeting was arranged for the 10 November<br />
2010 to update them of the situation, gather feedback about individual issues and<br />
discuss a way forward with potential options.<br />
Patients who are unable to attend this event were given the opportunity to submit<br />
their comments by returning a patient questionnaire with translations offered. Over<br />
150 questionnaires were submitted to Leicester City <strong>PCT</strong> and all comments were<br />
recorded and fed into the decision making process. This was followed by 6 patient<br />
registration sessions to support patients to register at alternative practices.<br />
Interpreters were available at these sessions.<br />
What information was given?<br />
Initially the situation and caretaking procedure was explained to the patients on the<br />
surgery’s list. This was carried out by letter in September 2010, with the option to<br />
phone a translation service. There was then a meeting in November 2010 where full<br />
details of the caretaking and possible options for future services were discussed.<br />
Following the meeting, once the <strong>PCT</strong> Board agreed the way forward, information<br />
was sent to patients through the post about alternative practices available and how<br />
to register. This was followed by six ‘drop-in’ sessions arranged for patients to speak<br />
to a member of the <strong>PCT</strong> primary care directorate about local practices and the best<br />
choice for their requirements.<br />
What were people asked to comment on?<br />
Patients were asked about any potential issues arising from the closure and for their<br />
help in deciding the best way forward from a selection of potential options. This was<br />
followed by comments on the type and location of practice they might like to be relocated<br />
to.<br />
Summary of feedback<br />
The main themes that emerged from the engagement process, which patients<br />
commented on were the following:<br />
• practice quality<br />
51
• practice accessibility<br />
• appointment availability,<br />
• practice location<br />
• disabled access<br />
• parking access<br />
• location convenience<br />
• services available<br />
• choice of practice<br />
Decisions made<br />
It was concluded that list dispersal provided a logical and sensible way forward.<br />
Prior to the implementation of dispersal of the patient list, NHS Leicester City<br />
requested that the patients could be assured of the capacity and quality of the local<br />
practices to ensure accessible, quality care was available to all patients.<br />
Patients were able to continue to receive care from the Caretaker practice until 31<br />
December 2010 before dispersal. The patient registration department and the <strong>PCT</strong><br />
Customer Services team assisted patients throughout this process.<br />
The six patient registration drop-in sessions helped to register patients. However,<br />
any patient who was not registered with another practice by the end of the caretaking<br />
arrangements were contacted by Patient Registrations and offered additional<br />
assistance.<br />
52
“Call time on drink” campaign<br />
What was the issue?<br />
As a result of rising hospital admissions relating to alcohol, a social marketing project<br />
was embarked on to help reduce alcohol consumption in the city. This had to be<br />
designed to specifically target communities in particular locations. Therefore the<br />
marketing team engaged with members of the specific communities to design an<br />
appropriate campaign.<br />
Who was consulted?<br />
After an analysis of hospital admission data and mosaic profiling, the project<br />
focussed on three areas of the city, New Parks, Braunstone Park and Rowley Fields,<br />
as well as Eyres Monsell. It was decided to target the 25 to 44 year-old group to<br />
tackle problem drinking at an early age to prevent hospital admissions in later life.<br />
Residents of the three areas within the target age-group were consulted on their<br />
behaviours and attitudes towards alcohol and ideas were generated for interventions<br />
that would help to reduce their alcohol consumption.<br />
What information was given?<br />
Background and current information about alcohol campaigns was provided.<br />
What were people asked to comment on?<br />
People were invited to join in discussions and activities with researchers in groups of<br />
three and in larger focus groups of 12. The discussions covered drinking behaviours,<br />
attitudes towards alcohol and campaigns as well as intervention ideas.<br />
Summary of feedback<br />
• drinking is a by-product of socialising, therefore solutions would still need to<br />
provide opportunities for this<br />
• the campaign needed to be more hard-hitting than existing national<br />
campaigns<br />
• units and recommended drinking levels were not well understood<br />
• liver disease was a well-quoted side effect of excessive drinking, therefore the<br />
campaign also needed to address the wider spectrum of conditions<br />
• the audience was comfortable with receiving support in pharmacies for<br />
smoking cessation services and requested similar support for alcohol.<br />
Decisions made<br />
A hard-hitting campaign was produced promoting the dangers to health of drinking<br />
too much and providing tips on cutting backing while still maintaining a social life.<br />
Drinking limits were discussed in terms of popular drinks as well as units. The<br />
campaign offered 10-minute brief advice in pharmacies in the three selected areas.<br />
53
Medicines Use Review survey<br />
What was the issue?<br />
A benchmarking exercise was carried out to identify training issues for community<br />
pharmacists in order to support them to deliver effective Medicines Use Reviews<br />
(MURs) with patients.<br />
Who was consulted?<br />
We sent three individually tailored online questionnaires to community pharmacists,<br />
GPs and members of the public who had received an MUR in the previous six to 12<br />
months.<br />
What information was given?<br />
A basic description of an MUR was given in the questionnaire.<br />
What were people asked to comment on?<br />
Community pharmacists were asked about the MURs performed recently including<br />
the number of medicines people are currently taking, the type of information given,<br />
the reason for conducting the MUR and any training needs.<br />
GPs were asked about any MURs received, the quality and usefulness of MURs,<br />
reason for the MUR and the effect on patient.<br />
Patients were asked about the reason they had an MUR, their understanding of the<br />
process, how useful it was and the quality of information given to them.<br />
Summary of feedback<br />
Community pharmacists highlighted their MURs were performed for a variety of<br />
reasons and that most patients chosen were on multiple repeat medications.<br />
GPs highlighted that they felt many MURs were a waste of time and NHS resources,<br />
and that patients were often confused by conflicting information given by<br />
pharmacists.<br />
Overall, some patients stated that they found MURs to be useful but some did not<br />
understand why they were having a review at the time it was undertaken.<br />
Decisions made<br />
The Local Pharmaceutical Committee (LPC) felt that the results were inconclusive as<br />
not all community pharmacists and GPs completed the survey. As a result the<br />
Pharmacy Development Group (based at NHS Leicester City) decided that a PR<br />
exercise was needed with GPs and community pharmacists to better understand the<br />
role of MURs and their purpose.<br />
Since then the Pharmacy Development Group has disbanded, and with the ongoing<br />
restructuring of the NHS, there has not been sufficient resource to carry out the<br />
planned PR campaign. However, a newsletter was sent out to signpost community<br />
pharmacists to training which was readily available.<br />
54
New arrivals engagement<br />
What was the issue?<br />
During the winter months local NHS services are put under considerable pressure,<br />
particularly the Accident and Emergency Unit (A&E). Extensive delays are caused<br />
often because people do not know where else to go. This project specifically takes a<br />
targeted approach, and looks at new arrivals to Leicester City. One of the ways of<br />
understanding why new arrivals attend A&E is to engage with a number of different<br />
groups gaining better insight.<br />
The New Arrivals Strategy (2006) defines new arrivals as “Asylum seekers,<br />
refugees, migrant workers, EU nationals who have chosen to make Leicester their<br />
home. A person, who has arrived in Leicester from abroad, and who, because of<br />
being new to the UK, has a significant need for support in accessing services and/or<br />
who needs different services to those of other residents.”<br />
The New Arrivals Strategy also states that, regarding the Leicester population and<br />
A&E interaction, it can mean that new arrivals may initially use emergency services<br />
unnecessarily and may require referral or signposting to mainstream services.<br />
This project aimed to explore and work with residents who have newly arrived (<br />
within 0 to 24 months) in Leicester/UK and/or settled in Leicester and are using A&E<br />
for non-urgent primary care needs. This engagement exercise mainly focused on<br />
new arrivals, including students, who were new to Leicester and did not speak or<br />
understand English, either at all or well.<br />
Who was consulted?<br />
Asylum seekers, refugee groups, Somali, Polish communities, and students were<br />
identified as new arrivals to Leicester. Attendees at A&E were also consulted when<br />
visiting the service.<br />
What information was given?<br />
Information was given and gathered in a variety of ways. Members of the public who<br />
attended A&E were asked to complete a questionnaire. One-to-one interviews were<br />
also conducted with members of public when they came in for their GP appointments<br />
to the ASSIST surgery, a special Leicester City service for asylum seekers.<br />
Information was also given and gathered through focus groups, conducted at Sure<br />
Start centres targeting parents who had newly arrived to Leicester.<br />
What were people asked to comment on?<br />
We wanted to know:<br />
• who uses A&E?<br />
• why people use A&E?<br />
• what is their experience of Primary Medical Care?<br />
• are the Choose Well materials helpful?<br />
• does Choose Well help you go to the right place for medical care?<br />
Summary of feedback<br />
The general consensus from engaging with asylum seekers and refugee groups was<br />
that when people come into the country, initially they are not aware of the provision<br />
of primary health care through GPs. Once given the information they are hesitant to<br />
55
use them due to the fear of being sent back to countries that they have successfully<br />
managed to escape.<br />
In trying to gauge a better understanding from newly arrived communities there is<br />
ample evidence to show that further work needs to be done in reaching out to these<br />
groups. There needs to be a targeted approach to educate, give information and<br />
signpost individuals to the correct service. The Choose Well campaign, launched<br />
nationally and locally should address some of these issues; increasing patients<br />
awareness of where to go to for the right treatment and also publicising the location,<br />
opening times and services offered in these centres. This, however, is only useful for<br />
those who can read English.<br />
The following recommendations were made with consideration to the findings from<br />
the new arrivals engagement:<br />
• work in partnership with the New Arrival Strategy group and deliver targeted<br />
campaigns to address the issues.<br />
• work on an ongoing basis with educational intuitions to create a better<br />
understanding particularly amongst International students.<br />
• promote the message that pharmacy services are available on the high street<br />
and can give people expert, confidential advice and treatment for a wide<br />
range of minor illnesses and ailments, without having to wait for an<br />
appointment.<br />
Decisions made<br />
Work is ongoing to ensure new arrivals to the city receive the most appropriate<br />
information about accessing health care services. The report of the findings was fed<br />
back to the New Arrivals Strategy group and the marketing department to use as a<br />
basis for developing a new, more targeted Choose Well campaign.<br />
56
Out of Hours Service<br />
What was the issue?<br />
NHS Leicester City’s Quality Directorate needed to review the out-of-hours service<br />
and monitor improvements to patient’s experience. There had previously been a low<br />
response rate to questionnaires sent to the homes of patients after being seen. It<br />
was then decided that a team would interview patients after using the service to<br />
analyse their experience and observe the process during a visit to one of the out-ofhour<br />
options, an Urgent Care Centre, next to Leicester Royal Infirmary’s A&E unit.<br />
Who was consulted?<br />
Staff from NHS Leicester City attended the city Urgent Care Centre unannounced to<br />
interview service users on a one-to-one basis. This was done on three occasions,<br />
one being a Saturday.<br />
What information was given?<br />
Patients were told who the team were, where they were from and that the service<br />
review was an inspection to suggest improvements, and had not been undertaken<br />
with the intention of closing the centre.<br />
What were people asked to comment on?<br />
Seven broad questions were identified, with the option for the patient to identify key<br />
words in relation to each question:<br />
• Booking/ arriving for appointment<br />
• Information at reception<br />
• Waiting time to see doctor/ nurse<br />
• Meeting with doctor/ nurse Treatment offered<br />
• Information given about condition<br />
• Information given about follow up<br />
They were then given an opportunity to give reasons why and comment on any other<br />
aspect of the service.<br />
The result was that patients were able to give NHS Leicester City staff an overall<br />
snapshot view of their experiences.<br />
Summary of feedback<br />
The following concerns and improvements were suggested for the service to<br />
improve:<br />
• approximate waiting times need to be available<br />
• the Jayex digital messaging display board could be used to show useful<br />
telephone numbers and health messages<br />
• provide Department of Health information on why prescriptions may not be<br />
the most appropriate treatment in the leaflet stand<br />
• provide NHS and trust magazines on information stand<br />
• provide a water cooler or information about where to get a drink of water<br />
• provide fans to ensure that the environment is comfortable for patients<br />
• have televisions or other media available to reduce ‘boredom’<br />
• provide directions to a vending machine nearby<br />
• provide a static information display board for the waiting area<br />
57
• can there be signs saying if there are any problems to report them to<br />
reception?<br />
• chlamydia tests could be available in the toilets<br />
• better communication to patients for why you are testing or treating them,<br />
especially where there are language barriers<br />
• have alternative methods for printing off information if patients request it<br />
• ensure that information is displayed to inform patients and carers how they<br />
can make a complaint<br />
• the notice board in the corridor outside the Urgent Care Centre was very<br />
crowded and it was difficult to read some of the notices – this needs to be<br />
regularly checked and updated<br />
• maintain a comfortable temperature in the facilities<br />
• ensure that the board at reception displaying which staff were on duty is<br />
accurate each day.<br />
Decisions made<br />
Many of the suggestions have already been adopted and the others are being<br />
investigated for the best possible solutions to improve the patient experience as part<br />
of a wider overall review of A&E, unscheduled and urgent care.<br />
58
Patient Participation Group event<br />
What was the issue?<br />
A Patient Participation Group (PPG) is a practice-based forum, which involves<br />
patient representatives and practice staff, who meet to contribute to the improvement<br />
of their GP services. The role of the group is to work together with the practice to<br />
improve services for patients and support good practice development. People who<br />
are involved with PPGs have said that they feel really involved and understand much<br />
more about how their views and feedback help to improve things for patients and<br />
service users.<br />
In Leicester City, although a growing number of GP practices now have a PPG in<br />
place, there are still many practices which have asked for support in setting up and<br />
running a successful PPG. A number of existing PPG members also asked for<br />
support with networking with other PPGs.<br />
In winter 2010 NHS Leicester City organised a public event to raise the profile of<br />
PPGs, to encourage practice managers, GPs and members of the public to set up<br />
new ones and to share ideas and best practice with those that already existed.<br />
Who was consulted?<br />
GPs, practice managers, PPG chairs and members of the public were invited to<br />
attend.<br />
What information was given?<br />
Presentations at the event outlined the purpose of a PPG, how to structure the group<br />
and recruit to ensure demographic representation. There were also presentations<br />
from local practices and patients who are part of PPGs who shared new ideas and<br />
best practice.<br />
What were people asked to comment on?<br />
The event gave attendees the opportunity to network with other PPG members and<br />
practices whilst encouraging questions from tables. A workshop session encouraged<br />
attendees to share ideas with topics of starting a PPG, health promotion, and<br />
planning for the future.<br />
Summary of feedback<br />
Feedback from the event highlighted the need for improved communication between<br />
the Trust and PPGs with individuals asking for further information regarding setting<br />
up and running a successful PPG. There were many comments made asking for<br />
advice on how to handle difficult situations (such as complaints from patients and<br />
individual members) and comments were made on the design of the current<br />
information booklet with suggestions of how to make it more visually appealing.<br />
Through examination of the evaluation forms, most attendees found the session to<br />
be very informative, with the networking opportunity as the most valuable element.<br />
Decisions made<br />
One of the outcomes from the event is that the Local Involvement Network (LINk) is<br />
now working to establish a PPG forum to offer consistent support to PPG Chairs and<br />
Practice Managers in the city. In addition a number of attendees expressed interest<br />
in starting their own PPGs and we are working to support them.<br />
59
Sexual health website<br />
What was the issue?<br />
The public health team wanted to develop a website that would be meaningful to all<br />
ages and cultures using the internet to be informative and cover all aspects of sexual<br />
health of interest to the residents of Leicester City. This is one of many approaches<br />
the public health team have been using to contact communities across the city.<br />
A key issue was that there are many different preferences in design and language<br />
between different cultures and members of those cultures, including differences<br />
between various target group members, depending on their gender, age and their<br />
sexual orientation or religion, among other social and cultural factors.<br />
Who was consulted?<br />
A ‘scatter-gun’ approach of the membership was chosen to select 50 people who<br />
were from a range of different backgrounds. We also engaged with various<br />
community organisations and groups to feedback information on specific preferences<br />
and examined evidence from previous research on preferences for both sexual<br />
health information, language and website design.<br />
What information was given?<br />
People were informed of the website proposition and purpose, and they were asked<br />
to review the proposed information pages and the website design. Members of our<br />
NHS trust membership scheme with online access were sent links to similar<br />
websites, to help them decide what styles they liked or disliked. They were also<br />
informed that, although it would not be possible for them to be identified through the<br />
process, their equality data was needed for the team to analyse what issues affected<br />
which cultures.<br />
What were people asked to comment on?<br />
A simple questionnaire was designed for residents to comment on the information<br />
they wanted, the language they wanted, the website to use, the website design<br />
preferred and any other comments or concerns they had. They were also asked to<br />
feedback their equality information, but it was emphasised that this information would<br />
not be used to identify them, and it was only necessary to analyse which<br />
communities had particular issues or preferences to better inform the project’s<br />
approach.<br />
Summary of feedback<br />
People gave comments on topics they wanted to see, the layout preference, their<br />
preferred language, with explanations of why some words were inappropriate to their<br />
community and what other features they wanted to see on the website.<br />
Decisions made<br />
The feedback is currently being used as a basis for the website development taking<br />
into account all the concerns and additional interests of the different communities.<br />
60
Part 3: Leicestershire County and Rutland<br />
engagements<br />
61
Bowel cancer and bowel cancer screening awareness<br />
What was the issue?<br />
To inform a social marketing campaign aimed at raising awareness of the symptoms<br />
of bowel cancer, and the uptake of the bowel cancer screening programme.<br />
Who was consulted?<br />
The campaign was focused on ‘seldom heard’ groups and people from areas of<br />
health inequality. Six focus groups were held with people from Charnwood and North<br />
West Leicestershire, including people from a BME background.<br />
What information was given?<br />
Questionnaires were sent to people in the membership scheme in older age<br />
brackets, and to members from a BME background to gain an understanding of their<br />
awareness of bowel cancer symptoms and the screening programme.<br />
What were people asked to comment on?<br />
People were asked questions about the symptoms of bowel cancer and whether they<br />
would seek medical advice. They were also asked if they were aware of a bowel<br />
screening programme and how confident they felt in the ability of screening to detect<br />
early symptoms of bowel cancer.<br />
At the focus groups information to be gained included:<br />
• what they knew about what effect bowel cancer has, and what it can lead to<br />
• what they knew about treatments for bowel cancer<br />
• what they knew about the symptoms of bowel cancer<br />
• what they knew about the test for bowel cancer (including showing them what<br />
they would receive if invited to take the test)<br />
• what were the barriers to them taking the test, if any<br />
• what would encourage/facilitate them to take the test<br />
• what were the barriers to them sharing suspicious symptoms with their GP.<br />
Summary of feedback<br />
More than 2,000 people completed the questionnaires. Six focus group sessions<br />
took place and all feedback was collated. The feedback showed that more<br />
interventions were needed to improve awareness of symptoms to encourage so that<br />
people realised the importance of bowel screening. It also showed that people were<br />
more likely to take part in the screening process if their GP contacted them about it.<br />
Decisions made<br />
The results of the focus groups and questionnaires have been used as insight to<br />
inform decisions about interventions to improve awareness of symptoms, and<br />
increase uptake of screening in at risk groups. A social marketing campaign has<br />
taken place including posters, radio, TV and bus advertising to increase awareness<br />
of the symptoms and the value of screening and including GPs contacting individual<br />
patients and asking them to take part in the screening process.. Further research<br />
planned in 2011 will evaluate the success of the campaign.<br />
62
Dental access<br />
What was the issue?<br />
People were not taking up available dental appointments that had been made<br />
available following public feedback saying they could not get a dental appointment.<br />
Therefore an event was arranged to inform the public of the importance of dental<br />
health and to engage with them on dental access.<br />
Who was consulted?<br />
Members of the public living in areas of high health and social deprivation<br />
What information was given?<br />
A public health specialist registrar and a practicing dentist spoke on the following:<br />
• importance of eating healthy food to keep teeth healthy.<br />
• negative effects of poor dental hygiene.<br />
• Self-help tips on what you can do at home to prevent tooth decay, infection<br />
and cavities.<br />
• NHS dental charges.<br />
A video was shown on how looking after your teeth from an early age can help<br />
prevent painful dental problems, such as abscesses.<br />
People attending then took part in a quiz to assess their understanding of the<br />
information given.<br />
What were people asked to comment on?<br />
A question and answer session took place where people could pose questions<br />
directly to the experts.<br />
Summary of feedback<br />
People felt better informed and aware that they could access dental appointments<br />
Decisions made<br />
To repeat this event annually.<br />
63
Health care for older people, patients and carers<br />
What was the issue?<br />
An event was organised to address feedback from the NHS Leicestershire County<br />
and Rutland’s “Be Healthy, Be Heard” membership scheme. Members felt that many<br />
people suffer with dementia, Alzheimer’s and Parkinson’s in particular, and wanted<br />
to learn more. In September, when the event was held, it was also Older Person’s<br />
Month, a celebration of older people involving a range of events organised by the<br />
public, private and voluntary sectors.<br />
Who was consulted?<br />
“Be Healthy, Be Heard” members and members from NHS organisations across<br />
Leicester, Leicestershire and Rutland, along with volunteer organisations such as<br />
LINks and Carers Action and the Neurological Associations.<br />
What information was given?<br />
Presentations were given on Alzheimer’s, Parkinson’s, and arthritis. After the<br />
presentations, the attendees had an opportunity to take part in a seated exercise and<br />
a ‘laughter yoga’ session.<br />
What were people asked to comment on?<br />
Following each presentation members of the audience were given the opportunity to<br />
ask questions. They were also asked to complete an evaluation form to assess the<br />
success of the event.<br />
Summary of evaluation feedback<br />
In all, 56 people attended. Attendees enjoyed the event and felt it was `excellent in<br />
all respects’. The presentations received a very good rating as the audience felt their<br />
needs had been addressed. Members of the audience also stated that they would<br />
have preferred more time for each topic.<br />
The aims of the event were achieved. Attendees felt more informed of the symptoms<br />
and prognosis of the conditions and felt motivated to discuss with their peers,<br />
friends, families and colleagues. Following the exercise participation sessions,<br />
attendees felt they could take away the simple and effective exercises they had been<br />
shown and continue at home.<br />
Decisions made<br />
To do more individual topic-specific events such as this one.<br />
64
Loughborough University health and wellbeing event<br />
What was the issue?<br />
The vent aims were to:<br />
• to encourage staff to consider the importance of their own health<br />
• to pick up risk areas for individuals via screening and offer direction to<br />
services to minimise this risk<br />
• to raise awareness of current, relevant cultural health issues<br />
• to promote staff feeling supported and cared for in their working environment<br />
• to maximise uptake of good services available within the university community<br />
and Charnwood region.<br />
Who was consulted?<br />
University staff were invited to attend via notifications on online notice-boards,<br />
newsletters and signage in communal staff areas. Reminders and requests to<br />
promote attendance were sent to heads of departments, sections and administrators<br />
to encourage staff to feel supported in attending by their managers.<br />
What information was given?<br />
Approximately 10 different organisations attended to give information on healthy<br />
lifestyles including the NHS Leicestershire County and Rutland.<br />
Summary of feedback<br />
In all, 220 members of staff attended the event. This was a very useful engagement<br />
event as it gave the opportunity to promote key health messages to a hard to reach<br />
group - those who work full time.<br />
Decisions made<br />
A follow-up session has been arranged. This will be appointment based and<br />
specifically focus on the most popular tests cholesterol, blood sugar, blood, pressure<br />
and body weight / composition measures.<br />
65
Membership Consultation<br />
What was the issue?<br />
In March 2009 NHS Leicestershire County and Rutland started a membership<br />
scheme called ‘Be Healthy, Be Heard’. The aim of the membership scheme was to<br />
help the public of Leicestershire and Rutland become as healthy as possible, and to<br />
provide a mechanism for people to feed back their views into the organisation on<br />
policies and service development by taking part in consultations.<br />
The engagement team has also attended a multitude of community events including<br />
farmers’ markets, family wellbeing clinics and events held by charities such as<br />
VISTA and the neurological society.<br />
A number of talks were given throughout the county called “community medicine for<br />
members”. Members attending these talks received up-to-date information and key<br />
health messages from health experts on a variety of topics, such as prostate cancer,<br />
women’s cancers, dental health, diabetes and staying healthy for older people.<br />
A quarterly newsletter delivers key health messages to members and keeps the<br />
members updated on the work of NHS Leicestershire County and Rutland. In each<br />
issue members are invited to give their views by taking part in current consultations,<br />
enter competitions and find out what events are happening in their area.<br />
In November 2010 a membership questionnaire was sent to all members of ‘Be<br />
Healthy, Be Heard’ (almost 10,000 people) to find out if the aims of the membership<br />
scheme were being achieved.<br />
What were people asked to comment on?<br />
The questionnaire invited responses to the following statements:<br />
• being a member has helped me to be more healthy and to feel better<br />
• as a member I have felt more informed about ways to stay healthy<br />
• as a member I have had the opportunity to feedback on health services, for<br />
example, the opportunity to feedback my concerns about any proposed<br />
changes, and how I would like services to look in the future.<br />
• I find the information I receive as a member easy to understand<br />
• I find the information I receive as a member interesting<br />
• I would like to see more information on…….<br />
• one suggestion I would like to make on how to improve Healthy Times the<br />
membership newsletter is ……..<br />
Summary of feedback<br />
When considering the aims of starting the ‘Be Healthy, Be Heard‘ membership<br />
scheme the results of the membership questionnaire indicate that the membership is<br />
indeed helping members to be more healthy and has given people a mechanism to<br />
feed back their views into the organisation.<br />
Over 50% of respondents agreed that being a member has helped them to be more<br />
healthy and feel better. Over 80% of respondents feel more informed about ways to<br />
stay healthy. More than 80% of respondents also agreed that membership gave<br />
them the opportunity to feed back their views and over 94% agreed that the<br />
66
information was easy to understand, along with over 85% of respondents agreeing<br />
that the information was interesting.<br />
The comments have provided a rich source of information on topics members would<br />
like to know more about and reflects the findings of the quantitative analysis. We<br />
have already begun to use this information in the planning of articles for our<br />
newsletters and in the planning of future events. For example, we have already held<br />
an event on dementia and have an event planned in the spring on how to navigate<br />
your way through the NHS.<br />
The demographics of our membership reflect that we have a representative<br />
membership including members from seldom heard groups such as people with<br />
physical disabilities, people with learning disabilities, older people and people from<br />
areas of high social and economic deprivation. The ‘Be Healthy, Be Heard’ brand is<br />
recognised and trusted in the community. We know this by the feedback we receive<br />
from the public at community events and by the number of invitations we now<br />
receive to attend community events. We always receive a good response from our<br />
members to all of our surveys. We are also aware that some of our members are<br />
eager to become more involved and are interested in becoming member volunteers.<br />
We also have over 100 corporate members and are currently working together to<br />
improve occupational health.<br />
We can therefore conclude that the NHS Leicestershire County and Rutland<br />
membership scheme is a successful scheme that engages with a large number of<br />
people from all walks of life, helping them to become healthier, be more informed<br />
and have a voice of influence in the decision making process for our organisation. In<br />
the future we hope to develop the scheme further as the membership along with our<br />
seldom heard strategy gives NHS Leicestershire County and Rutland a robust and<br />
meaningful way to engage with the public.<br />
Decisions made<br />
NHS LCR will continue to have a membership and recommend it to our CCGs for<br />
future engagement and consultations. We also plan to stage some of the events<br />
suggested by members.<br />
67
Pacesetters Bowel Cancer Screening Awareness Project<br />
What was the issue?<br />
The NHS Pacesetters Bowel Cancer project was established to increase awareness<br />
of bowel cancer and the NHS bowel cancer screening programme amongst the<br />
South East Asian community in North West Leicestershire and Charnwood.<br />
Bowel cancer is the third most common cancer in the UK and the second most<br />
common cause of cancer death. It has been particularly noted that there is poor<br />
uptake of cancer screening programmes by Black and Minority Ethnic groups. There<br />
is a clear need to reduce the barriers to screening by raising awareness and<br />
increasing access through culturally sensitive and community based interventions.<br />
Pacesetters is a national programme that encourages the involvement of local<br />
communities The importance of community engagement and consultation was<br />
central to the successful delivery of this project. This provided an opportunity to<br />
increase community awareness of bowel cancer screening and also to enable<br />
identification of the barriers to participating in the screening programme. This project<br />
involved attending a Well Family Clinic multi-agency event and also a series of Asian<br />
elders focus groups.<br />
Who was consulted? And what information was given?<br />
There were three events:<br />
• Well Family Clinic Event<br />
Attendance at this multi-agency session provided an opportunity to engage in<br />
a general health event in an effort to promote bowel cancer awareness and<br />
the screening programme. The plan was to ascertain baseline information<br />
about the knowledge of bowel cancer and the bowel cancer screening<br />
programme from the individuals attending the ‘clinic’. A questionnaire was<br />
used to collect this information and on completion a discussion was held with<br />
the individual based on the responses given.<br />
The Well Family Clinic was well attended, with 70 participants overall. 29<br />
individuals approached the bowel cancer screening stand, in a very busy<br />
multi-agency ‘clinic’ with numerous displays, and illustrates the difficulty in<br />
reaching all attendees at a general health awareness event. This consolidated<br />
the decision to hold a single, focussed event and in doing so, highlighted the<br />
need to consult the South East Asian community.<br />
This consolidated the decision to hold a single, focussed event and in doing<br />
so, highlighted the need to consult the South East Asian community.<br />
• Asian Elders Focus Groups<br />
Six focus group sessions were held with Asian elders. This helped raise<br />
awareness of bowel cancer screening by identifying community knowledge of<br />
bowel cancer signs and symptoms, the risk factors for bowel cancer and the<br />
NHS bowel cancer screening programme. The barriers to participating in<br />
screening were discussed and the discussions suggested that the main<br />
barrier within this community was lack of awareness of the screening<br />
68
programme. The focus groups helped to shape the development of the final<br />
event by highlighting the activities that would encourage participants to attend.<br />
When it came to naming the project and final event, there was unanimous<br />
agreement within the focus groups (approximately 110 individuals) that we<br />
should avoid using a ‘strap-line’ for the project as this was seen as having a<br />
hidden agenda. It was felt that advertising the event as an ‘NHS Bowel<br />
Cancer Awareness Event’ was more transparent.<br />
• Bowel Cancer Awareness Event<br />
The aim of the day was to raise awareness of bowel cancer and of the NHS<br />
bowel cancer screening programme. There were presentations on bowel<br />
cancer, the NHS screening programme and diet and a healthy bowel. A<br />
highlight of the event was a presentation from a service user perspective that<br />
was delivered in Gujarati.<br />
A series of activities were delivered, based on the suggestions from the earlier<br />
focus groups: two vegetarian cooking demonstrations, smoothie making, yoga<br />
sessions, chair exercises and health screening (blood pressure and body<br />
mass index calculation). Attendees also had the opportunity to have a private<br />
consultation about bowel cancer screening and volunteer to become a<br />
community health champions, The event was attended by 103 individuals<br />
from the South East Asian community.<br />
Summary of feedback<br />
This project highlighted that the South East Asian community in North West<br />
Leicestershire and Charnwood are willing to participate in health events and will<br />
participate in NHS screening programmes if they are aware of the importance of the<br />
programme. Evaluation of the event demonstrated that the methods used in this<br />
project can reach a significant part of a community to deliver health promoting<br />
messages and activities suited to their needs. It was also noted that event was<br />
primarily promoted through local groups, friends and family. This reinforces the<br />
importance of community health champions to promote a health message within<br />
these communities.<br />
Community health champions are the key to sustaining the delivery of health<br />
messages and converting these messages to actions that will result in significant<br />
changes in lifestyle and behaviour. As a result of this project three individuals have<br />
volunteered to train as community champions with a number of interested individuals<br />
requesting further information. It is also hoped that by disseminating this report within<br />
this community further individuals will be encouraged to become community<br />
champions. Ultimately this project has demonstrated that partnership working across<br />
health, social and voluntary agencies can successfully deliver a health improvement<br />
message to a South East Asian community.<br />
Decisions made<br />
Knowledge and awareness of bowel cancer screening is a barrier to screening<br />
uptake. Information needs to be provided to communities in a format that is easily<br />
accessible and understood. The focus groups indicated quite strongly that the<br />
General Practitioner should be involved in this process of raising awareness of the<br />
bowel cancer screening programme, promoting it to eligible patients and<br />
encouraging participation.<br />
69
The report will be used to inform the Countywide project working with General<br />
Practice to improve cancer awareness and promote screening to support early<br />
diagnosis.<br />
70
Patient experience<br />
What was the issue?<br />
The aim was to gather a range of quantitative data provided by patients while also<br />
identifying some questions about the equality and diversity issues facing patients<br />
and carers. This information was gathered to inform the NHS Leicestershire and<br />
Rutland Patient Experience Strategy 2010-13. Also, information gathered would help<br />
the organisation to understand the needs, expectations and preferences of the<br />
public.<br />
Who was consulted?<br />
Members of the <strong>PCT</strong>’s membership scheme “Be Healthy, Be Heard”.<br />
What information was given?<br />
People were informed of progress made in responding to the experience of local<br />
patients and how this was currently assessed through Patient Advice Liaison Service<br />
(PALS), complaints, comments and compliments, patient safety incidents and patient<br />
experience surveys. Members were informed on how their feedback would be used.<br />
What were people asked to comment on?<br />
People were asked about their experiences either as a patient; using the services or<br />
as a carer of someone using the services. People were also asked to consider<br />
recent experience and what they believed would make future experiences better.<br />
Summary of feedback<br />
Fifty people responded to the questionnaire. Taking the feedback into consideration<br />
the Patient Experience Strategy was developed.<br />
Decisions made<br />
The Patient Experience Strategy was approved by the Trust Board and is now being<br />
implemented by the Quality Directorate.<br />
71
Perinatal psychosis<br />
What was the issue?<br />
The aim was to understand the views of women of childbearing age about services<br />
for perinatal psychosis, in order to create an East Midlands-wide specialised mother<br />
and baby mental health service.<br />
Who was consulted?<br />
Women of childbearing age were selected from the membership database and<br />
asked for their feedback. Two meetings of BME women in Loughborough were also<br />
asked their views.<br />
What information was given?<br />
Documentation explained plans for caring for women who become mentally ill before<br />
or following the birth of a baby. It covered plans for the whole of the East Midlands,<br />
including Leicester, Leicestershire and Rutland. The information was followed by a<br />
short questionnaire, to feedback views on these plans.<br />
Perinatal psychosis was also explained along with a description of current service<br />
provision for those who became ill.<br />
What were people asked to comment on?<br />
People were asked where they would prefer to go to if they needed to go to hospital<br />
with mental health problems after having a baby. They were asked if they felt they<br />
would be able to approach health professionals on any mental health issues they<br />
may experience during pregnancy or following the birth of their child. People were<br />
asked to give reasons if they felt they could not approach a health professional.<br />
Views on how to improve awareness on mental health services were also asked for.<br />
Summary of feedback<br />
More than 50 women responded. All of women answered that they would prefer to<br />
go to a local mother and baby unit with their baby, if they needed mental health care,<br />
and 89% said they would be able to talk to a health professional.<br />
Feedback collected from the BME women’s groups included:<br />
• more information needed from the doctors or midwives – the information is<br />
unsuitable to the audience as the information given is too complicated<br />
• need for interpreters<br />
• time spent with doctor or midwife is limited<br />
• did not know what mental health was – it needs explaining by the midwife<br />
• maybe midwife needs to take more of a role in looking for changes – possibly<br />
have more appointments<br />
• accessing information at home, eg, the internet<br />
• leaflets that can be taken away, and which can be translated<br />
• post-natal classes to provide support.<br />
• need parenting classes or support classes to make sure they are aware of<br />
what is available to them and how to do things correctly<br />
• most new mums not sure of what to do in terms of good diet, creating a<br />
routine, feeding, etc<br />
• need to learn about planning a routine, balancing old life with new<br />
• help with how to include mothers’ partners<br />
72
• language and other barriers – midwifes and doctors do not understand the<br />
religious side or culture sufficiently<br />
• current leaflets are too complicated to read.<br />
Decisions made<br />
The results will help with planning for treatment of women with perinatal mental<br />
health issues in the East Midlands, particularly those from a BME background. All<br />
those who took part in the consultation process were informed that this is what their<br />
feedback would be used for.<br />
73
Public Consultation on the proposed closing of Ketton and<br />
Gretton branch surgeries by Uppingham General Practice<br />
What was the issue<br />
Uppingham GP practice approached the NHS Leicestershire County and Rutland<br />
Primary Care Panel with a request to close down the Uppingham GP practice branch<br />
surgeries at Ketton and Gretton.<br />
Who was consulted?<br />
All patients who attend the Ketton and Gretton surgeries received a questionnaire to<br />
share their views and were also offered the option to complete the questionnaire<br />
online at the NHS LCR website or at the Uppingham practice website. They were<br />
also invited to attend one of three public meetings taking place in Ketton and Gretton<br />
to find out more and share their views with NHS LCR and the practice GPs.<br />
What information was given?<br />
Information given included how many patients registered at Uppingham surgery lived<br />
in Gretton and Ketton and surrounding villages.<br />
What were people asked to comment on?<br />
People were asked if they accessed care in other places and what would they<br />
believed would change if the surgery closed. They were also asked to comment on<br />
benefits to them if the surgery closed, how often they had visited the surgery in the<br />
last 12 months, where the usually attended if they wished to see a GP, where they<br />
usually attended if they wished to see a nurse, if they had any objections to the<br />
closure of their branch surgery and the reasons for those objections. Over 250<br />
questionnaires were completed.<br />
Summary of feedback<br />
The feedback focused mainly on issues of access if patients needed to go in to<br />
Uppingham to see a doctor. There were also useful suggestions from both Ketton<br />
Parish Council and Corby Borough Council with regard to how to progress.<br />
Decisions made<br />
Once all feedback had been collated and considered the NHS LCR Trust Board on<br />
the recommendation of the NHS LCR Primary Care Panel was to keep Gretton<br />
branch surgery open.<br />
As requested by Ketton Parish Council the board gave a three-month period for<br />
suitable, alternative accommodation to be sought so that Uppingham branch<br />
surgery may remain open.<br />
74
Smoking, diabetes and eyes event<br />
What was the issue?<br />
To raise awareness of the effects of smoking with particular reference to diabetes.<br />
Also, to discuss eye disease in general and in relation to diabetes.<br />
Who was consulted?<br />
Members of the public were invited to attend an engagement event.<br />
What information was given?<br />
Before the event talks started members of the audience were asked to complete a<br />
questionnaire to assess their knowledge of the subjects to be talked about.<br />
Presentations were given on diabetes by the Deputy Director of Public Health for<br />
NHS Leicestershire County and Rutland, on eyes by an optometrist, and on the<br />
effects of smoking on health by a smoking cessation specialist for the <strong>PCT</strong>.<br />
What were people asked to comment on?<br />
Following each speaker members of the audience were invited to ask questions of<br />
the experts to improve their understanding.<br />
Summary of feedback<br />
Members were asked to complete an evaluation questionnaire following the<br />
presentations. In all, 100% of the audience stated that they were now better<br />
informed.<br />
Decisions made<br />
To continue to engage people through this type of event to keep people better<br />
informed on key health topics<br />
75
Women’s Cancer Event<br />
What was the issue?<br />
The aim was to raise awareness of women’s cancers.<br />
Who was consulted?<br />
Members of the “Be Healthy Be Heard” <strong>PCT</strong> membership scheme were invited to<br />
attend along with members from University Hospitals of Leicester NHS Trust; NHS<br />
Leicestershire Partnership Trust and NHS Leicester City.<br />
What information was given?<br />
Speakers presented on ovarian and cervical cancer, cervical screening, background<br />
to cancer research, current research trials for women’s cancers and genetics.<br />
What were people asked to comment on?<br />
Following each presentation women were encouraged to ask questions and the<br />
health specialists answered.<br />
Summary of feedback<br />
This was a successful engagement event which informed women about women’s<br />
cancers and emphasises the importance of early intervention.<br />
Decisions made<br />
The women enjoyed the event and gave very positive feedback finding the<br />
information given informative and useful. Therefore a similar event will be repeated<br />
in the future.<br />
76
Part 4: East Midlands Specialised<br />
Commissioning Group (EMSCG) engagements<br />
East Midlands Specialised Commissioning Group is an organisation hosted by NHS<br />
Leicestershire County and Rutland.<br />
77
Introduction<br />
The EMSCG is committed to ensuring it is accountable for the decisions it takes on<br />
behalf of the people of the East Midlands and uses patient feedback and proactive<br />
patient and user involvement as an integral part of service review and service<br />
redesign.<br />
We have Lay Members on our Board who provide the voice of the public and we<br />
engage with a variety of individual patients and patient groups to ensure the needs of<br />
patients are considered in all we do.<br />
As well as undertaking our own engagement and consultation we support national<br />
initiatives. A national review of children’s congenital heart services is being<br />
undertaken (Please visit www.specialisedservices.nhs.uk/safe_sustainable/<br />
childrens-congenital-cardiac-services). The review is being led by the national Safe<br />
and Sustainable team on behalf of the 10 Specialised Commissioning Groups and<br />
their constituent Primary Care Trusts, and the EMSCG works hard at a regional level<br />
in support of the associated public consultations.<br />
78
Foreword<br />
Julia Cons<br />
“It has been fascinating to be a part of the work of the EMSCG. More importantly, it<br />
has been a privilege to be involved in the guidance of this highly proficient<br />
organisation, particularly in these times of great change. Every person with whom<br />
I’ve had professional contact has been visibly motivated and passionate about the<br />
NHS. Each individual member of staff so obviously understands the imperative to<br />
provide the best possible care to the most possible patients under ever tighter<br />
budgetary constraints, and works hard to add their utmost to the process.<br />
“I have attended EMSCG board meetings and Clinical Priorities Advisory Group<br />
(CPAG) meetings, where my opinions and input have been actively sought and<br />
valued, both as an individual and a representative of the ‘man in the street’. It has<br />
been impressive to be made to feel no less valued on the rare occasion when I have<br />
felt the need to metaphorically bang the table than when high praise has been due or<br />
decisions have been straightforward and courses of action obvious.<br />
“I was also actively involved in the designation process for the genetics services in<br />
the East Midlands, taking part in site visits and staff interviews in Nottingham and<br />
Leicester, where I was able to ask questions to help ensure that the services provide<br />
the best possible service from the point of view of patients and carers.<br />
“During the early part of 2010 I was a member of the team that peer reviewed the<br />
burn care services in Birmingham, Nottingham and Leicester, taking part in all-day<br />
visits to each service and reviewing the information and services provided. I was<br />
hugely impressed by the care in all of the services, by the obvious dedication of the<br />
staff, and by the positive views of the patients. It was gratifying to receive such a<br />
warm welcome at each hospital, and to be provided with such comprehensive<br />
information to demonstrate their compliance - and more - with the Burn Care<br />
Standards. I was so impressed with the provision of burn care in the Midlands that I<br />
was thrilled to be asked to join the Midlands Burn Care Network as a lay member,<br />
and to be invited to be a member of a national team who are currently reviewing the<br />
Burn Care Standards.<br />
“The last year has been most rewarding. I hope I have added as much - preferably<br />
more – to the organisation and the NHS, and I look forward to being an active part of<br />
the EMSCG in the coming months.”<br />
Lee Bartholomew<br />
As well as involvement in the EMSCG Board and Clinical Priorities Advisory Group,<br />
EMSCG Lay Advisor, Lee Bartholomew was invited to Chair the Project Board for<br />
the National Haemoglobinopathies Project. This one year project to define the<br />
designation standards model service specification and commissioning framework for<br />
Sickle Cell Disease and Thalassaemia.<br />
Lee said “I have found the work of the Project Board a fascinating insight into the<br />
challenges faced by patients, providers and commissioners. The efforts the Project<br />
Team has made to consult as widely as possible with the stakeholders are to be<br />
commended. I am sure their efforts will produce an invaluable set of tools for the<br />
health community to use.”<br />
79
Teenage and Young Adults Cancer (TYA)<br />
Why?<br />
To ensure that the East Midlands service meets the needs of teenagers and young<br />
adults, the EMSCG involved patients in developing and improving the service.<br />
What did we do?<br />
We sought patients’ views and suggestions on:<br />
• Current service provision<br />
• How the service can change to incorporate both the medical model and<br />
psychosocial model of care<br />
• Improvements for physical facilities (to ensure the hospital surroundings<br />
stimulate and motivate teenage/young adult cancer patients).<br />
This was achieved in a variety of ways including:<br />
• Informal discussions at youth groups in order to build trust enabling patients to<br />
share their experience of the diagnosis, treatment and hospital care<br />
• A user experience questionnaire which provided a confidential method for<br />
capturing experiences of patients and assisted in understanding things from a<br />
patient perspective.<br />
• A media campaign, newsletters, direct mail and business card distribution,<br />
providing a comments book for thoughts, posters, and work with clinical teams<br />
to encourage them to seek feedback on patient views.<br />
Some of the key issues identified were the need for:<br />
• A quicker referral from GP to the acute sector and the early identification of<br />
TYA patients<br />
• Improvements in communication i.e. in the explanation and understanding of<br />
diagnosis, treatment and consent to treatment<br />
• Psychosocial support services that meet specific age group needs, such as<br />
alone time, access to peer support, support relating to feelings of isolation,<br />
fear and motivation<br />
• Information on health care needs - body image, puberty, diet, health<br />
promotion, pathway journey<br />
• Good facilities with choice, a contact person and a care plan<br />
• Access to outreach support, moving on back in the community.<br />
What was the impact?<br />
The following actions were taken forward:<br />
• Update our policy with the responsibilities of the key worker role, ensuring the<br />
role is managed and service allocated according to patient need at the TYA<br />
multi-disciplinary meeting<br />
• Develop an information leaflet for patients and a communication and<br />
marketing plan to raise awareness of the service amongst patients and<br />
clinicians<br />
• Ensure age appropriate facilities incorporate patient requirements: i.e. the<br />
look of the building and provision of specific facilities including a<br />
complementary therapy room, WIFI access, area for space and education<br />
• Develop specialist posts such as the TYA Childrens Nurse Specialist (CNS)<br />
role to provide outreach support.<br />
80
East Midlands Renal Network (EMRN)<br />
Patient and Carer Forum<br />
The EMSCG hosts the East Midlands Renal Network and provides specialised<br />
commissioning expertise to assist the Network in their aim to continually improve<br />
kidney care for patients and carers living with kidney disease. During 2011 the East<br />
Midlands Renal Network established a Patient and Carer Forum.<br />
Why?<br />
The renal network believes that patient and carer involvement is integral to the work<br />
of the network to ensure services are patient focused. The main purpose of the<br />
group is to provide the Renal Network with a perspective of the quality and<br />
experience of care from the viewpoint of patient and carers.<br />
The basis of the forum is that there is always a story to be told from an experience<br />
and we focus on how the Network can best tell that story in a way that others can<br />
learn from and users can benefit from.<br />
What did we do?<br />
Information about the East Midlands Renal Network and the proposed patient and<br />
carer forum was circulated liberally around renal dialysis units, local kidney patient<br />
associations and other relevant areas. This information asked for expressions of<br />
interests to joint the group. Further information was then provided and the first<br />
meeting took place. Meeting are held every 3-4 months.<br />
What was the impact?<br />
The forum is in its infancy and is working on ideas for assessing renal units from a<br />
patient and carer perspective. The forum provides a means of gaining patient and<br />
carer input in policy/guidelines development and service improvement initiatives.<br />
One quote was provided to the network manager in an e-mail following one of its<br />
meeting as follows;<br />
“I think the forum will do a great job in making the units all work as one and bringing<br />
them all to a certain high standard to give the patients peace of mind that they are<br />
getting the best.”<br />
(Patient: EMRN Patient and Carer Forum).<br />
81
Midland Burn Care Network (MBCN)<br />
Why?<br />
To understand the needs of those that use the burns services in the East Midlands.<br />
What did we do?<br />
The MBCN has continued to develop patient surveys. The MBCN team has also<br />
developed a website which provides a means of providing information on burn care<br />
to the local the population. Results from the patient surveys and comments from<br />
patients are available from: www.midlandsburnnetwork.nhs.uk<br />
What was the impact?<br />
The development and participation of patients completing surveys has had a positive<br />
impact on Burns services in the East Midlands. Patient experience has been<br />
improved in the Dressing Clinic / Outpatient departments after patient feedback.<br />
Length of time for appointments has been slightly increased and this has led to more<br />
patients reporting that they have been seen on time. There has been an increase in<br />
appropriate patients being seen by the Therapy teams. Following patients answering<br />
questions on pain / discomfort actions have been taken to improve patients’ pain<br />
control and the advice given on analgesic medication. In the most recent survey<br />
patients / carers report an increase in satisfaction with their care.<br />
82
Safe and Sustainable - National Paediatric Congenital<br />
Heart Surgery Review<br />
Why?<br />
To engage patients and their carers in the consultation process of the national<br />
review of children’s heart surgery services and obtain their views on the proposed<br />
service model and configuration options.<br />
What did we do?<br />
Extensive consultation documents and feedback mechanism have been made<br />
available by the national team supported by EMSCG. EMSCG worked with NHS<br />
Lincolnshire to engage with the local populations of Lincoln and Sleaford and have<br />
worked with Leicestershire Links. The engagement culminated in two events held on<br />
16 June attended by around 500 people. As part of the review the National Team<br />
commissioned an independent Health Impact Assessment (HIA). Individual<br />
interviews were held with parents and two events, supported by EMSCG, for hard to<br />
reach and disproportionately affected groups where held in the Belgrave and<br />
Highfields areas of Leicester.<br />
What was the impact?<br />
The views of patients from across the East Midlands have been fed into the<br />
reconfiguration decision making process. An interim HIA has been published and a<br />
report of the responses to the consultation is expected in the last week of August<br />
2011.<br />
83
East Midlands Haemophilia Management Group<br />
Why?<br />
EMSCG facilitated the establishment of the East Midlands Haemophilia Management<br />
Group to allow sharing of expertise and good practice, quality assure and inform<br />
commissioning decisions. This group has multi-professional representation from the<br />
haemophilia centres across the region and includes two patient representatives.<br />
What did we do?<br />
Patients are involved in the discussions and able to influence the decisions of the<br />
group.<br />
What was the impact?<br />
The introduction of a patient contract and a patient education event was held on the<br />
16 March 2011 attended by around 40 patients and their relatives.<br />
84
National Commissioning documents for<br />
Haemoglobinopathy<br />
Why?<br />
The EMSCG were commissioned by the Department of Health to produce a series of<br />
national commissioning documents for haemoglobinopathy services.<br />
What did we do?<br />
Patient group representatives were part of the Expert Working Party which informed<br />
the development of the documents. A patient workshop was help in London with<br />
patients from across the country in attendance.<br />
What was the impact?<br />
Patient views are explicitly represented in the final documents which will be used to<br />
inform the commissioning of local services for patients.<br />
85
Involvement of regional Expert Patient Committees in the<br />
commissioning and development of Specialised Perinatal<br />
Mental Health Services in the East Midlands<br />
Why?<br />
The East Midlands Perinatal Mental Health Clinical Network was set up to improve<br />
the care and treatment of pregnant and postpartum women who are seriously<br />
mentally ill. Working in collaboration with the EMSCG, the key principles of the<br />
Network are to support the development of comprehensive and integrated perinatal<br />
mental health services providing high quality care that meets the needs of mothers<br />
and their infants. Ex-patients have been involved in advising the Network on the<br />
various work programmes that have been set up to support this. From the outset,<br />
patients have actively participated in short life working groups, workshops and<br />
regional conferences.<br />
What did we do?<br />
In 2009, as part of the NHS East Midlands Next Stage Review regional priorities<br />
programme, five Expert Patient Committees were established, one in each mental<br />
health trust. These are now a constituent part of the formal organisational structure<br />
of the Network. The emphasis has been to ensure that, through the Expert Patient<br />
Committees, the views and experiences of service users across the Network are<br />
adequately represented in the planning and implementation of changes in service<br />
provision and delivery for perinatal mental services, taking into account regional and<br />
national initiatives and to give advice and recommendations to the Network<br />
Executive Committee and Management Board.<br />
Over the period April 2010 – March 2011, the Expert Patient Committees have<br />
contributed towards the development of:<br />
• Quality standards for in-patient mother and baby units, perinatal community<br />
psychiatric teams and infant welfare.<br />
• A quality of life measure and care and treatment questionnaire developed by<br />
the Network in conjunction with a clinical software company, FACE<br />
(Functional Analysis of Care Environments).<br />
• Antenatal screening midwifery training programme, incorporating both an e-<br />
learning and tutorial component.<br />
• Regional care pathway and management guidelines.<br />
• Patient information leaflets.<br />
• Research proposals and grants.<br />
What was the impact?<br />
Patient involvement in service redesign/development has had an important impact<br />
on service delivery, as follows:<br />
• Evidence of real patient influence on the Network, with patient representation<br />
on the Network Management Board and Stakeholder Reference Group and<br />
input into all Network work programmes.<br />
• Evidence that recommendations made by the Expert Patient Committees are<br />
integrated into network planning and regional strategic decision-making (i.e.<br />
outcome measures, standards, training).<br />
• Input into the development of quality standards, training programmes and<br />
care pathways, which has led to improvements in:<br />
86
• Clinical practice, skills and decision-making in maternity, psychiatric and<br />
primary care services.<br />
• Management and referral of patients in a timely and efficient manner.<br />
• Promotion of good/best practice in accordance with national guidelines/peerreview;<br />
this has also promoted continuing professional development and<br />
learning.<br />
• Collaborative working between clinicians and an increased capacity for<br />
shared/joint learning.<br />
• Understanding and management of perinatal mental health disorders together<br />
with increased skills and capacity in primary care.<br />
• Emphasis on improving and streamlining the patient journey has helped<br />
ensure rapid access to the most appropriate level of care.<br />
• Development of Patient Related Outcome Measures, which are tailored to the<br />
specific needs of women who are under the care of Specialised Perinatal<br />
Mental Services, enables patients to provide feedback on the quality of<br />
services and provide a self-assessment of their personal situation.<br />
87
Policy Development<br />
The EMSCG draft policies are routinely sent out for engagement with patients and<br />
the public via our regional Primary Care Trusts. Draft policies are also sent to known<br />
patient support/interest groups (national and regional) for comment, and we place<br />
draft policies on our website to give people the opportunity to provide us with their<br />
views. We review our draft policies in light of all the comments we receive, making<br />
changes and amendments where appropriate before a final copy is sent to the Board<br />
for approval. The case study below shows the details of policy consultations.<br />
EMSCG Commissioning Policy for the use of Pre<br />
Implantation Genetic Diagnosis (PGD)<br />
Why?<br />
Pre Implantation Genetic Diagnosis (PGD) enables couples who are at a high risk of<br />
passing a serious genetic disorder to their children, from avoiding the conception of a<br />
child with the genetic disorder (an ‘affected’ child). It uses in vitro fertilisation (IVF) to<br />
create embryos, tests one or two cells from each embryo for a specific genetic<br />
problem and identifies embryos without the genetic problem for transfer to the<br />
uterus.<br />
A revised (second version) of the policy already in existence was proposed, with<br />
changes in access criteria. These were to include the removal of the criteria of ‘no<br />
living unaffected children from their current relationship.’ This would mean that<br />
couples with child/children who had not inherited the genetic condition could still<br />
apply for PGD. The number of IVF cycles would be changed from the first version<br />
which offered ‘three completed’ cycles to an ‘unlimited’ number of cycles instead,<br />
and proposed to allow PGD treatment on the NHS to couples who had previously<br />
paid for the treatment privately.<br />
What did we do?<br />
The policy was posted on the EMSCG website. Leicestershire County and Rutland<br />
(LCR) <strong>PCT</strong> posted a link from their website to EMSCGs, and NHS Leicester City<br />
posted it on their website, on Facebook and Twitter. It was sent electronically with a<br />
plain English Question and Answer paper on June 8 2010 to the interest groups<br />
outlined in ‘Patient Interest/Support Groups’. Responses were received from the<br />
following:<br />
• Association for Improvement in Maternity Services (AIMS)<br />
• The CF Trust<br />
• East Midlands Public Health consultants (3)<br />
• Bassetlaw <strong>PCT</strong><br />
• National Cystic Fibrosis (CF) Trust<br />
• Clinical Genetics, NGH<br />
• Derbyshire county public representative<br />
• Haematology, LRI<br />
• CARE Fertility, Nottingham<br />
• Leicestershire LINk<br />
• IVF patient representative<br />
• FAP Gene Support Group<br />
88
What was the impact?<br />
The following reflects the recurrent themes that arose through the comments that<br />
were received, and the EMSCG response to these:<br />
Comment: “There is Inequity in comparing the criteria for the IVF Tertiary Infertility<br />
policy and the PGD policy”.<br />
Response: The IVF and PGD policy are two separate policies because the IVF<br />
policy is for infertile/subfertile couples, whereas the PGD policy is for fertile couples<br />
and to avoid the risk of having an affected child, not as a necessity to aid them in<br />
conceiving per se. Unlike sub fertile couples, fertile couples could conceive an<br />
affected child. So if tight criteria for access were put in place it could be argued that<br />
the EMSCG endorse an illogical policy because it does not make financial sense.<br />
This is because it may be a false economy not to fund PGD because the costs of<br />
funding an affected child would be far more than paying for PGD.<br />
Comment: “There is concern regarding the unlimited access to PGD, the open<br />
ended access criteria and its links to affordability”.<br />
Response: It would cost the NHS far more to pay for a child affected by a genetic<br />
condition, in comparison to PGD.<br />
PGD in relation to conditions currently not licensed by the HFEA.<br />
Response: The HFEA advises that for practices who are licensed to carry out PGD<br />
and wish to offer PGD for a new genetic condition (i.e. a condition that has not<br />
previously been licensed by the Authority) then they must apply to the Authority to do<br />
so, setting out how they consider the genetic condition in question meets both the<br />
significant risk and seriousness requirements in the HFEA Act (2008).<br />
(http://www.hfea.gov.uk/5259.html).<br />
Comment: “How successful will PGD be?”<br />
Response: Data from the Human Fertilisation and Embryology Authority (HFEA)<br />
shows that in 2006, for women receiving PGD, the percentage of cycles started that<br />
resulted in a live birth was 33.3% for women aged under 35; (9/48) for women aged<br />
between 35-37; and (2/27) for women aged between 38-39. (Percentages are not<br />
calculated where there are less than 50 cycles. Figures in brackets show cycles<br />
resulting in a live birth/all cycles started).<br />
Comment: “The need to consider the child’s welfare statement in the criteria for the<br />
policy is very subjective”.<br />
Response: There needs to be regard to the interest of the potential child (as per the<br />
HFEA Act 1990). However, this has not been classed as ‘mandatory’ criteria in the<br />
policy and these needs have now not been classed as ‘paramount’ as they were in<br />
the previous version – as there is not a ‘test’ to be passed or failed by the presenting<br />
patient.<br />
Comment: “Would PGD for infertile couples be decided under the PGD or IVF<br />
criteria?”<br />
Response: If a couple were subfertile/infertile and were carrier(s)/had a genetic<br />
condition, then the couple would be considered under the IVF criteria. If they met the<br />
criteria under the IVF policy then they would be provided with IVF in accordance with<br />
that policy, whilst allowing them to also have PGD. This will be clarified in the policy<br />
document.<br />
89
Comment: “What happens if the patient has one abandoned cycle?”<br />
Response: Policy has been amended to allow for more than one abandoned cycle.<br />
Comment: “Since some of these inherited conditions are under diagnosed, poorly<br />
understood or insufficiently researched, potentially the policy could discriminate<br />
against these populations.”<br />
Response: There will be equal access to the policy if they meet the clinical criteria,<br />
and the condition is licensed by the HFEA for PGD testing.<br />
Comment: “This policy could increase the risk of multiple births.”<br />
Response: Within the policy, single embryo transfer (SET) will take place so only<br />
one embryo will be transferred.<br />
Amendments made to the final policy as a result of engagement were:<br />
• Clarification within the policy document that couples who are infertile but also<br />
have or carry a genetic condition to be subject to the criteria for IVF as set out<br />
in the tertiary infertility policy, but also provided with PGD for that one cycle if<br />
they meet the IVF tertiary infertility policy.<br />
• Policy amended to delete reference to PGD testing on frozen embryos. The<br />
inclusion of using remaining frozen embryos from self funded IVF in<br />
conjunction with PGD will remain in the policy.<br />
• The policy was amended to allow for more than one abandoned cycle.<br />
• The criteria requirement for a Clinical Pathology (CP) accredited lab amended<br />
within the policy to advise should be working towards CP Accreditation (in line<br />
with the HFEAs 2007 requirements).<br />
• The criteria requirement that ‘the centre must have a HFEA licence to provide<br />
PGD for the condition being considered’, amended as if the lab has a HFEA<br />
license which includes PGD it can test for any of the conditions on the HFEAs<br />
central approved list.<br />
• Clarification on the position on Human Leukocyte Antigen (HLA) matching to<br />
an existing affected child within the policy. Policy amended to include the<br />
position in line with the HFEAs regulations (as per CPAG recommendation<br />
03/09/10).<br />
Patient interest/support groups<br />
• Cystic Fibrosis Trust (national)<br />
• Cystic Fibrosis Trust (regional)*<br />
• Familial Adenomatous Polyposis (FAP)<br />
• Fragile X Society (National)<br />
• Genetic Alliance UK (National)<br />
• Huntingdon’s Disease association, Nottingham<br />
• Muscular Dystrophy Campaign (National)<br />
• Nottingham Department of Clinical Genetics<br />
• Nottingham Sickle cell and thalassaemia service - Mary Potter Hostel, Hyson<br />
Green, Nottingham.<br />
• OSCAR Organisation for Sickle cell anaemia research<br />
• Sickle Cell and Thalassaemia Centre – Charnwood Health Centre, Leicester<br />
• The Haemophilia Society<br />
• The National Childbirth Trust (sent 12/07/10 – extended deadline for<br />
comments to 20/07/10)<br />
90
• The Sickle Cell Society (national) (sent 12/07/10 – extended deadline for<br />
comments to 20/07/10)<br />
• Twins and Multiple Births Association (TAMBA)<br />
• UK Thalassaemia Society<br />
Other networks/interest groups:<br />
• CARE Nottingham<br />
• Community specialist nurses for the sickle cell and thalassaemia service in<br />
Nottingham and Leicester.<br />
• Derby City General Hospital Haematology Department<br />
• East Midlands Directors of Public Health (DPHs).<br />
• East Midlands Genetic Network Group<br />
• East Midlands Specialised Commissioning Group (EMSCG) lay<br />
representatives<br />
• Embryologist and Director, CARE Fertility Nottingham<br />
• Embryologist and molecular geneticist. Genesis Genetics, Nottingham<br />
• Equality and Diversity leads within the 9 East Midlands Primary Care Trusts<br />
(<strong>PCT</strong>s).<br />
• Human Genetics Commission<br />
• Individual Funding Request (IFR) Managers within the East Midlands <strong>PCT</strong>s<br />
• Individual Local Involvement Networks (LINks) leads within the East Midlands.<br />
• LINks lead for the East Midlands.<br />
• Members of the East Midlands Clinical Priorities Advisory Group (CPAG)<br />
• East Midlands Public Health Consultants* (3<br />
• PPI/EMSCG liaison leads in the 9 East Midlands Primary Care Trusts (<strong>PCT</strong>s).<br />
• Primary Care Trust Chief Executives<br />
• Primary Care Trust Contract managers<br />
• Provider (Trust) Chief Executives * (NGH<br />
• The East Midlands (EM) cancer network.<br />
References<br />
Department for Business, Innovation and Skills (BIS) (2010) ‘Producing a Summary<br />
of Responses’. Available from http://www.bis.gov.uk/policies/betterregulation/consultation-guidance/summary-of-responses.<br />
Accessed 14/04/2010.<br />
Human Fertilisation and Embryology Authority (HFEA), http://www.hfea.gov.uk/,<br />
accessed 17/08/2010.<br />
91
How to contact us<br />
NHS Leicester City<br />
St John's House<br />
30 East Street<br />
Leicester LE1 6NB<br />
For general enquiries: 0116 295 1400 (Mon-Fri 8.30am - 5pm)<br />
Email: enquiries@leicestercity.nhs.uk<br />
NHS Leicestershire County and Rutland<br />
Lakeside House, 4 Smith Way,<br />
Grove Park, Enderby,<br />
Leicester,<br />
LE19 1SS<br />
For general enquiries: 0116 295 7500 (Mon-Fri 9am - 5pm)<br />
Email: info@nhslcrmembership.org<br />
EMSCG<br />
EMSCG<br />
Fosse House<br />
6 Smith Way<br />
Grove Park, Enderby<br />
Leicester, LE19 1SX<br />
For general enquiries: 0116 295 0849<br />
Email: info@emscg.nhs.uk<br />
Customer Services<br />
Our joint Customer Services team handles complaints, Freedom of Information<br />
requests, and helps with queries from patients, carers and members of the public.<br />
Post: Customer Services, St John’s House, 30 East Street, Leicester, LE1 6NB<br />
Tel: 0116 295 7011 (Monday to Friday 9am to 5pm)<br />
Email: customerservices@leicestercity.nhs.uk or customerservices@lcr.nhs.uk<br />
NHS Leicester City Membership<br />
NHS Leicester City Membership scheme enables people from all sections of the<br />
community to participate in our work in a way that suits them. The main aims are:<br />
• to develop two-way communication between NHS Leicester City, patients,<br />
community and voluntary groups, and frontline staff<br />
• to keep members informed of developments in healthcare<br />
• to reflect the diversity of the local population<br />
• to recognise the knowledge and experience of Leicester residents and our staff<br />
92
Tel: 0116 295 4183 (9am to 5pm)<br />
Fax: 0116 295 1513<br />
Email: getinvolved@leicestercity.nhs.uk<br />
Post: Freepost RRUE JRBR RGGT, NHS Leicester City, St John's House,<br />
30 East Street, Leicester, LE1 6NB.<br />
NHS Leicestershire and Rutland Membership<br />
NHS Leicestershire County and Rutland has set up a scheme to enable us to work<br />
together to reach this aim and for you to have a say in how local NHS services are<br />
provided. It is called “Be Healthy, Be Heard”. We have a dedicated interactive<br />
website where you can access a wealth of information about the membership<br />
scheme, find out about the benefits of becoming a member, join online and much<br />
more.<br />
To join online, visit the website www.lcr.nhs.uk. Fill in the interactive form and submit<br />
it. If you would like to join by post please download and print the relevant form from<br />
the website, complete it and send it back to by post to:<br />
NHS Leicestershire County and Rutland (Membership), Lakeside House, 4 Smith<br />
Way, Grove Park, Enderby, Leicester, LE19 1SS<br />
LINks - Local Involvement Networks*<br />
Local Involvement Networks (LINks) are a network of people, organisations and<br />
groups who want to strengthen the quality of health and social care services.<br />
For Leicester LINk telephone: 0800 731 9432<br />
You can also write to Leicester LINk at:<br />
Freepost RSBR-AKKG-XAHC<br />
Leicester Link<br />
Unit 55 Business Box<br />
3 Oswin Road<br />
Leicester<br />
LE3 1HR<br />
Email: LeicesterLINks@carersfederation.co.uk<br />
For Leicestershire and Rutland LINk telephone: 0116 229 3103<br />
You can also write to Leicestershire LINk at:<br />
Beaumont Enterprise Centre<br />
Boston Road<br />
Leicester<br />
LE4 1HB<br />
Email: info@leicestershirelink.org.uk<br />
* Please note that all LINKs will transform into HealthWatch groups under the terms<br />
of the Health and Social Care Bill, subject to Parliamentary approval.<br />
93
Do you need help understanding this report?<br />
Our annual report can be provided in other languages<br />
and formats on request, including large print.<br />
If you require help understanding the contents of this<br />
leaflet, please telephone 0116 295 4743 for translation<br />
or other formats.<br />
94
NHS Leicester City<br />
St John's House<br />
30 East Street<br />
Leicester<br />
LE1 6NB<br />
NHS Leicestershire County and<br />
Rutland<br />
Lakeside House, 4 Smith Way,<br />
Grove Park, Enderby,<br />
Leicester,<br />
LE19 1SS